elaborate spastic diplegia
spastic diplegia cerebral palsy
Spastic Diplegia
Definition and Eponym
Epidemiology
-
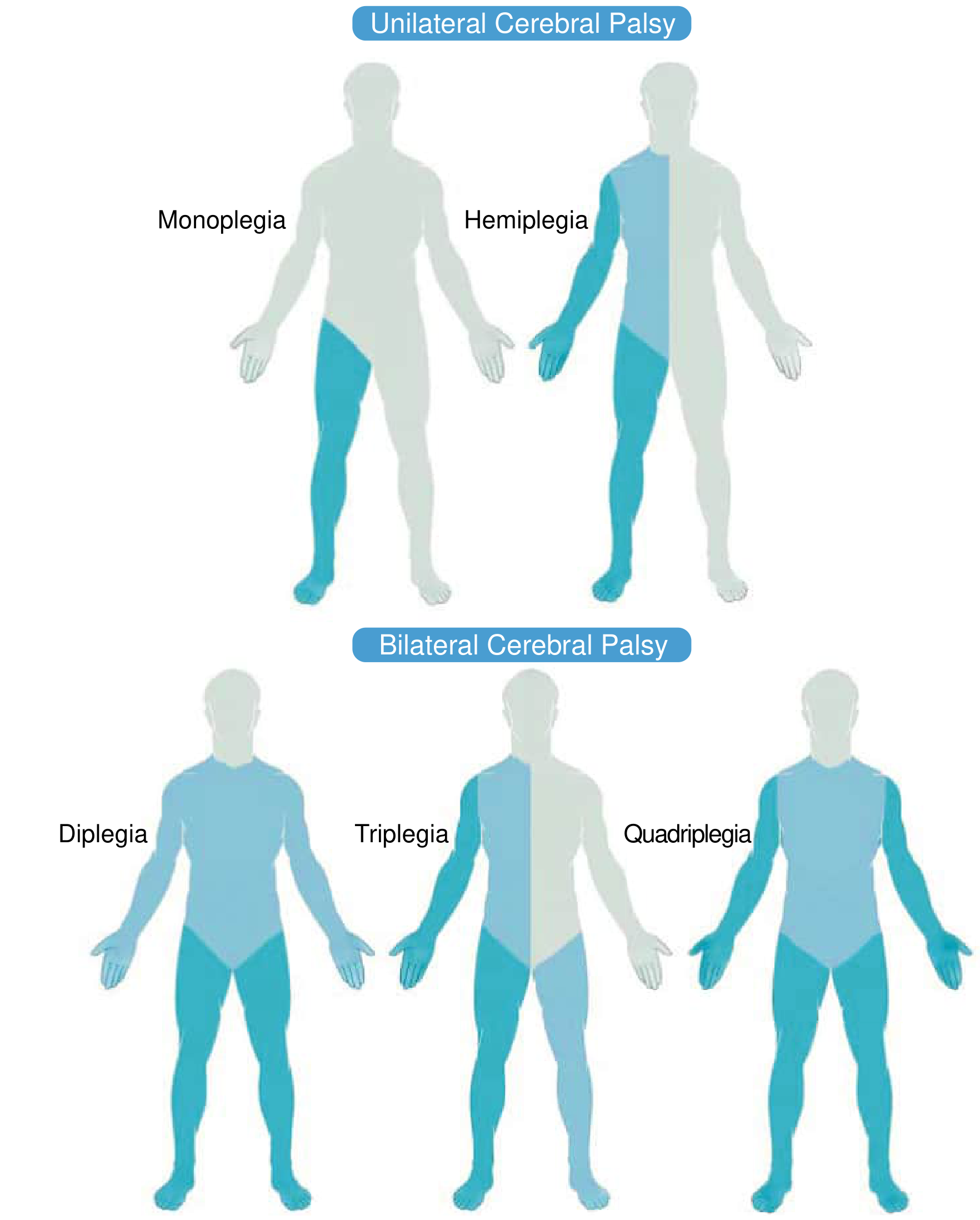
Spastic diplegia: legs > arms
-
Spastic hemiplegia: one side, usually arm > leg
-
Spastic quadriplegia: all four limbs + trunk + face
-
Bradley and Daroff's Neurology in Clinical Practice
Pathology and Etiology
Primary Underlying Lesion: Periventricular Leukomalacia (PVL)
- Hypoxia-ischemia is the primary mechanism, causing free radical exposure, cytokine toxicity, and glutamate excitotoxicity
- Immature oligodendrocytes (premyelinating) are particularly vulnerable
- Loss of oligodendrocytes leads to white matter volume loss and ventriculomegaly
- Preterm brains have a "pressure-passive" circulation - systemic BP drops directly reduce cerebral perfusion
- At early gestations (24-28 weeks), there are few anastomoses between long and short penetrating arteries, making border zones more susceptible
Major Etiological Categories
- Matrix hemorrhage (periventricular/intraventricular hemorrhage)
- Periventricular leukomalacia (most direct cause)
- Hypoxic-ischemic encephalopathy
- Kernicterus (hyperbilirubinemia)
Risk Factors
| Risk Factor | Details |
|---|---|
| Prematurity | Incidence of CP in very preterm (<32 weeks) = 8.7%; late preterm (34-37 weeks) = 0.6% |
| Very low birth weight | <1500 g is a strong predictor |
| Multiple gestation | Risk largely mediated by prematurity |
| PV/IVH | Especially severe grades |
| Maternal infection | Chorioamnionitis |
| Perinatal asphyxia | Though often insufficient alone to cause CP |
- Bradley and Daroff's Neurology in Clinical Practice
Clinical Features
Neonatal Presentation
- Hypotonia with retained tendon reflexes (not spasticity) in the first months
- Extensor plantar reflexes (Babinski sign) - pathologic at any age after infancy
- Stiff, awkward movements of the legs when lifted by the axillae
- Adduction posture of lower limbs
Later Childhood: Gait Pattern
- Scissors gait: adduction of the thighs so strong that the legs may cross during walking
- Toe walking: feet are plantar-flexed with heels not touching the floor
- Crouch gait: hamstring contractures cause excessive hip and knee flexion
- Stiff-knee gait: rectus femoris fires out of phase, limiting knee flexion during swing phase
- Short steps, each leg describing an arc of a circle
- Legs are maintained in a slightly flexed, adducted posture
Upper Limb Findings
- Awkwardness and stiffness of fingers
- Overpronation when reaching for an object
- Difficulty releasing a grasp
- In pronounced cases, weakness and spasticity of the hands
Other Features
-
Speech may be well articulated or noticeably slurred
-
In some cases, spastic facies
-
Legs tend to be short and small in adolescence/adulthood (but not markedly atrophic as in spinal muscular atrophy)
-
Passive manipulation reveals spasticity in extensors and adductors, with shortened calf muscles
-
Intelligence: often preserved or only mildly affected (in contrast to spastic quadriplegia)
-
Adams and Victor's Principles of Neurology, 12th Ed.
Classification by Functional Level: GMFCS
- Level I: walks without limitations
- Level II: walks with limitations
- Level III: walks using hand-held mobility device
- Level IV: self-mobility with limitations; may use powered mobility
- Level V: transported in manual wheelchair
Neuroimaging
- Periventricular leukomalacia is the most common finding (present in ~42% of all CP cases)
- Signal changes in periventricular white matter, often with ventriculomegaly
- Basal ganglionic damage seen in ~13%
- Cortical-subcortical lesions, malformations, or focal infarcts may also be found
- MRI can be normal in a subset of cases
- Bradley and Daroff's Neurology in Clinical Practice
Orthopaedic Management
Assessment
- Based on physical exam, birth history, developmental history
- Primitive reflex persistence informs prognosis for ambulation
- Gait analysis (including EMG) guides surgical planning
- A locomotor profile based on two or more persistent primitive reflexes predicts non-ambulation
Spasticity Management
- Mechanism: presynaptic blockade of cholinergic receptors at the neuromuscular junction
- Effect duration: 3-6 months (not a permanent solution)
- Used to maintain joint range of motion during rapid growth phases when the child is too young for surgery
- Miller's Review of Orthopaedics, 9th Ed.
- Neurosurgical procedure to decrease lower extremity spasticity
- Involves resection of dorsal rootlets that lack a normal myographic/clinical response to stimulation
- Primary indication: ambulatory patients aged 4-8 years with spastic diplegia
- Requires multilevel laminoplasty (risk of late spinal instability/deformity)
- Contraindicated in: athetoid disease; non-ambulatory patients with spastic quadriplegia
- Oral baclofen: adjunct to control overall tone; inhibits signals via the GABA pathway; decreases tone in all extremities
- Intrathecal baclofen (ITB) pump: higher-dose baclofen delivered intrathecally; negative effects include respiratory depression and drug dependency if stopped abruptly
| Gait Problem | Finding | Surgical Option |
|---|---|---|
| Hip flexion | Positive Thomas test | Psoas tenotomy/recession |
| Spastic hip | Decreased abduction, uncovered femoral head | Adductor release, later osteotomy |
| Hip adduction / scissors gait | Scissoring | Adductor release |
| Femoral anteversion | Increased prone internal rotation | Varus derotation osteotomy, hamstring lengthening |
| Knee flexion / crouch gait | Increased popliteal angle | Hamstring lengthening |
| Stiff-knee gait | Out-of-phase rectus femoris on EMG | Distal rectus transfer to hamstrings |
| Talipes equinus / toe walking | Toe walking | Achilles tendon lengthening |
| Talipes equinovalgus | Most common in spastic diplegia | Peroneus brevis lengthening; calcaneal osteotomy |
| Talipes varus | Appearance in standing | Split anterior/posterior tibialis transfer |
| Hallux valgus | Exam and X-ray | Osteotomy or MTP fusion |
- Miller's Review of Orthopaedics, 9th Ed.
Foot and Ankle in Spastic Diplegia
- Spastic peroneal muscles
- Contracted heel cords
- Ligamentous laxity
Hip Complications
- Hip subluxation: adductor tenotomy when abduction <20°, sometimes with psoas release
- Femoral coxa valga + acetabular dysplasia: femoral or pelvic osteotomy
- Spastic dislocation: open reduction, femoral shortening, varus derotation osteotomy (VDO), Dega osteotomy, or Chiari osteotomy
- Windswept hips: abduction of one hip and adduction of the other; bilateral femoral osteotomies to achieve varus correction
Associated Conditions
- Seizures (~30% of cases)
- Cognitive impairment: less common in diplegia than quadriplegia; intelligence often preserved
- Visual impairment (particularly strabismus)
- Speech and language difficulties
- Bladder dysfunction
- Scoliosis: significant risk in severe/total body involvement; surgical intervention for curves >45-50 degrees with progressive pelvic obliquity
Prognosis
- Adams and Victor's Principles of Neurology, 12th Edition
- Bradley and Daroff's Neurology in Clinical Practice
- Miller's Review of Orthopaedics, 9th Edition
- Creasy & Resnik's Maternal-Fetal Medicine
Can Phakka Vyadhi be corelated with any modern allopathy disorder
Phakka Vyadhi Ayurveda modern correlation allopathy disorder
Phakka Vyadhi Ayurveda rickets
https://jaims.in/index.php/jaims/article/download/4690/8079?…
Phakka Vyadhi types Kshiraja Garbhaja Vyadhija symptoms classical description Kashyapa Samhita
Phakka Vyadhi - Correlation with Modern Allopathic Disorders
What is Phakka Vyadhi?
Ayurvedic Pathophysiology (Samprapti)
Hetusevan (causative factors) → Kapha Dushtha Stanya (vitiated breast milk) or reduced nutrition → Strotodushti + Dhatwagnimandya (impaired channel function and tissue metabolism) → Rasadi Dhatu Dushti + Alpopachaya (poor nourishment of tissues especially Rasa and Asthi Dhatu) → Vataprakopa + Grahani Dushti + Agnimandya → Dhatu Kshaya (tissue wasting) → Phakka Vyadhi
Three Types of Phakka Vyadhi
| Type | Ayurvedic Cause | Modern Correlation |
|---|---|---|
| Kshiraja Phakka | Stanya (breast milk) vitiated with Kapha Dosha (called "Phakka-Dugdha") → causes obstruction in Rasavaha Srotasa → nutritional deficiency in infant | Acute malnutrition due to poor breast milk quality; analogous to early-stage Protein Energy Malnutrition (PEM) or failure to thrive from breastfeeding inadequacy |
| Garbhaja Phakka | Lactating mother becomes pregnant too soon → milk quantity/quality decreases → child becomes emaciated, may die | Advanced PEM; closely resembles Kwashiorkor (protein-deficiency malnutrition when child is displaced from breast by new pregnancy) |
| Vyadhija Phakka | Child suffers from repeated Nija (endogenous) or Agantuja (exogenous/environmental) diseases → progressive wasting of Mamsa, Rakta, Asthi Dhatu | Chronic malnutrition with generalized motor disability; correlates with Marasmus, chronic infections (TB), malabsorption states |
Modern Allopathic Correlations
1. Rickets (PRIMARY and most widely accepted correlation)
| Phakka Vyadhi Feature | Rickets Feature |
|---|---|
| Inability to stand or walk (Padabhyam na Gacchati) | Delay in walking, inability to weight-bear |
| Asthi Dhatu Dushti (bone tissue pathology) | Softening and weakening of growing bones |
| Asthivaha Srotasa Dushti | Impaired bone mineralization |
| Bony deformities of limbs | Bow legs (genu varum), knock-knees (genu valgum) |
| Weak, soft bones prone to injury | Pathological (greenstick) fractures of long bones |
| Cranial softness (Mridu Murdha) | Craniotabes, frontal bossing, delayed fontanelle closure |
| Chest deformity | Rachitic rosary (costochondral junction widening), pigeon chest, pectus excavatum |
| Short stature | Growth retardation, short stature |
| Widening of wrists and ankles | Widened epiphyses and metaphyses |
| Spinal deformity (Kyphosis) | Kyphosis/scoliosis from ligamentous laxity |
| Pot belly (abdominal protuberance) | Pot-belly from abdominal hypotonia and visceroptosis |
| Hyper-extensible joints | Ligamentous laxity in rickets |
| Nutritional deficiency as root cause | Vitamin D/calcium/phosphate deficiency |
2. Protein-Energy Malnutrition (PEM) - Marasmus and Kwashiorkor
- Kshiraja and Garbhaja Phakka = acute malnutrition, correlating with Marasmus (caloric and protein deficiency, severe muscle wasting, loss of subcutaneous fat from gluteal, chest, and extremities, protuberant abdomen, dominant head and face)
- Garbhaja Phakka especially resembles Kwashiorkor (child displaced from breast when mother becomes pregnant again, develops protein deficiency with edema, irritability, skin changes)
- Vyadhija Phakka = chronic malnutrition with motor disability, resembling chronic PEM with failure to thrive
3. Cerebral Palsy (Spastic Diplegia)
4. Muscular Dystrophies
5. Chronic Malabsorption Syndromes
- Celiac disease (gluten-sensitive enteropathy)
- Tropical sprue
- Inflammatory bowel disease in children
- Other chronic malabsorption states leading to secondary nutritional deficiencies and bone disease
6. Tuberculosis and Chronic Infections
7. Endocrine and Metabolic Errors
- Hypothyroidism (cretinism) - causes motor delay, bone maturation delay
- Inborn errors of metabolism (e.g., Glycogen storage diseases, mucopolysaccharidoses)
- Hypophosphatemic (Vitamin D-resistant) rickets - X-linked genetic defect in phosphate-regulating enzyme, causing severe rickets unresponsive to standard Vitamin D treatment - Miller's Review of Orthopaedics, 9th Ed.
Summary Table
| Phakka Type | Best Modern Correlate | Secondary Correlates |
|---|---|---|
| Kshiraja Phakka | Rickets (nutritional), early PEM | Failure to thrive, breastfeeding-associated malnutrition |
| Garbhaja Phakka | Kwashiorkor, Marasmus | PEM-associated rickets |
| Vyadhija Phakka | Marasmus, chronic PEM | Cerebral palsy, Muscular dystrophies, TB, Celiac disease, Metabolic bone disease, Endocrine disorders |
Consensus View in Modern Ayurvedic Scholarship
"The clinical presentation of Phakka contributes nutritional and metabolic disorders like malnutrition, malabsorption disorders, and different inborn and acquired errors of the metabolism and conditions like Cerebral Palsy, protein energy malnutrition, skeletal deformities, rickets, tuberculosis-like infectious disorders, muscular dystrophies, endocrinal metabolic errors, all ending up as a condition of Phakka causing failure to thrive."
How can be phakka corelated with periventricular lucomalacia
Phakka Vyadhi periventricular leukomalacia correlation Ayurveda cerebral palsy spastic diplegia
Garbhaja Phakka prematurity periventricular leukomalacia Ayurveda Vata Dhatu kshaya preterm infant
https://ijrap.net/admin/php/uploads/3426_pdf.pdf
Phakka Vyadhi and Periventricular Leukomalacia (PVL) - A Cross-System Correlation
Framing the Question
- Clinical phenotype - both conditions produce the same end presentation in a child
- Etiological overlap - the root causes described in each system parallel each other
- Pathophysiological analogues - the Ayurvedic Dhatu/Dosha mechanism mirrors the modern cellular injury cascade
What Each System Describes
PVL (Modern Medicine)
- Focal periventricular necrosis - coagulative necrosis in border zones of long penetrating arteries at the level of the trigone of lateral ventricles and foramen of Monro, resulting in cyst formation or glial scars
- Diffuse white matter injury - targeting premyelinating oligodendrocytes, causing global oligodendrocyte loss, astrocytic gliosis, white matter volume loss, and ventriculomegaly
Phakka Vyadhi (Ayurveda)
- Garbhini/Dhatri-related causation (maternal/nutritional factors in the prenatal/perinatal period)
- Strotodushti (impaired channels) particularly of Rasavaha, Asthivaha, Majjavaha, and Mamsavaha Srotasas
- Dhatwagnimandya (impaired tissue-level metabolism)
- Dhatu Kshaya (wasting of Rasa, Mamsa, Meda, Asthi, and Majja Dhatus)
- Vataprakopa (aggravation of Vata) as the final common pathway producing motor dysfunction
Point-by-Point Correlation
1. Etiology
| Phakka Vyadhi (Ayurveda) | PVL (Modern Medicine) |
|---|---|
| Garbhaja Phakka - mother becomes pregnant while lactating; malnourishment leads to deficient fetal/infant nutrition; Ksheem Garbhini (depleted pregnant mother) | Prematurity - premature birth is the dominant risk factor; PVL is overwhelmingly a disease of the preterm infant (<32 weeks); nutritional compromise of the fetus matches the concept of Garbhaja Phakka |
| Kshiraja Phakka - Kapha-Dushtha Stanya (qualitatively impaired breast milk) → Rasavaha Srotasa obstruction | Perinatal hypoxia-ischemia, maternal infection, chorioamnionitis - cause poor nutritional/oxygen delivery to fetal brain |
| Vyadhija Phakka - repeated illness/fever → Dhatwagnimandya → Majja + Asthi Dhatu Kshaya | Post-infection PVL: maternal/fetal infection causes cytokine-mediated white matter injury even without frank ischemia |
| Agnimandya (impaired metabolic fire at tissue level) → failure to nourish Majja Dhatu | Oligodendrocyte immaturity - premyelinating oligodendrocytes fail to mature and myelinate → analogous to Majja Dhatwagnimandya (failure of nervous tissue formation) |
The concept of Garbhaja Phakka maps most precisely to PVL-associated spastic diplegia: both involve a nutritionally/physiologically compromised prenatal state (depleted mother / hypoxic-ischemic preterm environment) leading to a child who cannot walk.
2. Pathophysiology
| Ayurvedic Concept | PVL Equivalent |
|---|---|
| Majjavaha Srotasa Dushti - impaired channels nourishing Majja Dhatu (bone marrow / nerve tissue) | Ischemic destruction of periventricular white matter - the anatomical home of descending neural tracts |
| Majja Dhatu Kshaya - depletion of nervous tissue | Loss of oligodendrocytes → failed myelination → white matter volume loss |
| Asthivaha Srotasa Dushti - Asthi Dhatu (bone/structural tissue) malnourished | Periventricular cyst formation and gliosis replacing functional white matter |
| Vataprakopa - Vata Dosha governs all motor and sensory neural functions; when it is excessively aggravated through Dhatu Kshaya, movement disorders result | Destruction of corticospinal tract fibers passing through periventricular white matter → UMN spasticity and motor paralysis |
| Kaphavrita Vata (Vata obstructed/enveloped by Kapha) - causes muscle rigidity, spasticity, and resistance to movement | Spasticity in PVL/spastic diplegia - upper motor neuron lesion → loss of inhibition → hypertonicity and clasp-knife rigidity |
| Avarana Janya Vata Vyadhi (obstruction-induced Vata disorder) | Loss of descending inhibitory tracts from cortex → disinhibited spinal reflexes → spastic diplegia |
| Snayu (ligament/tendon/nerve) and Kandara (tendon) vitiation | Corticospinal tract and association fiber injury in white matter |
3. Clinical Features - Mirror Image
| Phakka Vyadhi Feature | PVL/Spastic Diplegia Feature |
|---|---|
| Inability to walk or stand after 1 year (Padabhyam na Gacchati) | Delayed walking; inability to weight-bear; scissors gait |
| Sluggish/creeping movement (literal meaning of "Phakka") | Characteristic stiff, slow gait with short steps; toe walking; crouch gait |
| Lower limb predominance | PVL preferentially damages corticospinal fibers to lower limbs (somatotopic: leg fibers are medial/periventricular, arm fibers are lateral and spared) |
| Weak, hypotonic lower limbs progressing to spasticity | Initial hypotonia in neonate → spasticity emerges over months as pyramidal tract maturation reveals the lesion |
| Psychomotor delay | Cognitive and motor developmental delay; persistence of primitive reflexes |
| Mridu Murdha (soft head/skull changes) | Ventriculomegaly; posterior horn enlargement ("colpocephaly") on MRI in PVL |
| Seizures in ~1/3 of cases | Seizures common in periventricular injury |
| Wasting of gluteal, thigh, and lower limb muscles | Disuse atrophy of lower limbs; short, small legs in older children |
| Upper limbs relatively spared or mildly affected | Arms largely spared in spastic diplegia (arm fibers in corona radiata are lateral to PVL zone) |
4. Srotasa-Organ Correlation
| Srotasa | Modern Equivalent | Role in PVL |
|---|---|---|
| Rasavaha (plasma/nutritive channels) | Cerebrovascular circulation | Ischemic shut-down of periventricular perfusion |
| Majjavaha (nervous tissue channels) | White matter tracts and myelinated nerve fibers | Directly destroyed in PVL |
| Mamsavaha (muscular channels) | Neuromuscular system | Secondary disuse atrophy of lower limbs |
| Asthivaha (bone tissue channels) | Bone growth/remodeling | Secondary skeletal deformity from spastic forces |
5. The Garbhaja-PVL Link in Detail
- The classical description says: "Garbhinim-atruka kshipra stanyasya vinivartanat" - when a nursing mother quickly becomes pregnant again, her milk diminishes in both quantity and quality. The infant, deprived of adequate nutrition from this depleted lactating-pregnant mother, becomes emaciated with weak limbs and may even die.
- This maps to the modern scenario of:
- A preterm infant born to a physiologically depleted/stressed mother
- Inadequate nutritional substrate reaching the fetus during the critical window of 24-32 weeks when periventricular white matter is most vulnerable
- Resulting in PVL with subsequent failure to walk by the expected milestone
6. Why PVL Is More Than "Just Rickets" in the Phakka Spectrum
| Feature | Rickets (Phakka) | PVL/Spastic Diplegia (Phakka) |
|---|---|---|
| Root cause | Nutritional deficiency (Vit D/Ca) | Perinatal ischemia + white matter injury |
| Bone pathology | Primary (soft bones) | Secondary (deformity from spasticity) |
| Tone | Hypotonia, lax joints | Spasticity (hypertonia) |
| Reflexes | Normal or reduced | Exaggerated (UMN pattern) |
| Walking inability | Due to bone weakness | Due to motor tract destruction |
| Ayurvedic Dhatu | Asthi + Meda Dhatu Kshaya | Majja + Mamsa Dhatu Kshaya + Vataprakopa |
| Srotasa | Asthivaha, Rasavaha | Majjavaha, Mamsavaha, Rasavaha |
| Phakka type | Kshiraja/Ksheeraja | Garbhaja / Vyadhija |
Summary
- Garbhaja Phakka - prenatal nutritional compromise of the child - mirrors the PVL scenario of a preterm infant suffering periventricular ischemia due to an immature, pressure-passive cerebrovascular system
- Majja Dhatu Kshaya + Vataprakopa - the Ayurvedic pathology of depleted nervous tissue with aggravated Vata - mirrors the destruction of oligodendrocytes and corticospinal tracts in PVL
- Kaphavrita Vata / Avarana Janya Vata - the mechanism producing spasticity - mirrors the UMN disinhibition seen in PVL-associated spastic diplegia
- The clinical endpoint - "Padabhyam na Gacchati" (cannot walk on feet) with predominantly lower limb involvement - is identical in both systems
- Modern Ayurvedic scholarship (Narayanan, IJRAP 2025) has begun treating this condition as exactly this correlation, using Panchakarma targeting Majja Dhatu Poshana (nourishing nervous tissue) via Basti, Shiropichu, and Shashtika Shali Pinda Sweda for the PVL child with spastic diplegia
Tell me inclusion criteria and exclusion criteria for spastic diplegia/ PVL for Phakka
inclusion exclusion criteria spastic diplegia PVL Phakka Ayurveda clinical study
Phakka Roga inclusion exclusion criteria Kaumarbhritya clinical trial research
https://ijrap.net/admin/php/uploads/2027_pdf.pdf
Inclusion and Exclusion Criteria
For Correlating Spastic Diplegia / PVL with Phakka Vyadhi
(As applicable to clinical studies, case selection, or Ayurvedic OPD practice)
DIAGNOSTIC CRITERIA (must be satisfied before applying inclusion/exclusion)
Modern Side
- History of prematurity (<37 weeks gestation, typically <32 weeks) OR documented perinatal hypoxic-ischemic event
- MRI brain showing periventricular white matter signal changes, cystic PVL, periventricular gliosis, posterior horn ventriculomegaly (colpocephaly) - consistent with PVL
- Clinical picture of spastic CP - non-progressive motor disorder with:
- Increased muscle tone (hypertonia) in lower limbs > upper limbs
- Exaggerated deep tendon reflexes (DTR) bilaterally in lower limbs
- Extensor plantar response (positive Babinski)
- Delayed motor milestones
- Topographic distribution - legs predominantly affected (diplegia), arms spared or mildly involved
Ayurvedic Side (Phakka Vyadhi - Garbhaja/Vyadhija type)
- Padabhyam na Gacchati - child unable to walk or stand on feet beyond expected age (>1 year)
- Presence of Vataprakopa Lakshanas - spasticity, stiffness, contractures (Sthamba), loss of voluntary movement
- Evidence of Majja + Mamsa Dhatu Kshaya - wasted lower limbs, poor muscle bulk
- Majjavaha + Mamsavaha Srotasa Dushti - impaired neural and muscular channels
- History suggesting Garbhaja Nidana - prematurity, complicated delivery, or Vyadhija Nidana - perinatal disease/injury
- Kaphavrita Vata / Avarana Janya Vata pattern - rigidity overlying loss of voluntary motor control
INCLUSION CRITERIA
A. Age Criteria
| Parameter | Criterion |
|---|---|
| Age range | 1 to 12 years (most studies use 3-8 years; AIIA protocol uses 1-10 years) |
| Minimum age | ≥1 year (below this, Phakka cannot be definitively diagnosed as per Kashyapa's definition) |
| Maximum age | ≤12 years (adolescent and adult cases are considered established/fixed; neuroplasticity window for Ayurvedic treatment is most favourable in early childhood) |
B. Clinical Features (Modern)
- Diagnosed case of spastic diplegia type cerebral palsy with MRI-confirmed PVL changes
- Lower limb predominant spasticity - bilateral increased tone, legs affected more than arms
- Exaggerated DTRs in lower extremities (knee jerk, ankle jerk hyperreflexia)
- Positive Babinski sign bilaterally
- Delayed motor milestones - failure to walk independently by expected age
- Scissor gait, toe walking, or crouch gait on assessment
- Modified Ashworth Scale (MAS) score of ≥1 in relevant muscle groups
- GMFCS (Gross Motor Function Classification System) levels I to IV (ambulatory or potentially ambulatory cases)
C. Etiological/Historical Criteria (Modern + Ayurvedic)
- Birth history of prematurity (<37 weeks), OR
- History of perinatal asphyxia / birth hypoxia, OR
- History of neonatal intensive care admission, mechanical ventilation, or NICU stay
- (Ayurvedic equivalent): Evidence of Garbhaja Nidana (complications during pregnancy - Garbhini Kshama, Garbhini suffering from illness or nutritional deficiency, or delivery complications)
D. Ayurvedic Phakka Criteria
- Presence of Phakka Lakshanas as per Kashyapa Samhita:
- Inability to walk / stand on feet despite crossing the walking milestone age
- Sluggish, creeping movement (literal Phakka = creeping/sloth)
- Weak, thin lower limbs with wasted gluteal, thigh muscles (Mamsa Kshaya)
- Asthivaha Srotodushti features - bony changes, deformities (valgus/varus feet, hip abnormalities)
- Psychomotor delay with poor developmental progress
- Case must fit Garbhaja Phakka or Vyadhija Phakka subtype (not Kshiraja, which is primarily a breast milk/nutritional disorder without neurological injury)
E. Consent
- Parents/guardians willing to give written informed consent for participation
- Parents able to comply with treatment schedule and follow-up
EXCLUSION CRITERIA
A. Diagnostic Exclusions (Modern)
| Category | Specific Conditions to Exclude |
|---|---|
| Progressive neurological disorders | Spinal muscular atrophy (SMA), Duchenne Muscular Dystrophy, leukodystrophies, neuronal ceroid lipofuscinoses - these are progressive (CP is non-progressive; PVL-related diplegia is static) |
| Genetic / metabolic causes of motor delay | Inborn errors of metabolism, mucopolysaccharidoses, Down syndrome with motor delay, chromosomal disorders |
| Other CP subtypes | Dyskinetic/athetoid CP, ataxic CP, spastic hemiplegia, spastic quadriplegia (these have different pathology and different Ayurvedic correlations) |
| Mixed CP | Mixed variety with significant dyskinetic component excluded (different Dosha profile) |
| Active infectious disease | Active tuberculosis, meningitis, encephalitis (Vyadhija Phakka from ongoing infection must be treated differently) |
| Uncontrolled seizures | Poor controlled epilepsy, recurrent status epilepticus, intractable or complex seizures (safety and confounding concern) |
| Severe congenital malformations | Congenital heart disease, major structural brain malformations (holoprosencephaly, lissencephaly) causing motor delay - different etiology from PVL |
B. Severity / Functional Exclusions
| Category | Criterion |
|---|---|
| Severe motor handicap with fixed deformity | Long-standing spasticity with irreversible contractures or bony deformities not amenable to improvement (e.g., established hip dislocation, severe scoliosis) |
| Severe cognitive impairment | Profound intellectual disability where functional motor assessment is impossible |
| GMFCS Level V | Non-ambulatory patients with total body involvement and dependent positioning (treatment goals are different and Ayurvedic Panchakarma risk is higher) |
| Severe communication barrier | Inability to assess response to treatment due to absent communication in older children |
C. Systemic Disease Exclusions
- Active systemic illness at time of enrollment: Nephrotic syndrome, juvenile diabetes mellitus, hepatic disease, severe malnutrition (confounding factors on treatment response and safety)
- Congenital heart disease (risk during Panchakarma/Swedana procedures)
- Haematological disorders (relevant if Raktamokshana or invasive Panchakarma considered)
D. Ayurvedic Exclusions
| Ayurvedic Condition | Reason for Exclusion |
|---|---|
| Kshiraja Phakka (pure breast milk-related nutritional type) | This is Rickets/PEM spectrum, not PVL - different pathology and treatment |
| Balashosha (childhood wasting due to primary tuberculosis) | Different from PVL-Phakka; has Kapha + Pitta predominance, not purely Vata |
| Jadata (pure intellectual/mental disability without motor involvement) | Majjavaha Srotodushti without Mamsavaha - does not fit the Phakka motor profile |
| Pakshavadha / Ekangaroga (hemiplegia / monoplegia) | Unilateral involvement - does not fit the bilateral diplegia pattern of Phakka |
| Atibalashosha / Marasmus in terminal stage | Irreversible Dhatu Kshaya - poor prognosis, beyond scope of Phakka-PVL treatment |
| Active Jwara (fever/infection) at time of treatment | Contraindication to Panchakarma; must be deferred until afebrile |
| Cases with recent Shodhana (purification) therapy | Within 1 month of previous Panchakarma; body not yet stabilized |
E. Exclusion for Specific Interventions (Panchakarma)
- Children with skin diseases or open wounds at treatment sites (Abhyanga/Udwartana contraindicated)
- Severely undernourished child (BMI/weight severely below normal) - Shodhana procedures are contraindicated; Shamana (palliative) therapy preferred first
- Age below 1 year - most Panchakarma procedures are not appropriate; limited to internal medications and Abhyanga only
- History of hypersensitivity to oils or herbal preparations to be used
SUMMARY TABLE
| Domain | INCLUSION | EXCLUSION |
|---|---|---|
| Age | 1-12 years | <1 year or >12 years |
| CP type | Spastic diplegia (legs > arms) | Dyskinetic, ataxic, hemiplegic, quadriplegic, mixed |
| MRI | PVL changes confirmed | Normal MRI with unknown etiology (may be genetic) |
| Birth history | Prematurity / perinatal asphyxia | Term birth with unknown etiology (genetic excluded) |
| Motor | GMFCS I-IV, some walking potential | GMFCS V, totally non-ambulatory + fixed deformities |
| Seizures | Controlled epilepsy | Poorly controlled / intractable seizures |
| Systemic | Otherwise healthy | Active TB, CHD, DM, nephrotic syndrome |
| Progressive? | Non-progressive (static) lesion | Any progressive neurological disease |
| Phakka type | Garbhaja / Vyadhija Phakka | Kshiraja Phakka (nutritional only) |
| Dosha | Vata-predominant (Kaphavrita Vata) | Primarily Pitta or Kapha predominant |
| Consent | Parents willing and able | Parents non-compliant or refusing |
Rationale for Key Decisions
-
Why exclude GMFCS V? - In PVL-based spastic diplegia, GMFCS I-IV cases retain some ambulation potential. Phakka's core definition is reversible walking inability ("Sakrud Gacchati" - can move with effort). GMFCS V represents total body involvement closer to Sarvanga Vata Vyadhi than Phakka.
-
Why exclude Kshiraja Phakka? - Its pathology is nutritional (Rasavaha/Asthivaha Srotodushti from poor breast milk), not neural (Majjavaha Srotodushti from ischemic white matter injury). The treatment principles and Dhatu targets differ completely.
-
Why exclude progressive disorders? - CP (including PVL-based diplegia) is by definition non-progressive. The brain lesion is static. Progressive conditions (SMA, dystrophies) mimic Phakka clinically but worsen over time - this violates Kashyapa's implicit assumption of a fixed/treatable condition.
-
Why require MRI confirmation of PVL? - Without imaging, spastic diplegia may be due to cortical malformations, genetic white matter disorders (leukodystrophies), or spinal cord lesions - none of which map to Garbhaja/Vyadhija Phakka pathophysiology. MRI confirmation anchors the Ayurvedic-modern correlation to a specific, definable lesion.