myocarditis
Reading File
Finding Sources
Searching PubMed
myocarditis diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough, well-cited response.
Myocarditis
Definition
Myocarditis is an inflammatory process involving the myocardium, defined histologically by the presence of myocyte injury (degeneration or necrosis) and an inflammatory infiltrate not due to ischemia. It encompasses a diverse group of clinical entities in which infectious agents and/or inflammatory processes target the myocardium. The clinical spectrum ranges from asymptomatic ECG abnormalities to hemodynamic collapse and sudden death.
- Goldman-Cecil Medicine, p. 511
- Robbins Basic Pathology, p. 375
Epidemiology
-
Prevalence estimates range from 1 in 100,000 to 1 in 10,000
-
Postmortem studies report myocarditis in up to 12% of young victims of sudden cardiac death
-
Some degree of myocarditis is detected in nearly 10% of routine autopsies but is often clinically unrecognized
-
Up to 5% of patients with acute viral illness may exhibit a form of myocarditis
-
Linked to the development of dilated cardiomyopathy (DCM) in up to 16% of adult cases and 46% in children
-
Rosen's Emergency Medicine, p. 1119
-
Goldman-Cecil Medicine, p. 511
Etiology
Causes span the full microbial spectrum plus immune-mediated and toxic insults:
Infectious
| Category | Key Organisms |
|---|---|
| Viral (most common in the West) | Coxsackievirus A & B, enteroviruses, parvovirus B19, HHV-6, adenovirus, HIV, CMV, influenza, SARS-CoV-2, EBV, hepatitis C |
| Protozoal | Trypanosoma cruzi (Chagas - most common worldwide), Toxoplasma gondii |
| Bacterial | Borrelia burgdorferi (Lyme), Corynebacterium diphtheriae, Mycoplasma pneumoniae, Salmonella, Neisseria spp. |
| Spirochetal | Treponema pallidum, Borrelia, Leptospira |
| Fungal | Aspergillus, Candida, Cryptococcus |
| Parasitic | Trichinella spiralis (most common helminthic cardiac disease), Echinococcus |
| Rickettsial | Coxiella burnetii, Rickettsia rickettsii |
Immune-mediated
- Systemic lupus erythematosus, systemic sclerosis, polymyositis/dermatomyositis
- Sarcoidosis, eosinophilic granulomatosis with polyangiitis (Churg-Strauss)
- Giant cell myocarditis, Kawasaki disease, heart transplant rejection
- Hypersensitivity reactions (penicillin, sulfonamides, methyldopa, tricyclic antidepressants, thiazide diuretics)
- Immune checkpoint inhibitor therapy
Toxic
- Anthracyclines, cocaine, amphetamines, cyclophosphamide
- Heavy metals (copper, iron, lead), arsenic, carbon monoxide
- Physical agents: radiation, electric shock, hyperpyrexia
Vaccine-related
-
mRNA COVID-19 vaccines: rare cases, predominantly in male adolescents and young adults, most often after the second dose, usually within 1 week. Most recover uneventfully. Estimated excess incidence ~1-10 per million persons after mRNA vaccines.
-
Goldman-Cecil Medicine, pp. 511-512
-
Robbins Basic Pathology, p. 375
-
Rosen's Emergency Medicine, p. 1119
Pathogenesis
Viral myocarditis is best understood and follows three phases:
- Acute (cytotoxic) phase: Direct viral invasion with cytotoxicity, focal necrosis
- Subacute phase: Increase in humoral factors leading to autoimmune injury. The host antiviral immune response that initially limits viral damage, when prolonged, causes inflammatory damage. Viruses can trigger an immune reaction that cross-reacts with myocardial proteins such as myosin heavy chain (molecular mimicry)
- Chronic phase: Diffuse myocardial fibrosis and cardiac dysfunction, potentially leading to DCM
A breakdown of T-cell tolerance can produce chronic inflammation. Anti-beta-myosin antibodies are found in higher concentrations in patients with myocarditis and DCM compared to controls, supporting a predominantly autoimmune mechanism in idiopathic DCM following myocarditis.
For non-viral causes: Trypanosoma cruzi causes 10% mortality in the acute phase; survivors may enter a chronic immune-mediated phase with CHF and arrhythmias 10-20 years later (20-30% of patients with chronic Chagas disease develop cardiac disease).
- Rosen's Emergency Medicine, p. 1119
- Robbins Basic Pathology, pp. 374-375
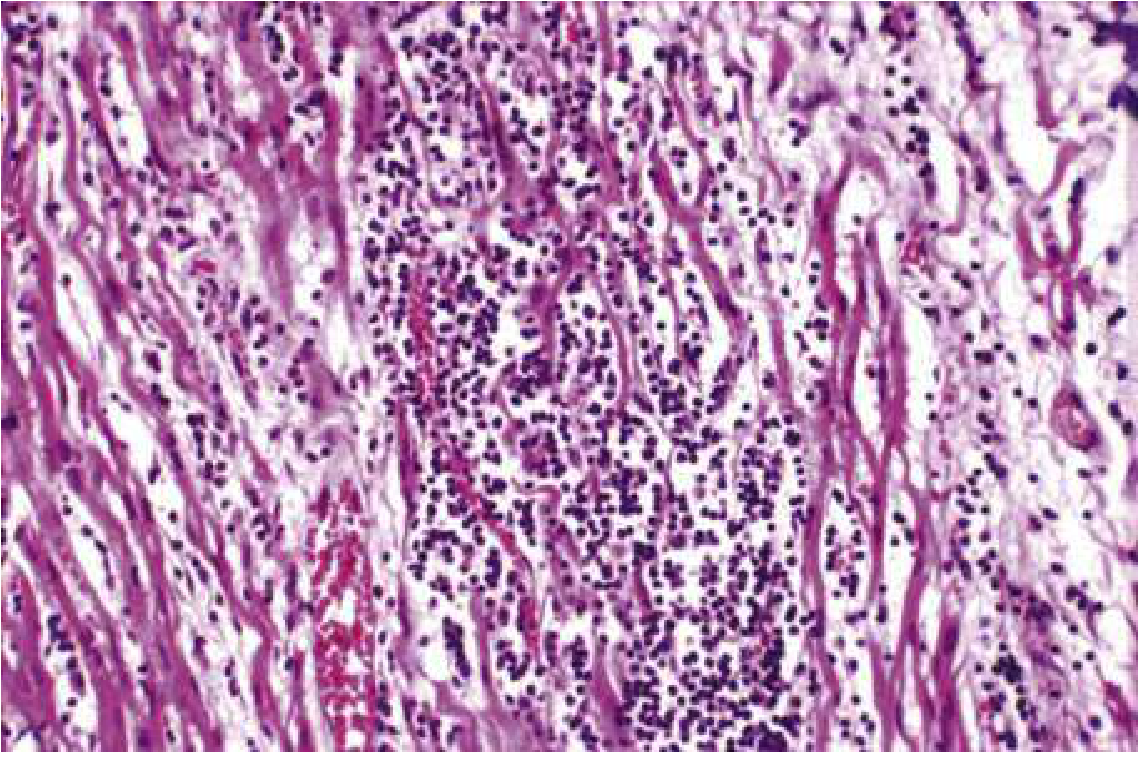
Morphology / Histopathology
Gross: In acute myocarditis, the heart may appear normal or dilated. In advanced stages the myocardium is typically flabby and mottled with pale and hemorrhagic areas. Mural thrombi may be present.
Microscopy:
- Viral myocarditis: Edema, interstitial inflammatory infiltrates (predominantly lymphocytic), and myocyte injury. Inflammatory involvement is often patchy.
- Hypersensitivity myocarditis: Interstitial and perivascular infiltrates composed of lymphocytes, macrophages, and a high proportion of eosinophils
- SLE myocarditis: Small focal areas of fibrinoid necrosis with lymphocyte and plasma cell infiltration; immune complex deposition around myocyte bundles; granular complement staining on immunofluorescence
If the patient survives the acute phase, lesions may resolve without significant sequelae or heal by fibrosis (substrate for future arrhythmia via scar-related reentry).
The Dallas criteria remain the historical standard for biopsy diagnosis - requiring the combination of leukocyte infiltration and necrosis. Four histologic patterns are recognized:
- Active myocarditis - myocyte degeneration/necrosis + definite cellular infiltrate ± fibrosis
- Borderline myocarditis - cellular infiltrate without myocyte injury
- Persistent myocarditis - continued infiltration
- Healed myocarditis - scarring without active infiltrate
Molecular analysis (DNA/RNA extraction + PCR) of biopsy specimens substantially refines diagnosis.
- Robbins Basic Pathology, p. 375
- Goldman-Cecil Medicine, p. 511
- Grainger & Allison's Diagnostic Radiology, p. 331
Clinical Features
The presentation is highly variable:
Prodrome: Flu-like symptoms - fever, fatigue, myalgias, vomiting, diarrhea (reflecting the preceding viral illness)
Common presentations in adults:
- Dyspnea, chest pain (can mimic ACS), palpitations
- New-onset heart failure or unexplained arrhythmias in an otherwise healthy patient
Presentation in children:
- Dyspnea is most common
- Infants may present with a fulminant syndrome: fever, cyanosis, respiratory distress, tachycardia, cardiac failure
Red flags for poor outcome:
- Severe dyspnea, heart failure, hemodynamic instability at presentation
- Ventricular dysrhythmias
Giant cell myocarditis - a particularly severe variant (10-20% of biopsy-positive cases): rapid onset of chest pain, fever, and hemodynamic compromise, often with ventricular tachycardia or AV block.
- Rosen's Emergency Medicine, p. 1119
- Goldman-Cecil Medicine, p. 512
Diagnostic Testing
ECG
- Sinus tachycardia (most common)
- Widened QRS, low voltages, prolonged QT interval
- ST/T-wave changes (nonspecific)
- AV block or complete heart block (especially Lyme myocarditis)
- AMI pattern - may extend beyond distribution of a single coronary artery
- Supraventricular or ventricular tachycardias; PVCs often originating from the inferior LV (RBBB superior axis morphology in lymphocytic myocarditis)
Biomarkers
- Troponin I/T: May be elevated; a negative serial troponin does not exclude the diagnosis
- ESR, CRP, WBC: Of no independent diagnostic value
- In SLE myocarditis: raised ESR, increased anti-dsDNA titers, complement consumption
Echocardiography
- Reduced LV ejection fraction, global hypokinesis
- Regional wall motion abnormalities not following coronary artery anatomy
- Possible pericardial effusion
- May be relatively unremarkable in mild cases
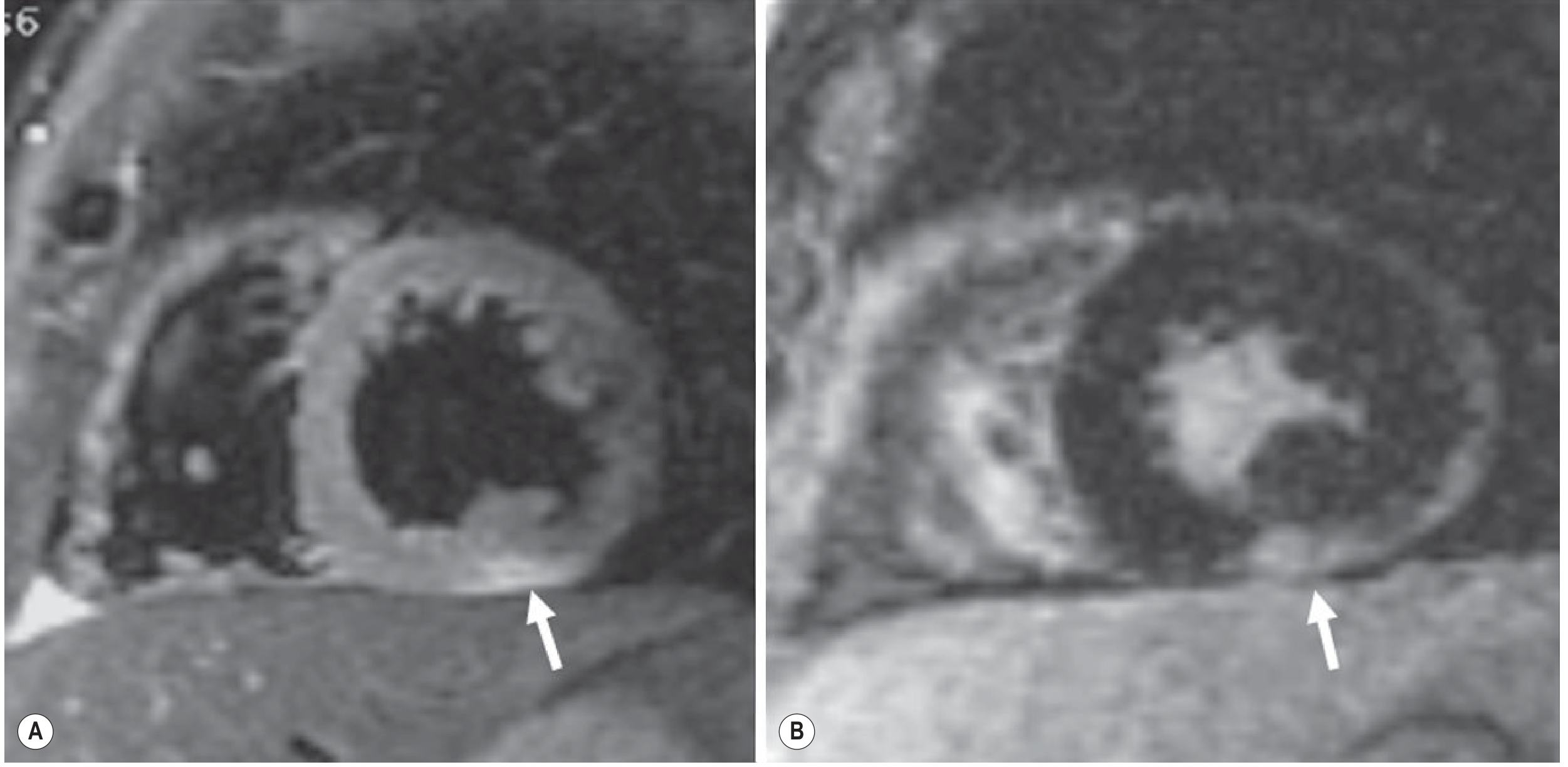
Cardiac MRI (modality of choice for non-invasive diagnosis)
The Lake Louise Criteria use a combination of:
- T2-weighted sequences (STIR): Myocardial edema - subepicardial or mid-wall hyperintensity
- Early gadolinium enhancement: Inflammatory hyperemia
- Late gadolinium enhancement (LGE): Subepicardial non-ischemic distribution, most frequently in the lateral and/or inferior wall
Key CMR points:
- LGE in myocarditis is subepicardial, distinguishing it from STEMI (subendocardial/transmural LGE) and takotsubo (typically absent LGE)
- A negative LGE study does NOT exclude acute myocarditis - early enhancement imaging is needed to detect inflammatory hyperemia without macroscopic necrosis
- Septal, mid-wall, and patchy LGE distribution is associated with increased risk of sudden death
Coronary Angiography
- Indicated when the presentation mimics ACS to exclude obstructive coronary artery disease
- Typically shows normal arteries in myocarditis
Endomyocardial Biopsy
-
Histologic gold standard, but has variable sensitivity due to sampling error (patchy inflammation)
-
Sensitivity can be increased by MRI-guided targeting of abnormal regions
-
Indications: Suspected giant cell myocarditis (young person with rapidly progressive heart failure + ventricular tachyarrhythmias or AV block), or when the diagnosis would change management
-
Not routinely used due to invasive nature and variable sensitivity
-
Grainger & Allison's Diagnostic Radiology, pp. 330-332
-
Rosen's Emergency Medicine, p. 1120
-
Goldman-Cecil Medicine, p. 511
Management
Acute Supportive Care
- Activity restriction (complete rest; avoid strenuous exertion during active inflammation)
- Afterload reduction and diuresis
- Standard heart failure therapy: ACE inhibitors, diuretics, beta-blockers, anticoagulants (per heart failure guidelines)
- Rhythm management for arrhythmias
Fulminant Myocarditis
- Inotropic support
- Mechanical circulatory support (ventricular assist devices)
- ECMO (extracorporeal membrane oxygenation)
- Cardiac transplantation for refractory cases
Immunosuppression
The role is uncertain in viral lymphocytic myocarditis:
- A landmark RCT of 111 adults with biopsy-proven myocarditis showed no difference in mortality or LV function improvement with prednisolone + cyclosporine or azathioprine vs placebo
- A subsequent trial using MHC expression on biopsy to select patients showed improved LVEF with prednisolone + azathioprine, but no mortality benefit at 2-year follow-up
Immunosuppression is indicated for:
-
Giant cell myocarditis (benefits established)
-
Eosinophilic myocarditis
-
Cardiac sarcoidosis
-
Biopsy-proven, infection-negative immune-mediated myocarditis refractory to conventional heart failure therapy
-
SLE-related myocarditis, polymyositis/dermatomyositis-related myocarditis
-
Goldman-Cecil Medicine, pp. 512-513
-
Rosen's Emergency Medicine, p. 1120
-
Braunwald's Heart Disease, p. 565
Prognosis and Complications
-
Most patients with acute viral myocarditis recover without sequelae
-
Residual myocardial fibrosis (detectable as LGE on CMR) can serve as a persistent substrate for scar-related reentrant VT and sudden cardiac death
-
Progression to dilated cardiomyopathy occurs in a significant subset (up to 16% of adults, 46% of children)
-
Long-term prognosis in children correlates with severity of initial presentation
-
Chagas disease: 20-30% of patients develop cardiac disease with CHF, aneurysms, and VT over decades; sudden death may be the first manifestation
-
Giant cell myocarditis has the worst prognosis among the histologic subtypes
-
Braunwald's Heart Disease, p. 565
-
Rosen's Emergency Medicine, p. 1120
Special Situations
SARS-CoV-2 / COVID-19
Myocarditis is a rare complication with an apparent excess incidence of ~40 extra events per million persons. The risk from infection appears to exceed the risk from mRNA vaccination. Vaccine-associated myocarditis risk is highest under age 40 and more pronounced after the second mRNA dose.
Lyme Myocarditis
Occurs in ~5% of patients with Lyme disease. Manifests primarily as self-limited conduction system disease - classically high-degree AV block, frequently requiring temporary pacemaker insertion. Managed with antibiotics.
Peripartum Myocarditis
Autoimmune in nature; myocarditis may be an initial feature of rheumatic diseases requiring consideration in the differential of unexplained heart failure.
Sources:
- Robbins & Kumar Basic Pathology, 10e
- Goldman-Cecil Medicine, International Edition
- Braunwald's Heart Disease, 12e
- Rosen's Emergency Medicine, 10e
- Grainger & Allison's Diagnostic Radiology, 7e
- Braunwald's Heart Disease (Rheumatic Disease chapter)
This is a shared conversation. Sign in to Orris to start your own chat.