My uncle who was who had an RTA was partly in the ICU for 15 days and today he has been shifted to the HDU. The edema has also started decreasing and is on the last phase of edema. It will be minimum in a few more days, said the neurologist. And now he is saying that earlier, uh, earlier he had EDH, HDH and contusion. And now he is saying that there is some kind of water like fluid. And the water like fluid subsides in 95% of the patients and in 5% of the patient, a hole has to be made in the skull to drain the fluid. So, what is that fluid and what is the effect of that fluid? Explain.
subdural hygroma after traumatic brain injury treatment burr hole drainage
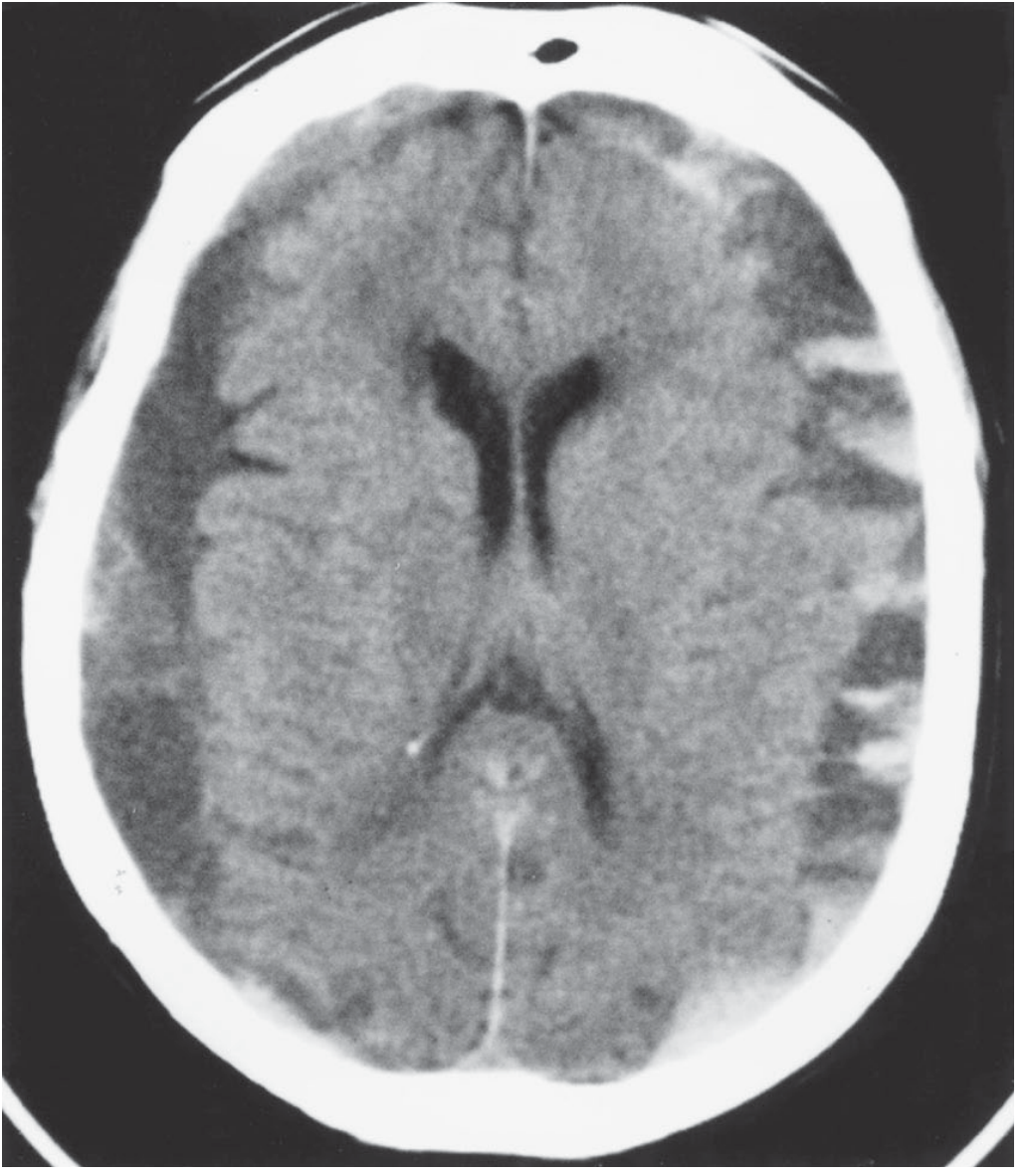
The "Water-Like Fluid" - Subdural Hygroma
What Happened to Your Uncle - Quick Recap
- EDH (Epidural Hematoma) - blood collected between the skull and the outer brain covering (dura)
- SDH (Subdural Hematoma) - blood collected between brain coverings (likely what "HDH" refers to)
- Contusion - bruising of the brain tissue itself
- Cerebral edema - swelling of the brain, now resolving
What Is a Subdural Hygroma?
Why Does It Develop at THIS Stage (After 15 Days)?
What Effects Can It Cause?
| Effect | Explanation |
|---|---|
| Brain compression | If the fluid collection grows large, it can press on the brain tissue, similar to how the original hematoma did |
| Headache | Increased pressure inside the skull |
| Drowsiness or confusion | If the fluid compresses brain areas controlling alertness |
| Weakness on one side | If it presses on motor areas |
| Speech difficulties | If it presses on language areas |
| Rarely, seizures | Though the association is not always direct |
When Is the "Hole in the Skull" (Burr Hole) Needed?
- The hygroma keeps growing instead of shrinking
- It causes significant brain compression (seen on CT as midline shift)
- The patient develops new neurological symptoms - worsening consciousness, limb weakness, severe headache
- It converts into a chronic subdural hematoma (the hygroma can sometimes trigger small bleeds from new fragile blood vessels that form around it, turning the clear fluid into blood-tinged fluid) - DiMaio's Forensic Pathology, 3rd Edition
The Key Point About Your Uncle's Case
- He survived a severe RTA with EDH + SDH + contusion
- Spent 15 days in ICU and is now in HDU (High Dependency Unit - a step down from ICU)
- His brain edema is already resolving
- He is stable enough for the neurologist to simply monitor the hygroma
Right now, my uncle has been speaking unconsciously, telling that to take him home and then he does not like him here. He wants to have tea and biscuits and I don't know whether he is speaking unconsciously or consciously, but he is speaking like that agitated way and he is asking all the family members to take him home, but he does recognize the family members. And earlier, his personality was not like this, but right now, it is like this. So, will his personality be like this only or will he change and how long will it take for him to change? Can you just suggest me and then his hands and feet are tied in the hospital so that he is not agitated and he does not move out.
post traumatic agitation after brain injury ICU confused agitated wants to go home personality change recovery
https://www.flintrehab.com/agitation-after-traumatic-brain-i…
What Is Happening to Your Uncle Right Now
The Medical Name: Post-Traumatic Agitation / Post-Traumatic Amnesia (PTA)
- Does not know where they are (hospital feels strange and frightening to them)
- Does not know what day/time it is or how long they have been there
- Cannot form new memories - they may ask the same question repeatedly because they forget the answer immediately
- Feels confused, disoriented, and scared - which comes out as agitation
- Recognizes familiar faces (family) but cannot make sense of the unfamiliar environment (hospital)
- Says things that seem random or confused - this is not "unconscious talking," their brain is active but not fully processing reality correctly - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Is the Agitation a Good Sign or Bad Sign?
- Agitated patients had better discharge Glasgow Coma Scores (a measure of consciousness)
- They were more frequently discharged home or to rehabilitation
- Agitation was temporally linked with the recovery of consciousness - meaning the brain "waking up" often looks like agitation first
Why Are His Hands and Feet Tied?
- Try to pull out IV lines, feeding tubes, oxygen tubes, drain tubes - which can be life-threatening
- Try to get out of bed and fall, risking serious injury
- Harm themselves without meaning to
Will His Personality Return to Normal?
Most Likely Scenario (PTA - Temporary Phase):
Timeline:
- PTA typically lasts days to a few weeks in moderate-to-severe TBI
- Since your uncle is already in HDU, already recognizing family, and already speaking - these are all signs of active brain recovery
- Most families see clear improvement in orientation and calmness within 1-3 weeks of this phase beginning
- Full personality recovery and settling can take 3-6 months, with continued slow improvement up to 1-2 years
If There Is Frontal Lobe Involvement:
- Increased irritability or short temper
- Slightly reduced patience
- Occasional impulsive behavior
What You and the Family Can Do Right Now
| What to Do | Why It Helps |
|---|---|
| Speak in a calm, soft, slow voice | The brain is overwhelmed - loud voices increase agitation |
| Keep visits short but frequent | Too much stimulation at once worsens confusion |
| Reorient him gently and repeatedly | "Uncle, you are in the hospital. You had an accident. You are safe. We are all here." Say this every visit even if he forgets |
| Bring familiar items - a photo, a familiar smell, his prayer beads, a piece of cloth from home | Familiar sensory inputs help the brain orient |
| Do not argue with anything he says - don't say "no you can't go home" - instead redirect: "You will go home soon. The doctors are helping you get better so you can have tea at home." | Arguing with confused patients escalates agitation |
| Consistent visitors - same faces each time | Familiarity is calming |
| Keep the room quiet - reduce TV noise, phone noise, multiple people talking at once | Sensory overload worsens PTA agitation |