Learn ecg 10 common
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram common patterns interpretation
Finding Sources
Finding Sources
Finding Sources
Searching Images
normal sinus rhythm ECG waveform PQRST
Reading File
Finding Sources
Finding Sources
Searching Images
atrial fibrillation ECG irregularly irregular rhythm
Searching Images
STEMI ST elevation myocardial infarction ECG 12-lead
Searching Images
ventricular tachycardia fibrillation ECG wide complex
Searching Images
left bundle branch block right bundle branch block ECG
Searching Images
complete heart block third degree AV block ECG
Searching Images
atrial flutter sawtooth waves ECG
Searching Images
sinus bradycardia tachycardia ECG rate
Searching Images
Wolff-Parkinson-White WPW delta wave ECG short PR
I now have rich content from the medical library and images for all 10 common ECG patterns. Let me compile the comprehensive guide.
🫀 10 Common ECG Patterns — A Complete Learning Guide
How to Read an ECG: The Basics First
Paper speed: 25 mm/sec → each small box = 0.04 s; each large box = 0.2 s
Heart rate (quick): 300 ÷ number of large boxes between R waves
The PQRST sequence:
- P wave — atrial depolarization (SA node → atria)
- PR interval — AV nodal conduction delay (normal: 0.12–0.20 s)
- QRS complex — ventricular depolarization (normal: < 0.12 s)
- ST segment — early repolarization (should be isoelectric)
- T wave — ventricular repolarization
"Electrical signals are transmitted from the Purkinje system to individual ventricular cardiomyocytes. The spread of depolarization to the ventricular myocardium is exhibited as the QRS complex on the ECG. Depolarization is followed by ventricular repolarization and the appearance of the T wave." — Miller's Anesthesia, 10e
1. Normal Sinus Rhythm (NSR)
Rate: 60–100 bpm
Key features:
- Regular P waves before every QRS (upright in II, inverted in aVR)
- PR interval 0.12–0.20 s
- Narrow QRS < 0.12 s
- Regular R-R intervals
Clinical significance: The baseline from which all abnormalities are compared.
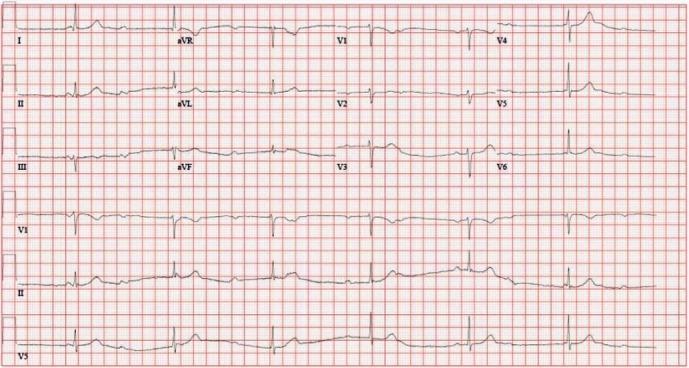
2. Sinus Bradycardia
Rate: < 60 bpm
Key features:
- Normal P-QRS-T morphology
- Regular rhythm, just slower
- All other intervals normal
Causes: Athletes, hypothyroidism, beta-blockers, inferior MI, increased vagal tone
Treat if: Symptomatic (dizziness, syncope, hypotension) → Atropine, then pacing
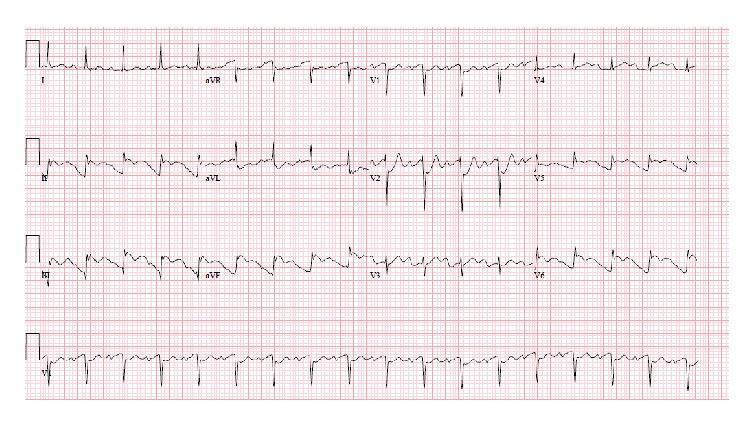
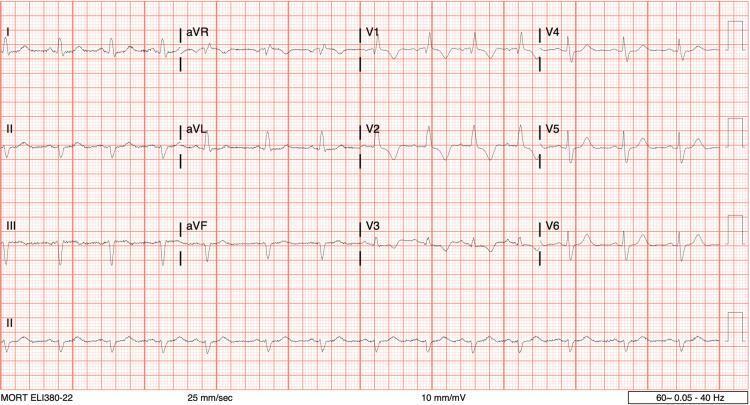
3. Atrial Fibrillation (AF)
Rate: Ventricular rate variable (usually 100–160 bpm if uncontrolled)
Key features:
- No P waves — replaced by chaotic fibrillatory (f) waves, best seen in V1
- Irregularly irregular R-R intervals (hallmark)
- Narrow QRS (unless aberrant conduction)

Causes: Hypertension, valvular disease, hyperthyroidism, alcohol
Key risks: Stroke (thrombus in LAA) → anticoagulate if CHA₂DS₂-VASc ≥ 2 (men) / ≥ 3 (women)
Treatment: Rate control (beta-blocker, diltiazem) or rhythm control (cardioversion, amiodarone)
4. Atrial Flutter
Rate: Atrial ~300 bpm; ventricular usually 150 bpm (2:1 block)
Key features:
- Classic sawtooth flutter waves (F-waves) at 300/min — most visible in II, III, aVF
- Regular ventricular rate (fixed AV conduction ratio, e.g., 2:1, 3:1, 4:1)
- No isoelectric baseline between F-waves
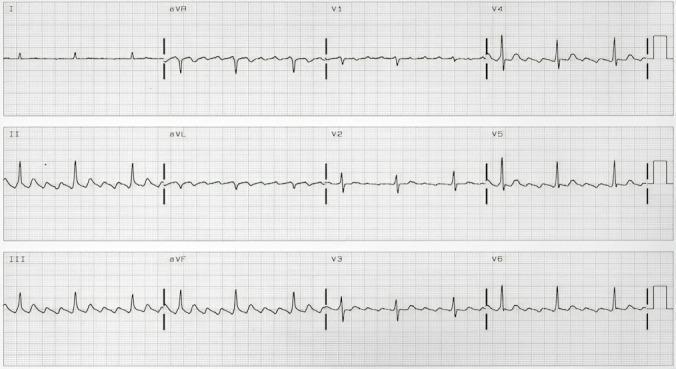
Mechanism: Macro-reentrant circuit around tricuspid valve (cavotricuspid isthmus)
Treatment: Rate control; cardioversion; catheter ablation (highly effective)
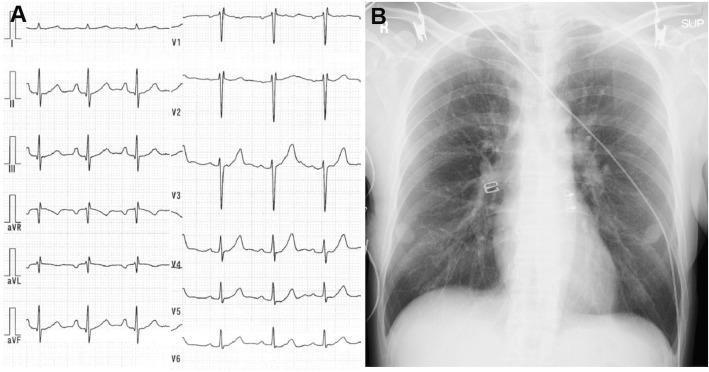
5. ST-Elevation MI (STEMI)
Key features:
- ST elevation ≥ 1 mm in ≥ 2 contiguous limb leads, or ≥ 2 mm in V1–V3
- Reciprocal ST depression in opposite leads
- Hyperacute (peaked) T waves early; Q waves develop later
- Location tells you the artery:
| Territory | Leads | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V3 | RCA/LCx |

Emergency action: Activate cath lab — door-to-balloon ≤ 90 min
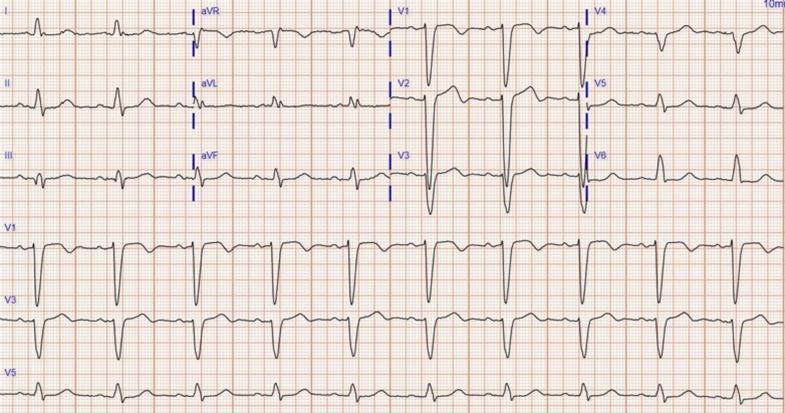
6. Left Bundle Branch Block (LBBB)
Key features:
- Broad QRS > 0.12 s (usually > 0.14 s)
- Broad, notched R in I, aVL, V5–V6 ("M" or "W" pattern)
- Deep QS in V1 (no r wave)
- Secondary ST/T discordance (T wave opposite QRS direction)
- New LBBB + chest pain = treat as STEMI equivalent
Causes: Hypertension, dilated cardiomyopathy, anterior MI, cardiac surgery
7. Right Bundle Branch Block (RBBB)
Key features:
- Broad QRS > 0.12 s
- rSR' ("rabbit ears") in V1 — terminal R' wave
- Broad/slurred S wave in I, V5, V6
- T-wave inversion in V1–V3 (secondary change)
Causes: Often normal variant; also PE (acute RBBB), RV hypertrophy, anterior MI
Memory: LBBB = WiLLiaM (W in V1, M in V5), RBBB = MaRRoW (M in V1, W in V5)
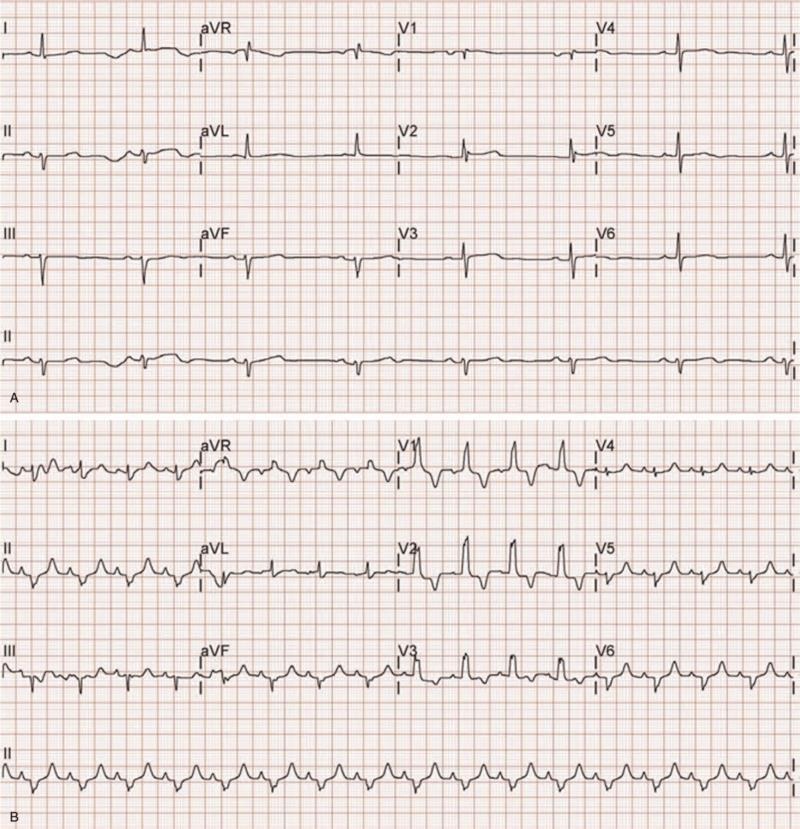
8. Third-Degree (Complete) Heart Block
Key features:
- Complete AV dissociation — P waves and QRS complexes are independent
- Atrial rate > ventricular rate
- Regular P-P intervals, regular R-R intervals (but NO relationship between them)
- Escape rhythm: junctional (narrow QRS ~40–60 bpm) or ventricular (wide QRS ~20–40 bpm)

Causes: Inferior MI (RCA), Lyme disease, drugs (digoxin, beta-blockers), fibrosis
Treatment: Atropine (temporary), urgent transvenous/permanent pacemaker
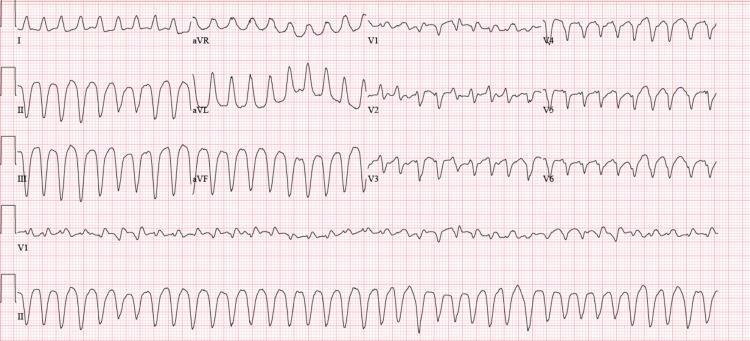
9. Ventricular Tachycardia / Fibrillation
Ventricular Tachycardia (VT)
- Rate: 100–250 bpm
- Broad QRS > 0.12 s (usually > 0.14 s)
- Regular (monomorphic VT) or irregular (polymorphic VT/Torsades)
- AV dissociation, fusion beats, capture beats (diagnostic)
Ventricular Fibrillation (VF)
- Chaotic, irregular waveforms — no discernible P, QRS, or T
- No cardiac output → cardiac arrest
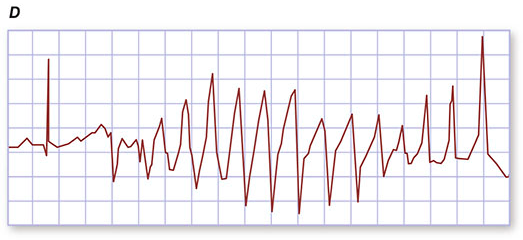
VT: Amiodarone, cardioversion if unstable; VF: Immediate defibrillation
Torsades (prolonged QT): Stop offending drug, IV Magnesium 2 g
10. Wolff-Parkinson-White (WPW) Syndrome
Key features:
- Short PR interval < 0.12 s (bypasses AV nodal delay)
- Delta wave — slurred upstroke of QRS (pre-excitation)
- Widened QRS (> 0.10 s due to delta wave)
- Risk of rapid AF over accessory pathway → hemodynamic collapse

DANGER: Never give AV-nodal blocking drugs (adenosine, digoxin, verapamil, beta-blockers) in WPW + AF → can precipitate VF
Treatment: Procainamide (acute); radiofrequency ablation of accessory pathway (definitive)
Quick Reference Summary Table
| # | Pattern | Rate | P Waves | QRS | Key Feature |
|---|---|---|---|---|---|
| 1 | Normal Sinus Rhythm | 60–100 | Normal, upright | Narrow | Baseline normal |
| 2 | Sinus Bradycardia | < 60 | Normal | Narrow | Slow but regular |
| 3 | Atrial Fibrillation | Variable | Absent (f-waves) | Narrow | Irregularly irregular |
| 4 | Atrial Flutter | ~150 (2:1) | Sawtooth F-waves | Narrow | Regular saw pattern |
| 5 | STEMI | Variable | Normal | Narrow (initially) | ST elevation + reciprocal ↓ |
| 6 | LBBB | Variable | Normal | Wide (M in V5) | No r in V1, M in V6 |
| 7 | RBBB | Variable | Normal | Wide (rSR' V1) | Rabbit ears V1, S wave I/V6 |
| 8 | 3° Heart Block | Atrial > Vent | Dissociated | Wide (escape) | P & QRS independent |
| 9 | VT/VF | 100–250/chaotic | Often none | Wide/chaotic | Emergency — shock/defib |
| 10 | WPW | Variable | Normal | Wide (delta) | Short PR + delta wave |
A Systematic Approach (Never Miss Anything)
- Rate — 300 ÷ large boxes between R-R
- Rhythm — regular or irregular?
- Axis — normal (I ↑, aVF ↑), LAD, RAD
- P waves — present? morphology? 1:1 with QRS?
- PR interval — short (< 0.12), normal, long (> 0.20)?
- QRS duration — narrow (< 0.12) or wide (> 0.12)?
- ST segment — elevation, depression, or flat?
- T waves — upright, inverted, peaked?
- QT interval — corrected QTc (normal < 440 ms men, < 460 ms women)
Sources: Miller's Anesthesia 10e; Fuster and Hurst's The Heart 15e; Tintinalli's Emergency Medicine; Braunwald's Heart Disease; Harrison's Principles of Internal Medicine 21e
This is a shared conversation. Sign in to Orris to start your own chat.