Rheumatoid fever
Reading File
Finding Sources
Searching PubMed
"rheumatic fever"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from two authoritative sources. Let me compile the full answer.
Acute Rheumatic Fever (ARF)
Acute rheumatic fever is a delayed, non-suppurative inflammatory complication of Group A Streptococcus (GAS) pharyngitis. It is called "rheumatic" because it principally affects the joints and heart, and "fever" because fever is nearly universal. It does NOT follow streptococcal skin infections (impetigo).
Epidemiology
- Most common in children aged 5-15 years (rare before age 3, infrequent after 15)
- Occurs equally in males and females; however, rheumatic heart disease (the chronic sequela) is more common in women
- ARF develops in approximately 1.6-2.5% of patients with streptococcal pharyngitis
- Peak prevalence of rheumatic heart disease is in the 3rd and 4th decades (due to recurrent damage)
- More common in developing countries and overcrowded settings
Pathobiology (Molecular Mimicry)
The mechanism is not direct infection but an aberrant immune response:
| Manifestation | Mechanism |
|---|---|
| Carditis | Antibody-binding + T-cell infiltration of the heart |
| Arthritis | Immune complex deposition in joints |
| Chorea | Antibody binding to basal ganglia |
| Skin lesions | Delayed hypersensitivity reactions |
Structural similarities between GAS proteins (particularly M protein) and human cardiac proteins trigger cross-reactive antibodies and T cells - "molecular mimicry."
Clinical Manifestations
Symptoms begin approximately 2-3 weeks after GAS pharyngitis (average 18.6 days). Chorea may be delayed 4-8 weeks. Symptoms typically persist 2-4 weeks.
Major Manifestations (Mnemonic: JONES)
| Feature | Frequency | Notes |
|---|---|---|
| Joints (migratory polyarthritis) | ~75% | Most common; additive pattern also occurs; knees (76%), ankles (50%), elbows/wrists |
| O (cardiOtis) | 15-91% | Pancarditis; mitral valve most affected; Carey-Coombs murmur, mitral regurgitation |
| Nodules (subcutaneous) | <10% | 0.5-2 cm, painless, over bony prominences/extensor tendons |
| Erythema marginatum | <10% | Pink, non-pruritic, blanching, serpiginous pattern on trunk and proximal limbs |
| Sydenham's chorea | ~30% | Involuntary, non-rhythmic, purposeless movements; worse on one side; stops during sleep |
Fever is present in >90% of cases.
Carditis Details
- Affects all layers: pericardium, myocardium, endocardium (pancarditis)
- Mitral valve affected in almost all cases of carditis
- Aortic valve involved in ~20-30%
- Classic murmurs:
- Mitral regurgitation: high-pitched, blowing, holosystolic, apical
- Carey-Coombs murmur: low-pitched, apical, mid-diastolic flow murmur
- Aortic regurgitation: high-pitched, decrescendo, diastolic
- Heart failure is the most life-threatening feature
- Subclinical carditis can be detected by echocardiography (Doppler) even without audible murmur
Diagnosis - Revised Jones Criteria (2015 AHA)
There is no definitive test - it is a diagnosis of exclusion. Diagnosis requires evidence of preceding GAS infection PLUS fulfillment of the Jones criteria.
Evidence of preceding GAS infection:
- Positive throat culture or rapid strep test
- Elevated/rising ASO (anti-streptolysin O) or anti-DNase B titers
For Initial ARF:
- 2 major criteria, OR
- 1 major + 2 minor criteria
For Recurrent ARF:
- 2 major, OR 1 major + 2 minor, OR 3 minor criteria
| Criteria | Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|---|
| Major | Carditis (clinical/echocardiographic), polyarticular arthritis, chorea, erythema marginatum, subcutaneous nodules | Same + monoarticular arthritis counts |
| Minor | Polyarthralgia, fever ≥38.5°C, ESR ≥60 mm and/or CRP ≥3.0 mg/dL, prolonged PR interval | Monoarthralgia, fever ≥38.5°C, ESR ≥30 mm and/or CRP ≥3.0 mg/dL, prolonged PR interval |
Low-risk = ARF incidence <2/100,000 school-aged children/year or RHD prevalence ≤1/1000/year
Lab findings: Elevated ESR/CRP, normochromic normocytic anemia, leukocytosis, prolonged PR interval on ECG.
Treatment
1. Eradication of GAS (Primary Treatment)
- Benzathine penicillin G 1.2 million units IM (single dose) - preferred
- Oral penicillin V 250 mg BID x 10 days (alternative)
- Oral macrolide (e.g., azithromycin) if penicillin-allergic
2. Anti-inflammatory Therapy
| Symptom | Drug | Dose |
|---|---|---|
| Arthritis/fever | Aspirin (first-line) | 80-100 mg/kg/day divided; max 4-8 g/day |
| Arthritis/fever | Naproxen (alternative) | 10-20 mg/kg/day divided BID |
| Severe carditis | Corticosteroids (prednisone) | Used for severe carditis/HF; taper after 2-3 weeks |
| Chorea | Carbamazepine or valproate | Haloperidol if severe |
Continue NSAIDs for at least 1 month (or until inflammatory markers normalize). Aspirin response is typically rapid - lack of response should prompt reconsideration of diagnosis.
3. Secondary Prophylaxis (CRITICAL - prevents recurrence and RHD)
- Benzathine penicillin G 1.2 million units IM every 4 weeks (or every 3 weeks in high-risk patients)
- Alternative: oral penicillin V 250 mg BID or oral macrolide
Duration of prophylaxis:
| Category | Duration |
|---|---|
| ARF without carditis | 5 years or until age 21 (whichever is longer) |
| ARF with carditis, no residual RHD | 10 years or until age 21 |
| ARF with carditis + residual RHD | ≥10 years or until age 40 (sometimes lifelong) |
Key Points
- The arthritis of ARF is never radiographically destructive (unlike RA)
- "Loves the joints, licks the heart" - arthritis is transient; cardiac damage is cumulative with each recurrence
- Sydenham's chorea stops during sleep (distinguishes from tics)
- Subclinical carditis (echocardiographic only) was added to the 2015 revised Jones criteria
- The NSAIDs work so well for arthritis that prompt response is virtually diagnostic; if no response to NSAIDs, reconsider diagnosis
- Jaccoud's arthropathy (non-erosive, deforming) can occur after multiple recurrent articular attacks
Recent evidence (2024-2025): A Cochrane systematic review (PMID 39312290) confirmed long-term benzathine penicillin G prophylaxis is effective for preventing recurrence and progression to rheumatic heart disease. A 2025 meta-analysis (PMID 40333929) examined severe adverse reactions to benzathine penicillin G - the overall risk of severe reactions is low, supporting its continued use for prophylaxis.
- Goldman-Cecil Medicine, International Edition (2-Vol Set)
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
Diagnosis of it
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Excellent - I have the Jones Criteria evolution chart. Now I have everything needed for a thorough answer on the diagnosis of rheumatic fever.
Diagnosis of Acute Rheumatic Fever (ARF)
There is no single confirmatory test for ARF. Diagnosis is clinical, based on a structured set of criteria, supported by laboratory and imaging evidence. It is fundamentally a diagnosis of exclusion after ruling out other conditions.
Step 1 - Establish Evidence of Preceding GAS Infection
This is mandatory - the criteria cannot be applied without it.
| Test | Details |
|---|---|
| Throat culture | Positive for Group A Streptococcus (GAS); may be negative if infection has cleared |
| Rapid antigen detection test (RADT) | Quick bedside test; lower sensitivity than culture |
| Anti-streptolysin O (ASO) titer | Most commonly used serologic test; detects recent GAS pharyngitis; rises 1-3 weeks after infection, peaks at 3-5 weeks. False elevation occurs when serum cholesterol is high (e.g., nephrotic syndrome) |
| Anti-DNase B | More sensitive than ASO, especially for skin infections and chorea (ASO may already be declining by the time chorea appears) |
| Anti-streptokinase / Anti-hyaluronidase | Used when ASO and anti-DNase B are inconclusive |
Note: In Sydenham's chorea (which appears 4-8 weeks after pharyngitis), ASO titers may no longer be elevated by the time chorea presents. Anti-DNase B persists longer and is more useful.
Step 2 - Apply the Revised Jones Criteria (2015 AHA)
The Jones Criteria have evolved since 1944. The 2015 revision introduced two key advances:
- Echocardiographic (subclinical) carditis counts as a major criterion
- Risk-stratification by population (low vs. moderate/high risk)
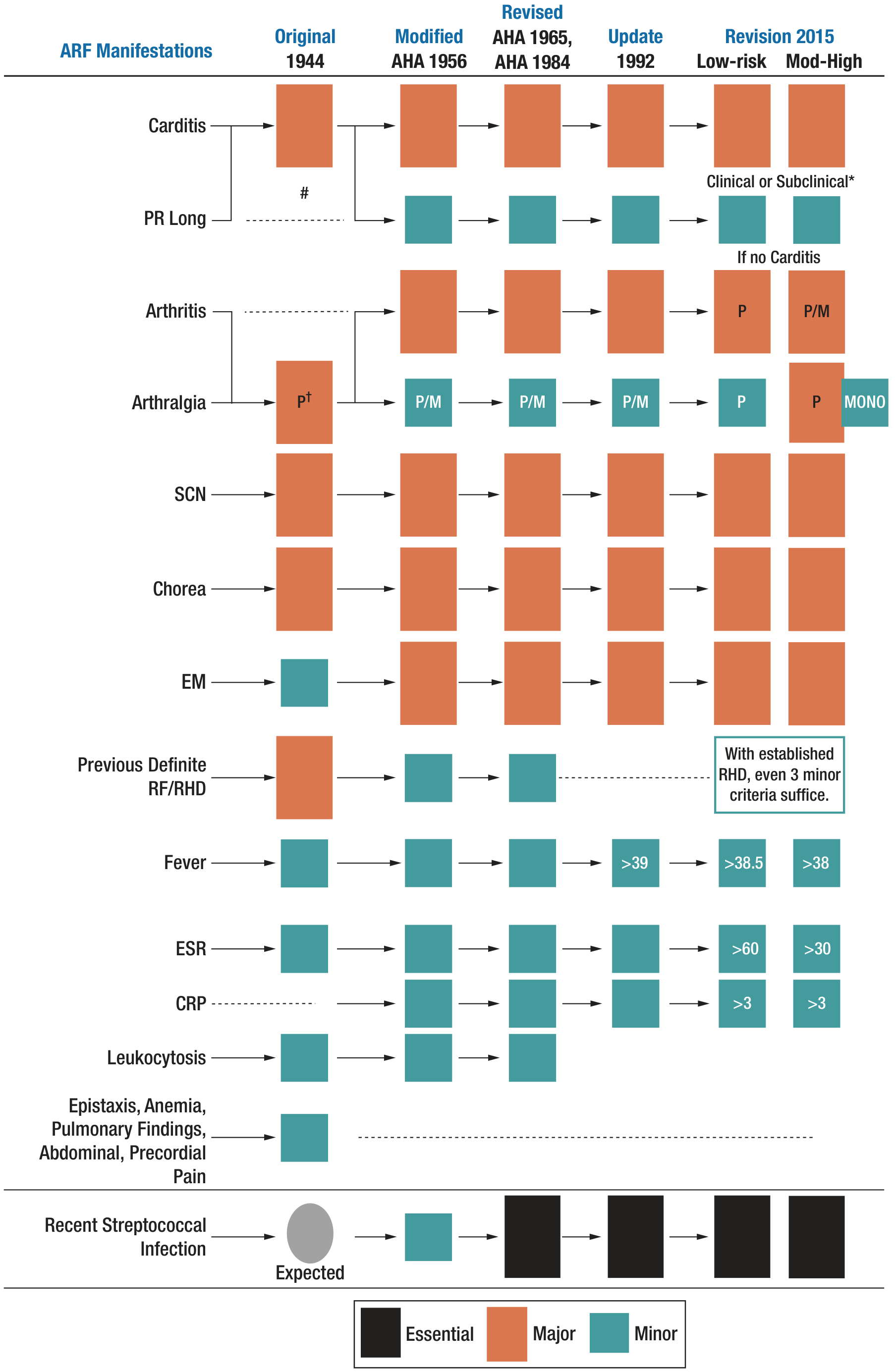
Diagnostic Thresholds
| Scenario | Requirement |
|---|---|
| Initial ARF | 2 major criteria, OR 1 major + 2 minor criteria |
| Recurrent ARF (established RHD) | 2 major, OR 1 major + 2 minor, OR 3 minor criteria |
| Chorea alone | Sufficient for diagnosis (stand-alone major criterion) |
| Subclinical carditis alone | Sufficient if 4 echocardiographic sub-criteria are met |
Major Criteria
| Criterion | Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|---|
| Carditis | Clinical or subclinical (echocardiographic) | Same |
| Arthritis | Polyarticular only | Mono- or polyarticular |
| Chorea | Yes | Yes |
| Erythema marginatum | Yes | Yes |
| Subcutaneous nodules | Yes | Yes |
Minor Criteria
| Criterion | Low-Risk | Moderate/High-Risk |
|---|---|---|
| Arthralgia | Polyarthralgia | Monoarthralgia |
| Fever | ≥38.5°C | ≥38.0°C |
| ESR | ≥60 mm/hr | ≥30 mm/hr |
| CRP | ≥3.0 mg/dL | ≥3.0 mg/dL |
| Prolonged PR interval | Yes (if carditis is NOT the major criterion) | Same |
Low-risk = ARF incidence <2/100,000 school-age children/year OR RHD prevalence ≤1/1,000/year (applies to developed countries). High-risk = developing countries, Indigenous communities.
Step 3 - Investigations in Practice
Inflammatory / Hematologic
| Test | Expected Finding |
|---|---|
| ESR | Elevated |
| CRP | Elevated |
| CBC | Normochromic normocytic anemia, leukocytosis |
| Blood culture | Negative (rules out septic arthritis, infective endocarditis) |
Cardiac Investigations
| Test | What to Look For |
|---|---|
| ECG | Prolonged PR interval (first-degree AV block) - minor criterion; rarely 2nd/3rd degree block requiring temporary pacing |
| Echocardiography (MANDATORY in all suspected ARF) | Valvular regurgitation (mitral most common, aortic in 20-30%); subclinical carditis; pericardial effusion; morphologic changes (leaflet thickening, restricted mobility, chordal involvement) |
| Chest X-ray | Cardiomegaly if significant carditis/HF; pulmonary edema if HF |
Subclinical Carditis - Echocardiographic Criteria (all 4 required)
To diagnose subclinical (echocardiographic-only) carditis, ALL of these must be present:
- Pathologic mitral regurgitation by Doppler
- At least 2 jet features present (seen in ≥2 views, mosaic, >2.5 cm in length, velocity >3 m/s, pan-systolic)
- Pathologic aortic regurgitation (if aortic valve involved)
- Absence of physiologic (normal variant) regurgitation
Synovial Fluid (if joint aspirated)
- Sterile (no organisms)
- Lymphocyte predominance
- Rules out septic arthritis
Step 4 - Differential Diagnosis
Conditions that can mimic ARF and must be excluded:
| Condition | Distinguishing Features |
|---|---|
| Juvenile Idiopathic Arthritis (JIA) | Sustained arthritis >6 weeks, no GAS evidence, different pattern |
| Septic arthritis | Single joint, very elevated WBC in synovial fluid, positive culture |
| Reactive arthritis (post-enteric/urogenital) | HLA-B27 association, urethritis, conjunctivitis (Reiter's triad), different trigger |
| Infective endocarditis | Positive blood cultures, Osler nodes, Janeway lesions, emboli |
| Lyme disease | Tick exposure, erythema migrans, Borrelia serology; carditis can mimic ARF |
| Viral arthritis (parvovirus B19, rubella) | Symmetrical small joint involvement, viral serology |
| Systemic Lupus Erythematosus | ANA positive, malar rash, renal involvement, positive anti-dsDNA |
| Kawasaki disease | Age <5 years, conjunctivitis, lip/tongue changes, desquamation |
| Still's disease | Quotidian fever, salmon-colored rash, hepatosplenomegaly |
| Viral myocarditis | No preceding pharyngitis, no arthritis, no ASO rise |
Key clinical clue: Prompt, dramatic response to NSAIDs is virtually diagnostic of ARF arthritis. Lack of NSAID response should prompt reconsideration of the diagnosis.
Diagnostic Pitfalls
- Up to 50% of preceding GAS pharyngitis is asymptomatic - absence of sore throat history does NOT exclude ARF
- ASO titers may be falsely negative in chorea (too late in the illness) - test anti-DNase B
- Subclinical carditis (echocardiographic only) missed if echo not done - this is now a major criterion
- In high-risk populations, monoarthritis and monoarthralgia count - using low-risk criteria will miss cases
- Myocarditis without valvulitis should NOT be attributed to ARF
- The arthritis of ARF is never radiographically erosive/destructive - if bone erosions are present, think JIA or RA
Sources:
- Goldman-Cecil Medicine, International Edition
- Fuster and Hurst's The Heart, 15th Edition
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Edition
This is a shared conversation. Sign in to Orris to start your own chat.