Inguinal canal anatomy. Anatomy of the abdomen
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks with excellent anatomical images. Let me compile the full answer.
Inguinal Canal Anatomy and Anatomy of the Abdomen
I. ANATOMY OF THE ABDOMEN
Layers of the Anterior Abdominal Wall
The anterior abdominal wall is a multi-layered structure whose components work together for organ protection, posture, and respiration. From superficial to deep, the layers are:
- Skin
- Superficial fascia - has a superficial fatty layer (Camper's fascia) and a deep membranous layer (Scarpa's fascia)
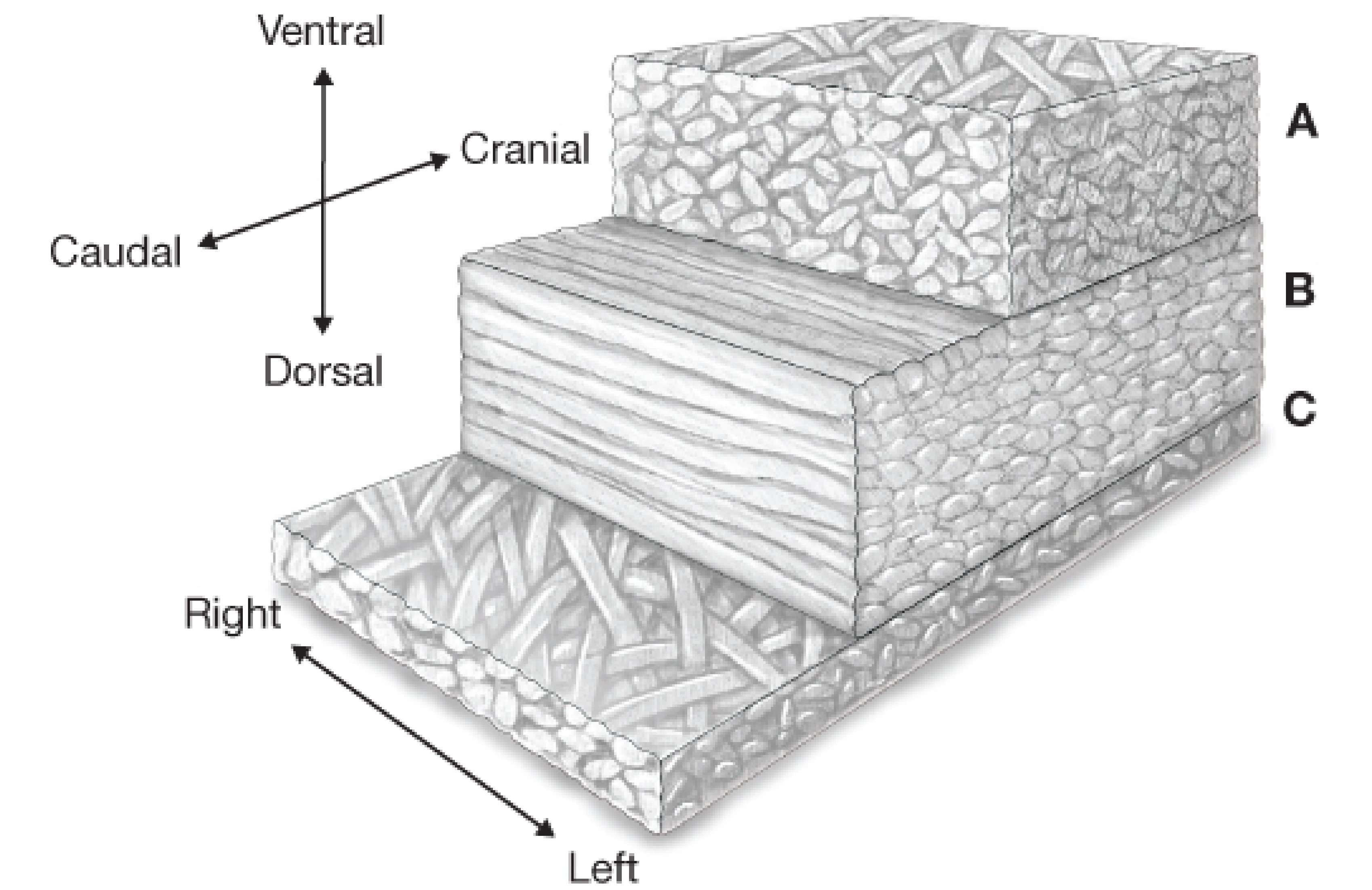
- External oblique muscle / aponeurosis - fibers run downward and medially (like hands in pockets)
- Internal oblique muscle - fibers run upward and medially (perpendicular to external oblique)
- Transversus abdominis muscle - fibers run horizontally
- Transversalis fascia - thin but important fascial layer lining the inner surface
- Extraperitoneal fat
- Peritoneum (parietal)
The abdominal core musculature includes muscle groups and aponeuroses connected to the lumbar vertebrae posteriorly, the thorax superiorly, and the pelvis at the base. The base of this "canister" is the pelvic floor and the top is the diaphragm. - Fischer's Mastery of Surgery, p. 5984
Rectus Sheath
- Two rectus abdominis muscles run vertically on either side of the midline, separated by the linea alba
- The rectus sheath is formed by the aponeuroses of the three flat muscles:
- Above the arcuate line: anterior sheath = external oblique + anterior lamina of internal oblique; posterior sheath = posterior lamina of internal oblique + transversus abdominis
- Below the arcuate line (Douglas's line): all three aponeuroses pass anterior to rectus abdominis, leaving only transversalis fascia behind it
Blood Supply
The abdominal wall has a dual blood supply:
- Superior epigastric artery (from internal thoracic artery) - runs in the rectus sheath superiorly
- Inferior epigastric artery (from external iliac artery) - enters the rectus sheath below the arcuate line, lying just medial to the deep inguinal ring
- Lateral wall: deep circumflex iliac and lower intercostal/subcostal vessels
Internal Surface of the Anterior Abdominal Wall
Five peritoneal folds radiate toward the umbilicus from below, creating potential hernia sites:
| Fold | Contents |
|---|---|
| Median umbilical fold (unpaired) | Obliterated urachus |
| Medial umbilical folds (paired) | Obliterated umbilical arteries |
| Lateral umbilical folds (paired) | Inferior epigastric vessels |
Between these folds lie three fossae on each side:
- Supravesical fossa - between median and medial umbilical folds
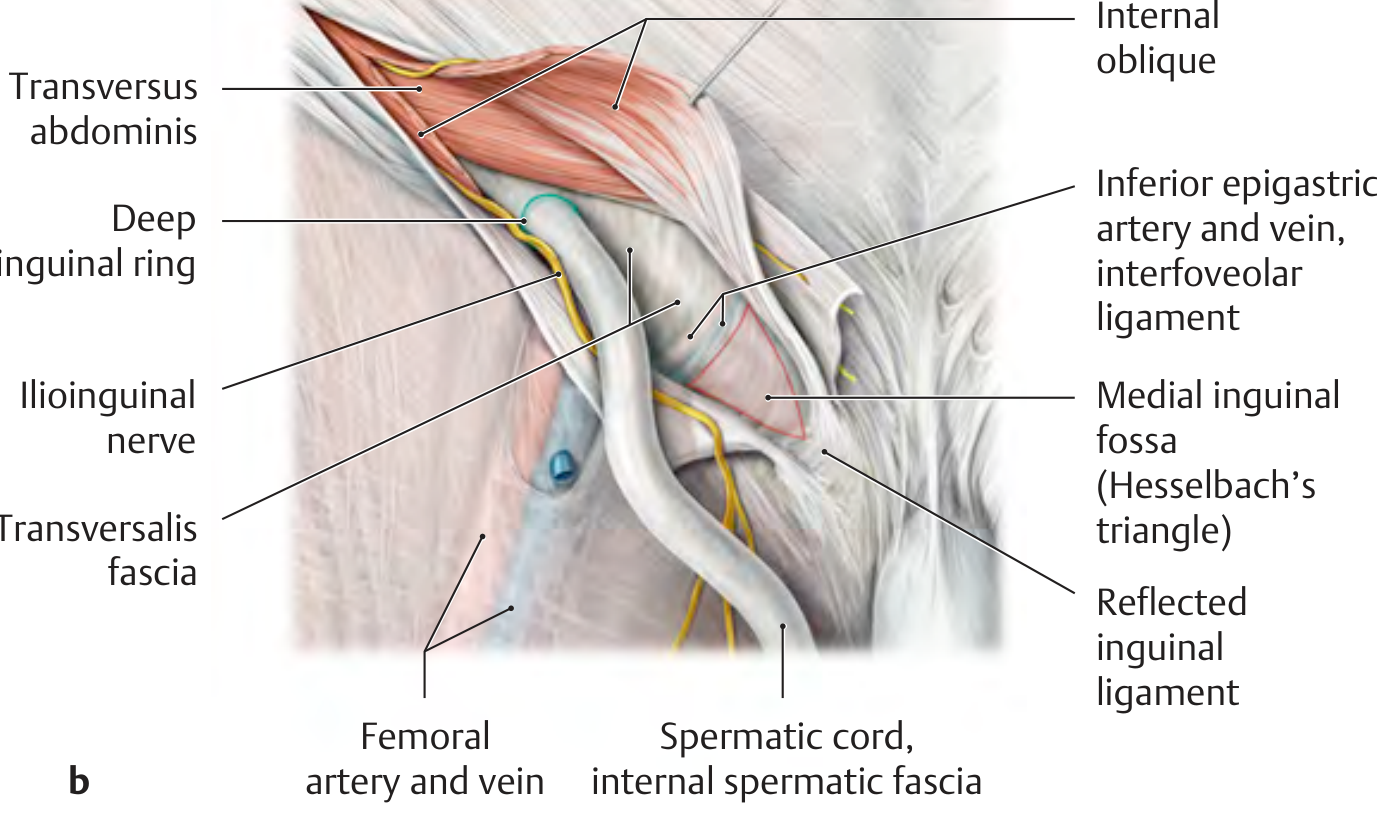
- Medial inguinal fossa (= Hesselbach's triangle) - between medial and lateral folds
- Lateral inguinal fossa - lateral to the lateral fold; site of the deep inguinal ring
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
II. THE INGUINAL CANAL
Overview
The inguinal canal is an oblique passage approximately 4-6 cm long in adults, running forward, downward, and medially above the inguinal ligament. It pierces the anterior abdominal wall and connects the internal ring to the external ring. - THIEME Atlas of Anatomy
It provides the pathway for testicular descent during fetal development, and in adults it transmits:
- Males: spermatic cord
- Females: round ligament of the uterus
- Both sexes: ilioinguinal nerve and lymphatics
The Two Openings (Rings)
Deep (Internal) Inguinal Ring
- An opening in the transversalis fascia
- Located midway between the anterior superior iliac spine (ASIS) and the pubic tubercle, approximately 2-3 cm above the femoral artery pulse
- Lies in the lateral inguinal fossa
- The inferior epigastric vessels lie just medial to it
- Bounded by: the interfoveolar ligament, inguinal ligament, and lateral umbilical fold
- The transversalis fascia is invaginated here into the inguinal canal to form the internal spermatic fascia around the cord
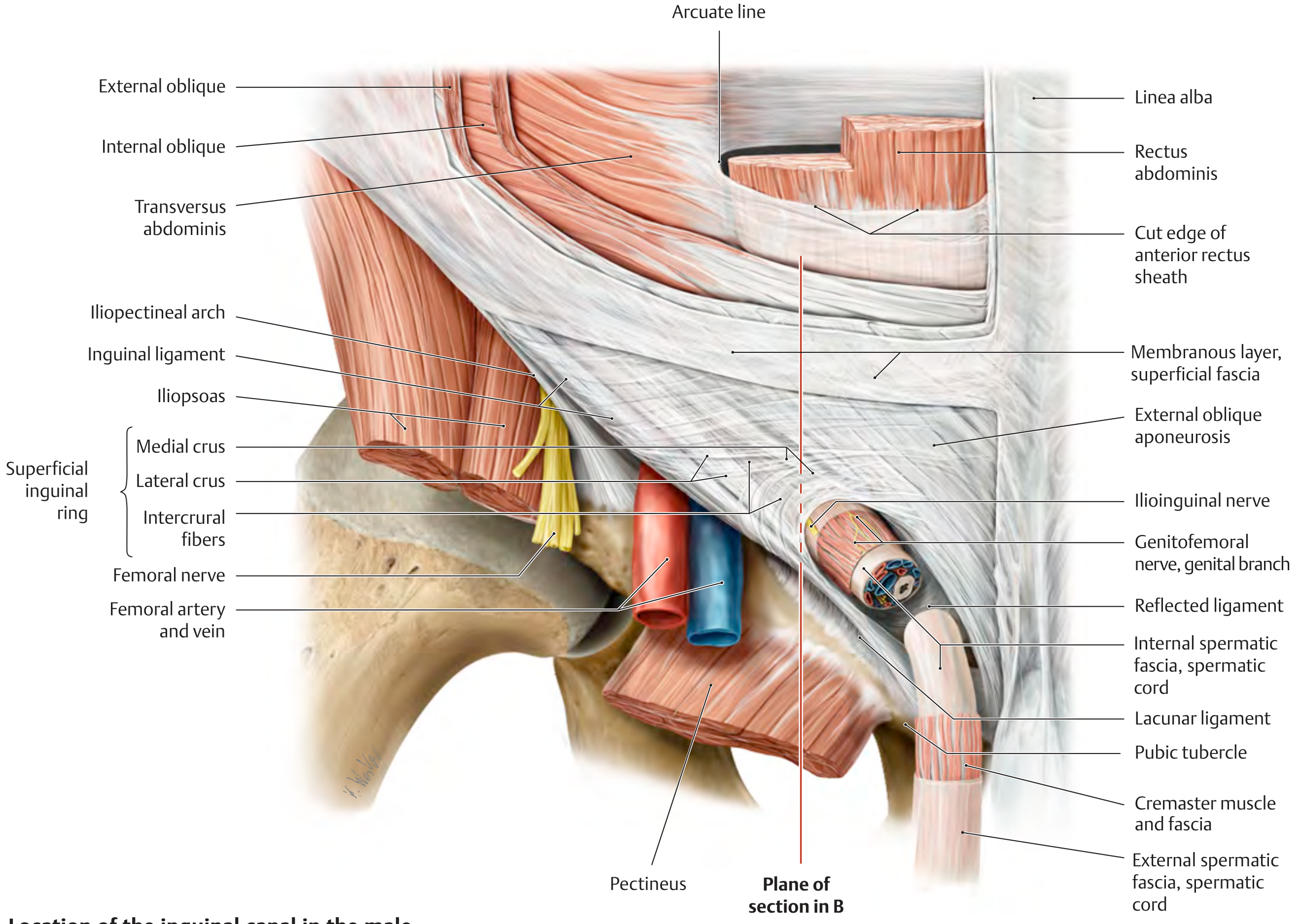
Superficial (External) Inguinal Ring
- An inverted V-shaped (slit-like) defect in the external oblique aponeurosis
- Located lateral to the pubic tubercle
- Bounded by:
- Medial crus (superomedially)
- Lateral crus (inferolaterally)
- Intercrural fibers (superiorly, connecting the crura)
- Reflected inguinal ligament (inferiorly, completing it internally)
Walls of the Inguinal Canal
| Wall | Structure |
|---|---|
| Anterior wall | External oblique aponeurosis (+ internal oblique in the lateral third) |
| Posterior wall | Transversalis fascia + peritoneum (reinforced medially by interfoveolar ligament and reflected inguinal ligament) |
| Roof | Arching fibers of transversus abdominis and internal oblique |
| Floor | Inguinal ligament (the thickened, inrolled free inferior edge of the external oblique aponeurosis = Poupart's ligament) |
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1087
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
The Conjoint Tendon
Muscle fibers of the transversus abdominis and the internal oblique arch over the deep inguinal ring from lateral to medial, then descend to attach to the pubic tubercle and crest. As they fuse and become tendinous, they form the conjoint tendon (inguinal falx). This tendon forms the roof of the inguinal canal and reinforces the medial posterior wall. Below the arch, where no muscle covers the posterior wall, only transversalis fascia and external oblique aponeurosis are present - this creates the area of weakness exploited in hernias. - Bailey and Love's
Contents of the Inguinal Canal
Males:
- Vas deferens (ductus deferens)
- Testicular artery
- Pampiniform plexus of veins (become the testicular vein)
- Lymphatics from the testis
- Cremaster muscle (from internal oblique)
- Genital branch of the genitofemoral nerve
- Ilioinguinal nerve (runs on the cord's anterior surface)
All covered by three fascial layers: external spermatic fascia (from external oblique), cremasteric fascia, and internal spermatic fascia (from transversalis fascia).
Females:
- Round ligament of the uterus (ends in the labia majora)
- Ilioinguinal nerve
- Lymphatics
Key Nerves in the Region
| Nerve | Course |
|---|---|
| Ilioinguinal nerve (L1) | Runs through the inguinal canal on the spermatic cord; exits the superficial ring to supply skin over pubic symphysis, medial scrotum/labia majora, and medial thigh |
| Genital branch of genitofemoral nerve (L1-L2) | Runs with the spermatic cord below cremasteric fascia; supplies cremaster muscle and sensation to scrotal skin |
| Iliohypogastric nerve (L1) | Runs above the inguinal canal; supplies skin above the inguinal ligament |
Hesselbach's Triangle (Medial Inguinal Fossa)
The triangle of weakness in the posterior wall, bounded by:
- Lateral: Inferior epigastric vessels
- Medial: Lateral edge of rectus abdominis
- Inferior: Inguinal ligament (iliopubic tract)
This area is covered only by transversalis fascia and external oblique aponeurosis - no muscle reinforcement. It is the site of direct inguinal hernias. - Bailey and Love's, p. 1088
Clinical Anatomy: Hernia Types

| Feature | Indirect (Lateral) | Direct (Medial) | Femoral |
|---|---|---|---|
| Origin | Lateral inguinal fossa → deep ring | Medial inguinal fossa (Hesselbach's) | Below inguinal ligament, femoral ring |
| Relation to inferior epigastric vessels | Lateral | Medial | Below |
| Mechanism | Congenital (processus vaginalis) or acquired | Always acquired | Acquired |
| Can reach scrotum? | Yes | No | No |
| Strangulation risk | Higher (narrow ring) | Lower (broad base) | Highest (sharp lacunar ligament) |
| External opening | Superficial inguinal ring | Superficial inguinal ring | Saphenous opening |
The table from the THIEME Atlas summarizes hernia fossae:
| Hernia | Internal opening | External opening |
|---|---|---|
| Direct inguinal | Medial inguinal fossa (Hesselbach's) | Superficial inguinal ring |
| Indirect inguinal | Lateral inguinal fossa (deep ring) | Superficial inguinal ring |
| Femoral | Femoral ring (below inguinal ligament) | Saphenous opening |
Processus Vaginalis and Its Clinical Significance
As the testis descends, it carries a tube of peritoneum - the processus vaginalis - which wraps around it to form the tunica vaginalis. This should obliterate after birth. If it remains patent:
- Complete patency → indirect inguinal hernia
- Partial obliteration → hydrocele of the cord
- Obliteration at the testis only → communicating hydrocele
Inguinal hernias in neonates and children are almost always of this congenital (indirect) type. - Bailey and Love's, p. 1088
Summary Memory Aid
"My External Oblique And Transversalis Keeps Contents Right"
- Anterior = External oblique aponeurosis
- Posterior = Transversalis fascia
- Roof = Conjoint tendon (Int. oblique + Transversus)
- Floor = Inguinal ligament (= Poupart's ligament)
Deep ring = in transversalis fascia, lateral to inferior epigastrics Superficial ring = in external oblique aponeurosis, lateral to pubic tubercle
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System | Fischer's Mastery of Surgery 8th Ed. | Gray's Anatomy for Students | Campbell-Walsh-Wein Urology
Sebaceous cyst anatomy, skin anatomy
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full detailed answer.
Skin Anatomy and Sebaceous Cysts
I. SKIN ANATOMY
The skin (cutis / integument) is the largest organ of the body, with a surface area of approximately 1.8 m² and constituting 15-20% of total body mass. It has three main layers: epidermis, dermis, and hypodermis (subcutaneous tissue). - Histology: A Text and Atlas (Eroschenko), p. 1279
Functions of the Skin
| Function | Mechanism |
|---|---|
| Physical barrier | Mechanical, permeability, and UV protection |
| Immune surveillance | Langerhans cells process antigens |
| Thermoregulation | Sweat glands + cutaneous blood flow |
| Sensory | Mechanoreceptors, thermoreceptors, nociceptors |
| Endocrine | Vitamin D3 synthesis; secretion of cytokines and hormones |
| Excretion | Sweat, sebaceous, and apocrine gland secretion |
Thick vs. Thin Skin
| Thick Skin | Thin Skin | |
|---|---|---|
| Location | Palms and soles | Rest of the body |
| Epidermal layers | 5 (including stratum lucidum) | 4 |
| Hair follicles | Absent | Present |
| Stratum corneum | Extremely thick | Thinner |
Note: "Thick skin" and "thin skin" refer histologically to epidermal thickness only. The anatomically thickest skin (by dermis) is the upper back. - Histology: A Text and Atlas, p. 1281
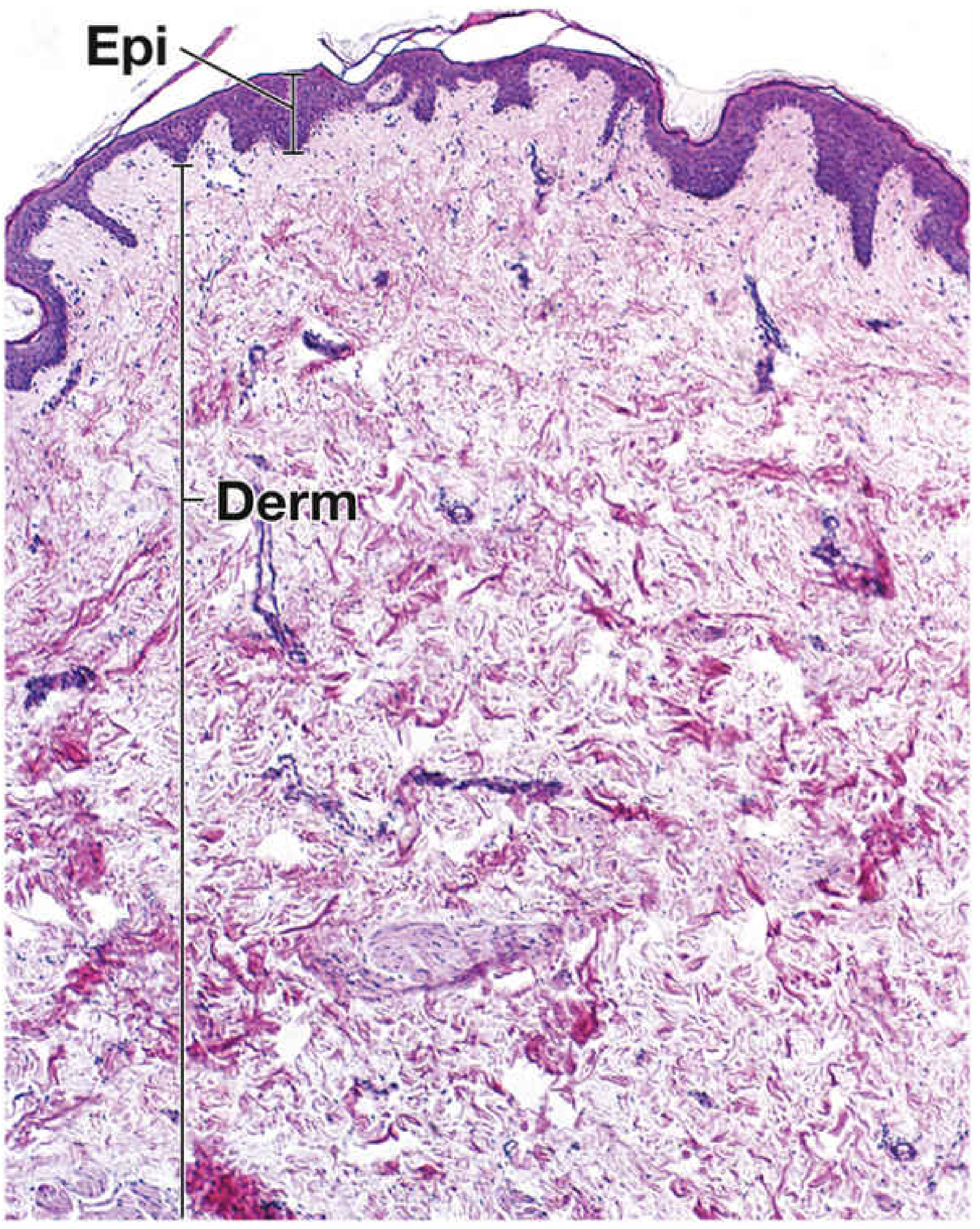
Layer 1: EPIDERMIS
The epidermis is a keratinized stratified squamous epithelium derived from ectoderm. It ranges from 0.05 to 1.5 mm in thickness. It contains no blood vessels - nutrition comes by diffusion from the dermis.
The 5 Layers of the Epidermis (deep to superficial)
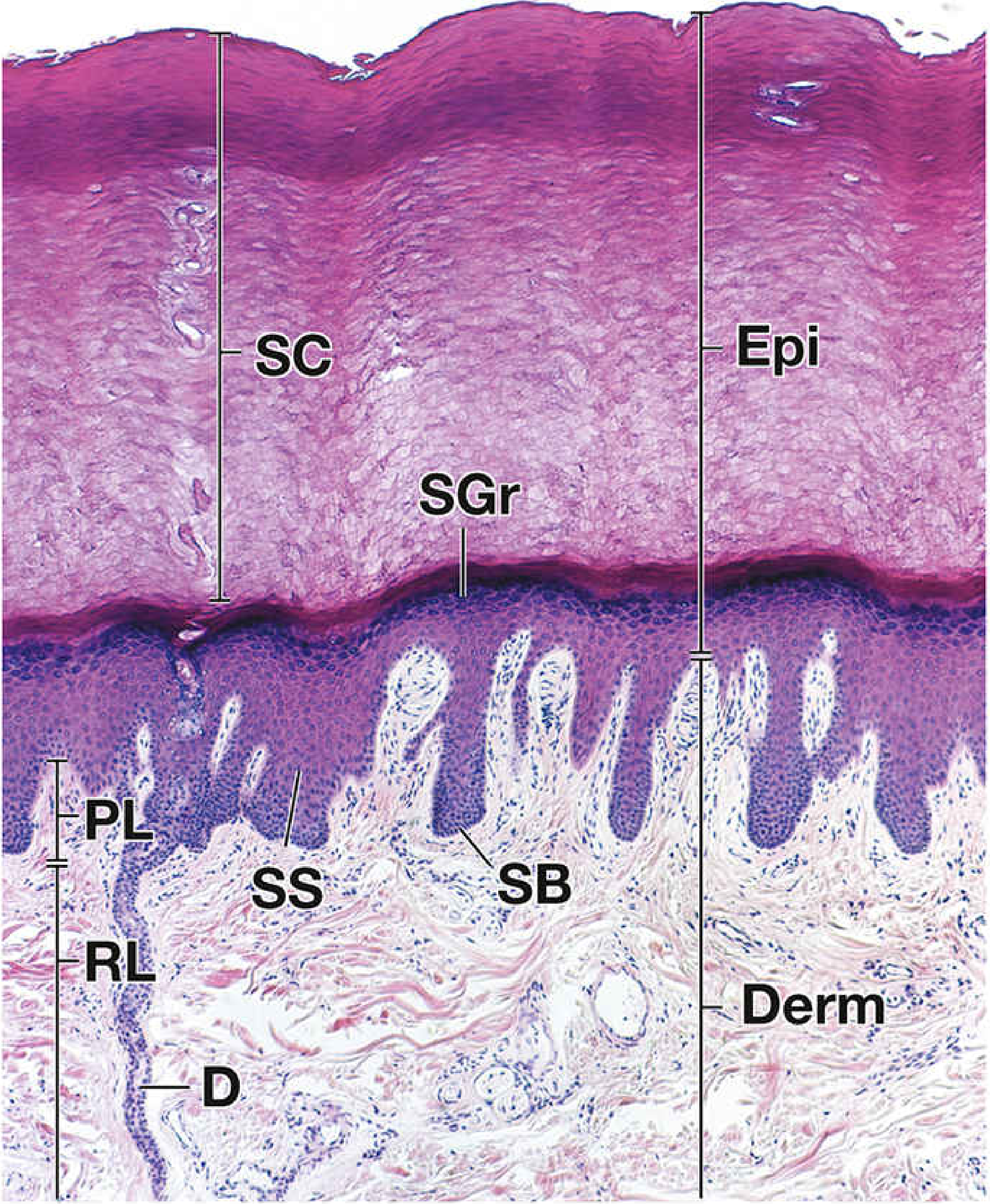
1. Stratum Basale (Germinativum) - deepest
- Single layer of cuboidal to low columnar cells resting on the basal lamina
- Contains stem cells (keratinocytes) that divide mitotically - the regenerative layer
- Also contains melanocytes interspersed between basal cells
- Cells connected to basal lamina by hemidesmosomes and to each other by desmosomes
- Basophilic cytoplasm due to abundant ribosomes
2. Stratum Spinosum (Prickle Cell Layer)
- Several cells thick; cells are larger and more polygonal
- Named for the numerous short "spines" (cytoplasmic processes connected by desmosomes) visible on light microscopy
- Cells contain tonofilaments (keratin intermediate filaments) bundled into tonofibrils
- Upper spinosum begins producing keratohyalin granules and lamellar bodies
3. Stratum Granulosum
- 3-5 layers of flattened cells containing prominent keratohyalin granules (dark purple on H&E)
- Cells discharge lamellar bodies into the intercellular space - these create the water permeability barrier
- Cells exhibit apoptotic nuclear morphology; nucleus begins to degrade
- pH here is approximately neutral (pH 7.17)
4. Stratum Lucidum (thick skin only)
- Thin, glassy, translucent zone between the granulosum and corneum
- Only present in palm and sole skin
5. Stratum Corneum - most superficial
- 15-20 layers (up to hundreds in thick skin) of dead, anucleate, keratinized cells (corneocytes)
- Cells filled with soft keratin bundled in a protein matrix
- pH is acidic (4.5-6.0) - allows kallikrein (KLK) serine peptidases to digest desmosomes, causing desquamation
- Provides the main barrier against desiccation and infection
Keratinocyte lifecycle: Stem cell divides in stratum basale → migrates upward → synthesizes keratin → forms lamellar bodies in spinosum → discharges water barrier lipids in granulosum → nucleus and organelles degrade → becomes dead corneocyte → desquamates at surface. Total transit time: ~2-4 weeks. - Histology: A Text and Atlas, p. 1285-1293
Non-Keratinocyte Cells of the Epidermis
| Cell | Location | Function |
|---|---|---|
| Melanocytes | Stratum basale | Produce melanin (eumelanin - brown/black; pheomelanin - red/yellow) via tyrosinase acting on L-tyrosine; donate melanosomes to keratinocytes via dendritic processes |
| Langerhans cells | Stratum spinosum | Antigen-presenting cells; initiate cutaneous hypersensitivity reactions (contact dermatitis) |
| Merkel cells | Stratum basale | Mechanoreceptors (light touch / pressure) |
Layer 2: DERMIS
The dermis is composed of dense irregular connective tissue derived from mesoderm. It is connected to the epidermis via the basement membrane and is the structural backbone of skin. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Two Sublayers
| Papillary Dermis | Reticular Dermis | |
|---|---|---|
| Position | Superficial, adjacent to epidermis | Deep, thicker layer |
| Connective tissue | Loose; thin collagen fibers | Dense; thick collagen bundles |
| Cellularity | More cellular | Less cellular |
| Vascular | Capillary loops entering dermal papillae | Larger vessels; vascular plexuses |
Dermal Contents
- Hair follicles with attached arrector pili muscles
- Sweat glands (eccrine and apocrine)
- Sebaceous glands
- Blood vessels arranged in superficial and deep plexuses
- Sensory receptors: Meissner's corpuscles (papillary dermis, fine touch), Pacinian corpuscles (reticular/hypodermis, deep pressure/vibration), Ruffini endings, free nerve endings
- Lymphatics
- Fibroblasts, mast cells, macrophages
The dermis is connected to the epidermis by the dermoepidermal junction (DEJ), which is interdigitated: epidermal downgrowths form rete ridges (interpapillary pegs) that interlock with connective tissue dermal papillae. This increases surface area and resistance to shear. - Histology: A Text and Atlas, p. 1282-1284
Layer 3: HYPODERMIS (Subcutaneous Tissue)
- Lies deep to the dermis; equivalent to the subcutaneous fascia of gross anatomy
- Contains variable amounts of adipose tissue in lobules separated by connective tissue septa
- Also contains deeper portions of hair follicles, sensory receptors (Pacinian corpuscles), neurovascular bundles
- Functions: thermal insulation, energy storage, cushioning, tethering skin to underlying fascia/muscle
- Blood vessels in the dermis and hypodermis form plexuses between each layer, all originating from source vessels via fine perforating vessels - Bailey and Love's, p. 1087 (plastic surgery section)
Skin Appendages (Epidermal Derivatives)
All derived from epidermis (ectoderm), but sit within the dermis:
Sebaceous Glands
- Holocrine glands (entire cell disintegrates to release secretion = sebum)
- Almost always associated with hair follicles - their duct opens into the upper portion of the hair follicle (pilosebaceous unit)
- Absent from palms and soles
- Sebum lubricates hair and skin, has mild antimicrobial properties
- Most numerous on face and scalp
Eccrine Sweat Glands
- Simple coiled tubular glands opening directly on skin surface
- Distributed almost everywhere; most numerous on palms and soles
- Produce watery sweat for thermoregulation
Apocrine Sweat Glands
- Open into hair follicles (not directly to skin surface)
- Located in axillae, groin, areola, perianal region
- Produce viscous secretion; odorless until acted upon by bacteria
Hair Follicles
- Invaginations of epidermis into the dermis
- Produce hair via a matrix of actively dividing cells
- Have a bulge region (lower permanent portion) containing stem cells
- Attached to arrector pili (smooth muscle) - contraction causes "goosebumps" (cutis anserina)
Nails
- Modified stratum corneum, produced by the nail matrix
II. SEBACEOUS CYST (Epidermoid Cyst)
Terminology
The term "sebaceous cyst" is a misnomer - these lesions are correctly called epidermoid cysts (or epidermal inclusion cysts). True sebaceous cysts (arising from sebaceous glands) are rare; the common clinical "sebaceous cyst" is an epidermoid cyst arising from follicular infundibulum, not the sebaceous gland itself. - Fischer's Mastery of Surgery, 8th Ed., p. 6205
Definition and Pathogenesis
Epidermoid cysts are the most common cutaneous cysts. They are:
- Benign subepidermal nodules filled with keratin (not sebum)
- Formed by plugging of the follicular orifice (infundibulum) → the follicular epithelium invaginates and proliferates, forming a cyst lined by stratified squamous epithelium
- The cyst wall is the keratinizing epithelium itself - this is the "capsule"
- Contents: white, cheese-like, foul-smelling keratin material (often called "sebaceous material" colloquially)
Location in the Skin
The cyst sits in the dermis / subepidermal plane, with:
- Its wall made of stratified squamous epithelium (continuous with the epidermis at the punctum)
- Contents occupying the space within the dermis
- A punctum (central pore) = the blocked follicular opening, visible as a small black dot on the surface
Clinical Features
| Feature | Description |
|---|---|
| Common locations | Face, scalp, neck, trunk, back, scrotum (can occur anywhere) |
| Size | 0.5 - 2 cm typically; can grow larger |
| Consistency | Smooth, round, mobile, rubbery nodule |
| Punctum | Central dark spot (pathognomonic) - blocked follicular orifice |
| Symptoms | Usually asymptomatic; may become infected |
| Contents | Cheesy, foul-smelling keratin expressed on rupture |
| Capsule | Pearly white; must be completely excised to prevent recurrence |
| Diagnosis | Clinical - history and examination; biopsy rarely needed |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 887
- Fischer's Mastery of Surgery, p. 6205
Complications
- Infection - increasingly caused by MRSA; cyst presents as tender, fluctuant, erythematous mass
- Rupture - releases keratin into dermis → intense foreign body inflammatory reaction ("rupture abscess")
- Recurrence - if capsule not fully removed
- Rare: malignant transformation to squamous cell carcinoma (extremely rare)
Treatment
Uninfected cyst:
- Complete surgical excision (elliptical incision centered on the punctum, dissecting out the entire capsule intact)
- An elliptical incision is made centered on the punctum, approximately a third of the cyst diameter in width
- The line of cleavage is sought and the cyst shelled out intact
- If rupture occurs during dissection, all fragments of epithelium must be removed or recurrence is certain
- Dead space closed with absorbable sutures, skin closed - Pye's Surgical Handicraft, 22nd Ed.
Infected / acutely inflamed cyst:
- Step 1: Incision and drainage (I&D) - express the thick sebaceous material manually (too thick to drain spontaneously)
- Step 2 (delayed): Excision of the pearly white capsule after inflammation has settled, to prevent recurrence
- Alternatively: primary excision at the initial sitting (evidence shows faster healing, fewer days of pain, less scarring - Kitamura et al. RCT, n=71) - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Key surgical principle: Loop drainage is not applicable to sebaceous cysts because the capsule must be removed - this distinguishes it from a simple abscess.
Summary: Sebaceous Cyst vs. Dermoid Cyst
| Epidermoid (Sebaceous) Cyst | Implantation Dermoid | |
|---|---|---|
| Origin | Follicular infundibulum (plugging) | Traumatic implantation of epidermis under skin |
| Location | Anywhere; face/scalp/trunk common | Hands and feet (digits) |
| Contents | Keratin | Keratin |
| Wall | Stratified squamous epithelium | Stratified squamous epithelium |
| Treatment | Excision | Excision |
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Eroschenko) | Bailey and Love's Short Practice of Surgery 28th Ed. | Fischer's Mastery of Surgery 8th Ed. | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Pye's Surgical Handicraft 22nd Ed. | Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.