Thromboangiitis obliterans in surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
thromboangiitis obliterans Buerger disease
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
thromboangiitis obliterans Buerger disease angiogram corkscrew collaterals
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough answer.
Thromboangiitis Obliterans (Buerger's Disease) — Surgical Perspective
Definition & Epidemiology
Thromboangiitis obliterans (TAO) is a progressive, nonatherosclerotic, segmental inflammatory disorder affecting small- and medium-sized arteries, veins, and nerves of the distal upper and lower extremities. First described by Leo Buerger in 1908 from 11 amputated limbs, it differs from atherosclerotic peripheral arterial disease in almost every dimension.
| Feature | Detail |
|---|---|
| Age of onset | 20–50 years (typically before age 40) |
| Sex | Predominantly male |
| Essential association | Tobacco use (cigarettes, chew, cannabis) |
| Geography | Higher prevalence in Asia, Eastern Europe, Middle East, India |
| Incidence in limb ischemia | <1% of severe limb ischemia in North America; 24% of lower limb ischemia in young adults (Mayo Clinic data) |
— Schwartz's Principles of Surgery, 11th Ed., p. 1002
Pathogenesis
The cause is unknown, but tobacco use is essential to both diagnosis and progression. Proposed mechanisms include:
- Direct endothelial cytotoxicity from tobacco components
- Immune-mediated injury — tobacco modifying vascular wall proteins → autoimmune response
- Most patients demonstrate hypersensitivity to intradermally injected tobacco extracts
- Impaired endothelium-dependent vasodilation (acetylcholine challenge)
- Association with specific MHC/HLA haplotypes suggests genetic susceptibility
— Robbins & Kumar Basic Pathology, p. 334; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 483
Pathology / Morphology
The hallmark is segmental, thrombosing, acute and chronic vasculitis affecting medium- and small-sized vessels — especially the tibial and radial arteries.
Histological Stages
| Stage | Findings |
|---|---|
| Acute | Dense PMN infiltration of vessel wall; cellular inflammatory thrombus in lumen; sterile microabscesses within the thrombus surrounded by granulomatous inflammation |
| Subacute/Chronic | Mononuclear cells, fibroblasts, giant cells replace neutrophils; thrombus organization and recanalization begins |
| End-stage | Perivascular fibrosis, organized thrombus; artery, adjacent vein and nerve encased in fibrous tissue |
Pathological distinction: TAO is one of the very few vasculitides where inflammation extends into contiguous veins and peripheral nerves. The internal elastic lamina is preserved (unlike PAN). The inflammatory thrombus is highly cellular, unlike bland atherosclerotic thrombus.
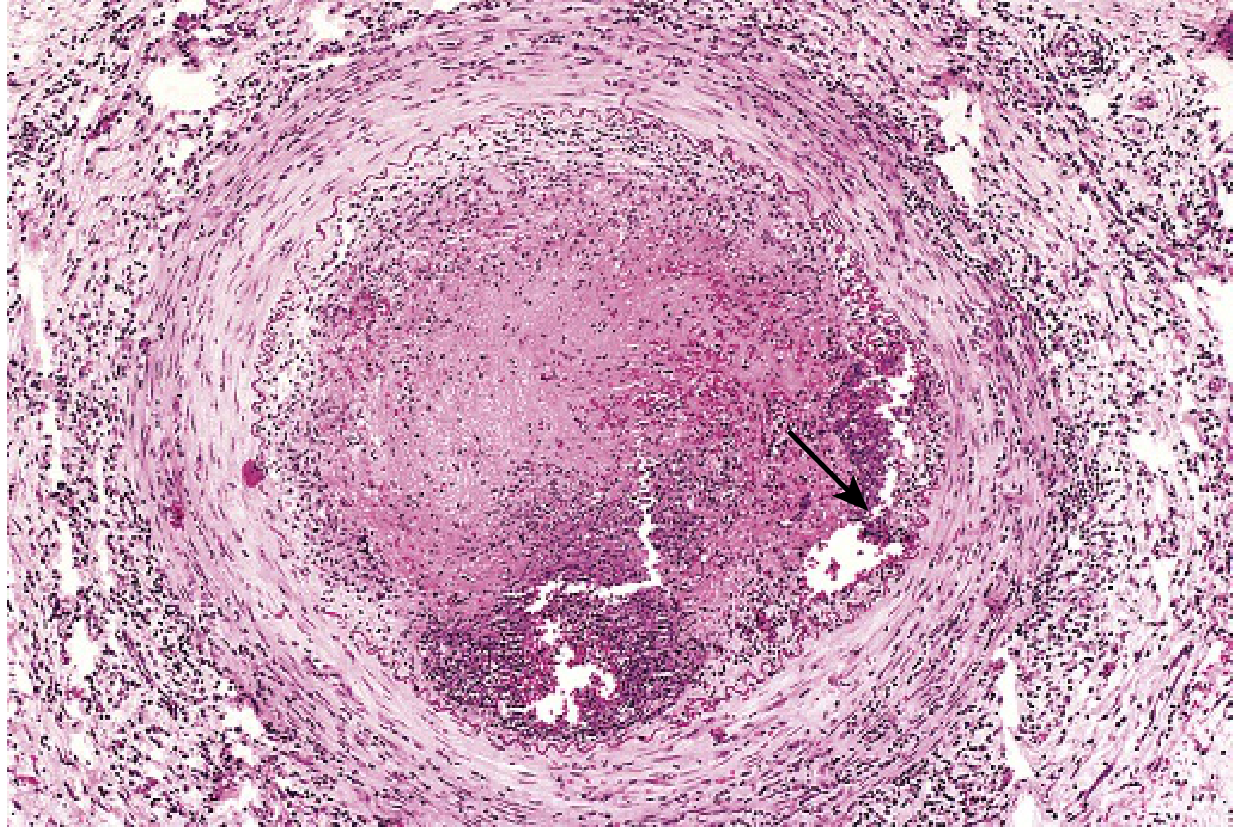
Buerger disease: lumen occluded by thrombus containing a sterile microabscess (arrow), vessel wall infiltrated with leukocytes. — Robbins & Kumar Basic Pathology, Fig. 8.25
Clinical Features
The classic triad is:
- Claudication of the affected extremity (instep/foot, forearm, hand — not calf, due to distal vessel predilection)
- Raynaud phenomenon (>40% of patients; often cold-induced)
- Migratory superficial thrombophlebitis (in up to 16% — indicates systemic inflammatory activity)
Progression
- Early: Foot arch pain on exercise (instep claudication), Raynaud phenomenon, superficial nodular phlebitis
- Late: Ischemic rest pain (severe — due to neural involvement), trophic nail changes, digital ulceration at fingertips/toes, gangrene
Physical Examination
- Normal brachial and popliteal pulses
- Reduced or absent radial, ulnar, and/or tibial pulses
- Abnormal Allen test (failure of one major hand artery to fill when other is compressed)
- Abnormal ankle-brachial index (ABI) with essentially normal proximal plethysmography
— Harrison's Principles of Internal Medicine, 22E, p. 2218; Goldman-Cecil Medicine
Diagnosis
Diagnostic Criteria
- Young smoker (<40–50 years) with distal extremity ischemia
- No diabetes, hyperlipidemia, or proximal source of emboli
- No serologic evidence of inflammatory vasculitis (ANA, ANCA, RF negative)
- Involvement of multiple limbs — angiography of all four limbs recommended
Imaging
Angiography (conventional, CTA, or MRA) is central. Characteristic findings:
- Disease confined to distal circulation (infrapopliteal; distal to brachial artery)
- Segmental occlusions with "skip" lesions
- "Corkscrew" collaterals — tortuous collateral vessels at sites of occlusion (hallmark sign, though not pathognomonic)
- Absence of proximal atherosclerosis
Angiogram showing corkscrew collaterals:
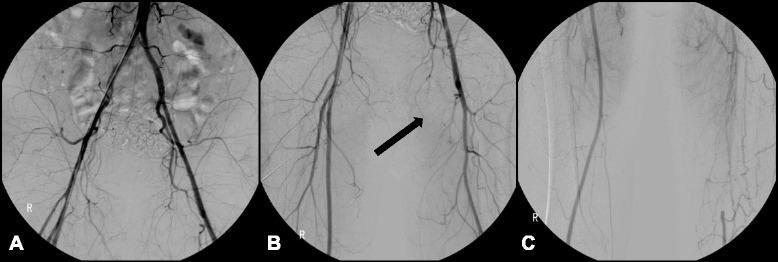
Lower extremity catheter angiogram: complete occlusion of left SFA with distal reconstitution via characteristic tortuous corkscrew collaterals from the deep femoral artery.
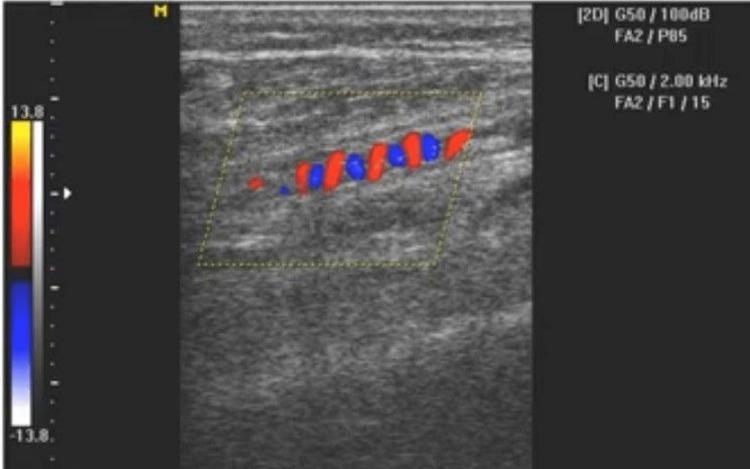
Doppler ultrasound showing corkscrew collaterals:
Definitive diagnosis: Excisional biopsy + histopathologic examination of an involved vessel.
Clinical Photographs

Ischemic digit in Buerger disease — note discoloration and darkened nail (Goldman-Cecil Medicine, Fig. 66-3)
Treatment
1. Smoking / Tobacco Cessation — THE Cornerstone
Complete abstinence from tobacco (and cannabis) is mandatory and the only proven disease-modifying intervention. Confirm with urinary cotinine testing.
- Patients who cease: disease remission; no progression with tissue loss (Oregon Health Sciences Center experience)
- Patients who continue: unrelenting pain, recurrent tissue necrosis, progressive amputation
- Amputation rate: 67% in smokers vs. 35% in those who quit
2. Medical Therapies
| Drug | Role |
|---|---|
| Antiplatelet (aspirin 81–325 mg/day) | Commonly prescribed; modest benefit only |
| Iloprost (prostacyclin analogue) | 1 ng/kg/min IV for 6 h/day × 28 days (off-label); superior to aspirin or lumbar sympathectomy for pain relief and wound healing |
| Calcium channel blockers, α-blockers, sildenafil | No proven benefit |
| Anticoagulants / glucocorticoids | Not helpful |
| Antibiotics | May be useful for infected ulcers |
| Bosentan | Tried with variable success |
| Spinal cord stimulators | Variable success |
| Intermittent pneumatic compression | Variable success |
3. Surgical Interventions
The role of surgical intervention is minimal in Buerger's disease due to:
- No acceptable target vessel for bypass (disease involves distal circulation)
- Limited autogenous vein conduit due to coexisting migratory thrombophlebitis
| Procedure | Indication / Notes |
|---|---|
| Arterial bypass | Only in selected cases with larger, more proximal vessel involvement |
| Angioplasty | May be effective in preserving the limb and preventing amputation; preferred over stenting in most cases |
| Stenting | Reserved for bail-out or more proximal disease |
| Lumbar/digital sympathectomy | Tried; variable results |
| Local debridement | For non-healing ulcers |
| Amputation | When all other measures fail; 31% limb loss over 15 years reported (Mills et al.) |
— Schwartz's Principles of Surgery, 11th Ed., p. 1002; Harrison's Principles, 22E; Goldman-Cecil Medicine
Prognosis
- Smoking cessation is the single most important prognostic factor
- Mills et al. (26 patients, 15 years): 31% limb loss
- Continued smokers: ~67% amputation; ex-smokers: ~35% amputation
- Once advanced vascular lesions are established, smoking cessation does not reverse them but prevents progression
- Visceral, cerebral, and coronary involvement occurs rarely but carries poor prognosis
Key Differentiators from Atherosclerotic PAD
| Feature | TAO | Atherosclerotic PAD |
|---|---|---|
| Age | <40–50 years | >50 years |
| Risk factors | Tobacco (essential) | HTN, DM, dyslipidemia |
| Vessels affected | Distal (tibial, radial, digital) | Proximal (aortoiliac, femoral) |
| Veins involved | Yes (migratory phlebitis) | No |
| Nerves involved | Yes | No |
| Angiogram | Corkscrew collaterals, skip lesions | Diffuse calcified plaque |
| Bypassability | Poor (no target) | Good |
Recent Evidence (2023–2026)
- A 2025 review (Front Immunol, PMID 40936931) highlights endothelial activation as a key mechanism, with emerging therapeutic targets.
- A 2025 review (J Clin Med, PMID 40725544) addresses challenges in angiography pattern interpretation and recommends standardized diagnostic criteria.
Sources: Schwartz's Principles of Surgery 11th Ed.; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.