Thromboelastography - MD ANAESTHESIA PG EXAM - 30 marks major answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
thromboelastography TEG viscoelastic hemostatic assay
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
thromboelastography TEG parameters trace interpretation anaesthesia MD exam
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, high-quality content from Miller's Anesthesia and Barash Clinical Anesthesia textbooks, plus excellent diagrams. I have everything needed to write a thorough 30-mark MD Anaesthesia PG exam answer. Let me now compose the complete answer.
Thromboelastography (TEG) - MD Anaesthesia PG Examination Answer
Introduction
Thromboelastography (TEG) is a point-of-care viscoelastic hemostatic assay (VHA) that measures the global viscoelastic properties of whole blood during clot formation and fibrinolysis under low shear stress. First described by Hartert in 1948, it has undergone a major resurgence in perioperative medicine as it provides real-time, bedside monitoring of the entire hemostatic process - from initial fibrin strand generation through clot retraction and fibrinolysis - in a single test.
Miller's Anesthesia, 10e | Barash Clinical Anesthesia, 9e
Principle and Mechanism
How TEG Works
A small sample of whole blood (0.35 mL) is placed into a disposable cuvette maintained at 37°C within the instrument. The cuvette continuously rotates around a fixed axis through an arc of approximately 4-5 degrees at a rate of 1 cycle per 10 seconds (simulating sluggish venous flow).
A sensor "piston" (pin) attached by a torsion wire to an electronic recorder is lowered into the blood. An activator (most commonly kaolin or celite) initiates clotting.
- Before clotting begins: the cuvette rotates freely; no motion is transferred to the pin.
- As clot forms: fibrin strands bridge the cuvette wall and the pin; the pin begins to move with the cuvette.
- As clot strengthens: increasing resistance is transferred through the torsion wire to the recorder, generating a characteristic waveform.
- As fibrinolysis occurs: the clot breaks down, the pin slips, and the waveform amplitude decreases.
The magnitude of pin motion is directly proportional to clot strength.
Barash Clinical Anesthesia, 9e, p. 1278
TEG Tracing and Parameters
The characteristic spindle-shaped (or "cigar-shaped") waveform generated by TEG is described by the following parameters:
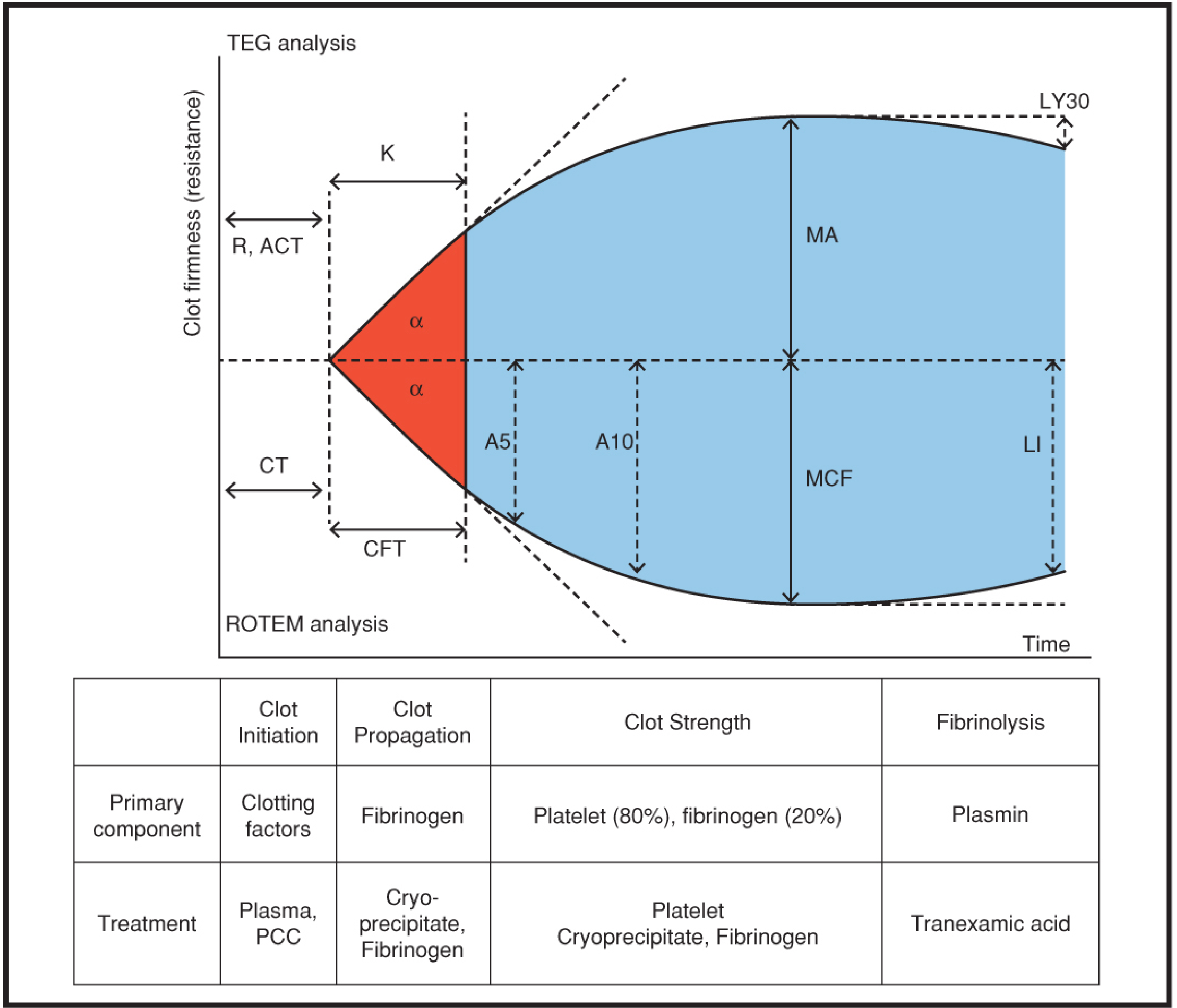
Figure: Schematic TEG/ROTEM tracing and parameters - Barash Clinical Anesthesia, 9e
TEG Parameters (Normal Values - Kaolin-Activated)
| Parameter | Full Name | What it Measures | Normal Value | Prolonged/Abnormal by |
|---|---|---|---|---|
| R | Reaction Time | Time to initial fibrin formation (clot initiation) | 5-10 min | Factor deficiency, heparin, anticoagulants |
| K | Kinetics Time | Time from clot initiation to 20 mm amplitude (clot propagation speed) | 1-3 min | Low fibrinogen, factor deficiency, thrombocytopenia |
| α (alpha angle) | Alpha Angle | Rate of clot formation (tangent to the curve at 2 mm amplitude) | 53-72° | Low fibrinogen, thrombocytopenia |
| MA | Maximum Amplitude | Maximum clot strength/firmness | 50-70 mm | Platelet dysfunction/thrombocytopenia (↓), hypercoagulability (↑) |
| LY30 | Lysis at 30 min | % reduction in area under curve at 30 min compared to MA | < 7.5% | Fibrinolysis (if elevated) |
| CL30/CL60 | Clot Lysis | % decrease in amplitude at 30 or 60 min | < 15% | Primary fibrinolysis |
| EPL | Estimated % Lysis | Predicted % lysis before 30 min | < 15% | Hyperfibrinolysis |
Miller's Anesthesia, 10e, p. 6747 | Barash Clinical Anesthesia, 9e, p. 1278
Interpretation of Parameters by Phase
| Phase | Parameter | Primary Component Responsible | Treatment if Abnormal |
|---|---|---|---|
| Clot Initiation | R (TEG) / CT (ROTEM) | Clotting factors | FFP, PCC |
| Clot Propagation | K, α-angle (TEG) / CFT, α (ROTEM) | Fibrinogen | Cryoprecipitate, Fibrinogen concentrate |
| Clot Strength | MA (TEG) / MCF (ROTEM) | Platelets (80%), Fibrinogen (20%) | Platelets, Cryoprecipitate, Fibrinogen |
| Fibrinolysis | LY30 (TEG) / LI30 (ROTEM) | Plasmin | Tranexamic acid, Epsilon-aminocaproic acid |
ROTEM vs TEG: Comparison
Rotational Thromboelastometry (ROTEM) is the main alternative to TEG. In ROTEM, the pin oscillates (not the cuvette), making it less susceptible to vibration artifacts.
| Feature | TEG | ROTEM |
|---|---|---|
| Manufacturer | Haemonetics (TEG 5000, TEG 6s) | TEM Systems (ROTEM delta, ROTEM sigma) |
| Cuvette motion | Cuvette rotates | Pin oscillates |
| Activator (standard) | Kaolin | Ellagic acid (INTEM), Tissue factor (EXTEM) |
| R equivalent | R (Reaction time) | CT (Coagulation time) |
| K equivalent | K (Kinetics) | CFT (Clot formation time) |
| MA equivalent | MA (Maximum amplitude) | MCF (Maximum clot firmness) |
| LY30 equivalent | LY30 | LI30 (Lysis index at 30 min) |
| Vibration sensitivity | Higher | Lower |
ROTEM-Specific Test Channels
| Channel | Activator | Assesses |
|---|---|---|
| EXTEM | Tissue factor + phospholipids | Extrinsic pathway, overall clot |
| INTEM | Ellagic acid | Intrinsic pathway, heparin effect |
| FIBTEM | Tissue factor + platelet inhibitor (cytochalasin D) | Fibrinogen contribution only |
| HEPTEM | Ellagic acid + heparinase | Distinguishes heparin effect from intrinsic factor deficiency |
| APTEM | Tissue factor + aprotinin | Differentiates hyperfibrinolysis |
Barash Clinical Anesthesia, 9e, p. 1278
Newer Devices
The TEG 6s (Haemonetics) uses a microfluidics-based resonance detection system - it vibrates a blood meniscus using frequencies of 20-500 Hz. As clot forms, clot-strength-specific resonance frequencies are detected by a photodetector and converted into TEG-equivalent units. This eliminates vibration artifact, reduces operator variability, and allows simultaneous multiple assays using cartridge-based technology.
The Quantra analyzer (HemoSonics) uses ultrasonic pulses to vibrate the blood sample and measures resonance to estimate shear modulus - providing clot stiffness, start of clot formation, and platelet/fibrinogen contributions.
Miller's Anesthesia, 10e, p. 6748
TEG Tracings in Various Pathological States
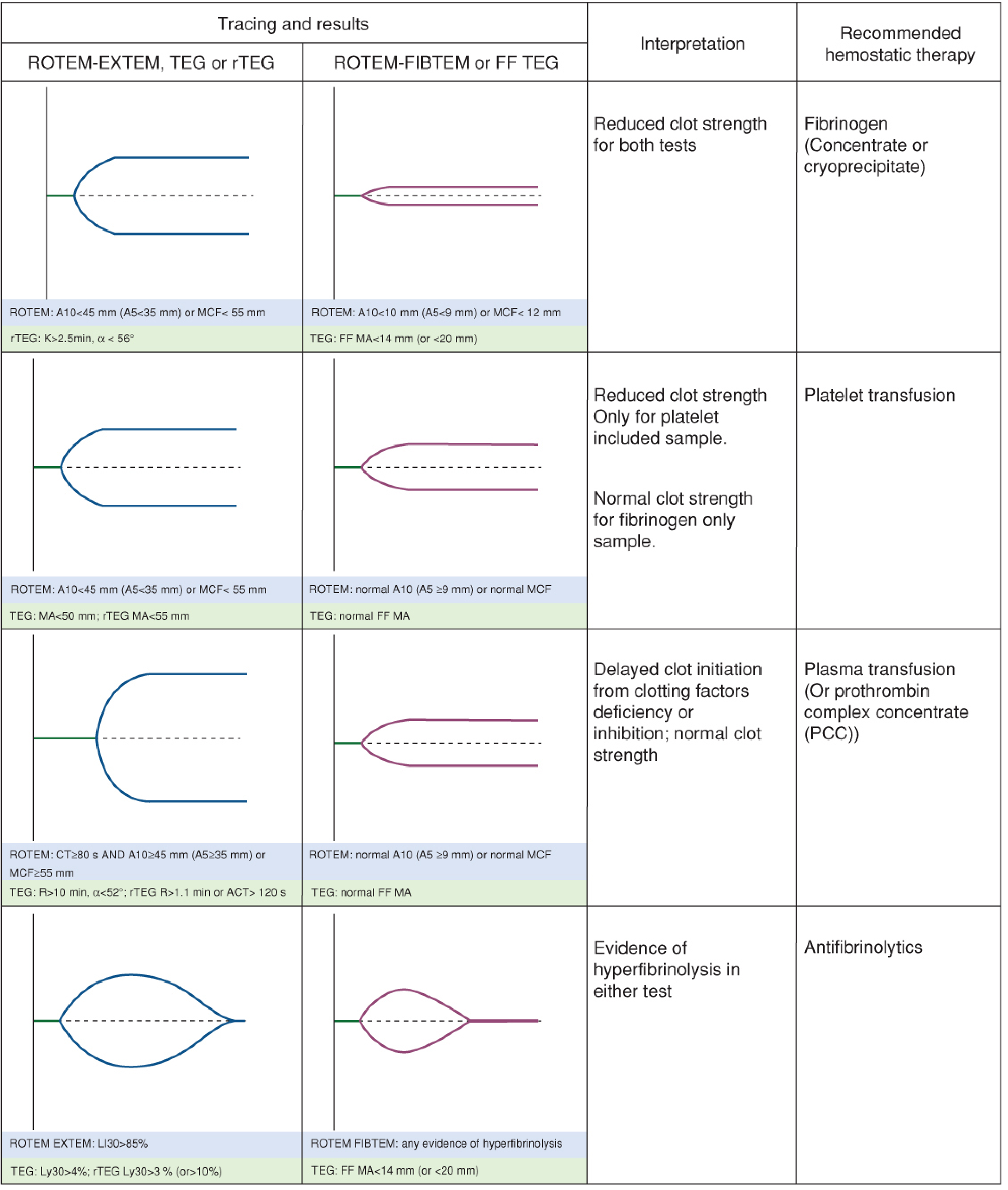
Figure: Schematic TEG/ROTEM tracings in various coagulopathies with recommended hemostatic therapy - Barash Clinical Anesthesia, 9e
Common Patterns
- Normal trace: Symmetric spindle shape, normal R, K, alpha, MA, minimal LY30
- Factor deficiency (e.g., hemophilia, warfarin): Prolonged R value (wide "gap" at start), prolonged K → FFP or PCC
- Thrombocytopenia / platelet dysfunction: Low MA, reduced alpha angle → Platelet transfusion
- Hypofibrinogenemia: Prolonged K, reduced alpha angle, low MA → Cryoprecipitate or fibrinogen concentrate; FIBTEM MCF reduced
- Hyperfibrinolysis (e.g., liver failure, trauma, abruption): LY30 >7.5%, clot "falls apart" - narrow trace that diminishes rapidly → Tranexamic acid, epsilon-aminocaproic acid
- Hypercoagulability: Short R and K, high MA, wide trace → Anticoagulation
- Heparin effect: Prolonged R/K (corrected in HEPTEM channel or with heparinase addition)
- DIC: Initially hypercoagulable then progresses to hypocoagulable with hyperfibrinolysis - evolving trace
Treatment Thresholds (TEG-Guided Transfusion Protocol)
| TEG Parameter | Threshold | Treatment |
|---|---|---|
| R > 10 min | Factor deficiency | FFP 10-15 mL/kg, or PCC |
| R > 15 min | Severe factor deficiency | 2 units FFP |
| α-angle < 45° | Fibrinogen deficiency | Cryoprecipitate (5-10 units or 0.06 units/kg) |
| MA < 40 mm | Severe thrombocytopenia | 1-2 units platelet apheresis |
| MA < 55 mm | Moderate thrombocytopenia/dysfunction | 1 unit platelet apheresis |
| LY30 ≥ 3-7.5% | Hyperfibrinolysis | Tranexamic acid 1 g IV |
PMC review (PMID not directly cited) | Barash 9e
Clinical Applications of TEG in Anaesthesia
1. Cardiac Surgery (Most Established)
TEG is most validated in cardiac surgery involving cardiopulmonary bypass (CPB).
- Detects heparin effect and residual heparin after protamine reversal
- Identifies platelet dysfunction from CPB
- Distinguishes surgical bleeding from coagulopathic bleeding
- Guides rational blood product use, reducing transfusion requirements
- Detects protamine excess
2. Liver Transplantation
- Detects hyperfibrinolysis (which is common and dramatic during the anhepatic phase)
- Guides fibrinogen and antifibrinolytic therapy
- Identifies the "rebound hypercoagulability" after reperfusion
- TEG-guided protocols significantly reduce blood product usage compared to INR/platelet-guided approaches (RCT evidence)
3. Trauma - Trauma-Induced Coagulopathy (TIC)
- Identifies early TIC: prolonged R, low MA, elevated LY30
- Rapid TEG (rTEG) provides actionable results within 5-10 minutes
- Guides massive transfusion protocols and damage control resuscitation
- Detects hyperfibrinolysis - a major contributor to traumatic coagulopathy
- Guides antifibrinolytic therapy (TXA) timing
4. Obstetric Haemorrhage
- Detects coagulopathy in postpartum haemorrhage (PPH)
- Guides management of placental abruption, HELLP syndrome, amniotic fluid embolism
- Some evidence for modest reduction in blood loss vs. conventional tests
5. Neuraxial Anaesthesia Decision-Making
- Assesses adequacy of reversal before neuraxial blocks in patients on anticoagulants
- Useful when timing of anticoagulant dosing is uncertain
6. Paediatric Cardiac Surgery and ECMO
- Guides anticoagulation monitoring on ECMO circuits
- Detects coagulopathy in complex paediatric cardiac repairs
7. Monitoring Anticoagulation
- Detects effect of unfractionated heparin (prolonged R, corrected with heparinase)
- Can detect effect of direct oral anticoagulants (DOACs) - though nonspecific
- Monitors reversal of anticoagulation
8. Other Applications
- Sepsis-associated coagulopathy
- Hepatic disease assessment
- Pre-operative risk stratification
- Monitoring fibrinolytic therapy
Advantages of TEG Over Conventional Coagulation Tests
| Feature | Conventional Tests (PT, aPTT, INR) | TEG/ROTEM |
|---|---|---|
| Sample | Citrated plasma | Whole blood |
| Turnaround time | 15-60 min | 20-40 min (actionable in 5-10 min) |
| Hyperfibrinolysis detection | No | Yes |
| Hypercoagulability detection | No | Yes |
| Platelet function | No | Partially (MA reflects platelet-fibrin interaction) |
| Fibrinolysis | Not in routine tests | Yes (LY30/LI30) |
| Real-time monitoring | No | Yes |
| Point-of-care | No | Yes |
| Warfarin detection | Yes | Unreliable |
| DOAC detection | No | Nonspecific |
| Primary hemostasis | No | No (limitation) |
| Cell-based coagulation model | Reflects plasma-based model only | Reflects cell-based model in vivo |
Barash Clinical Anesthesia, 9e, Table 53-3
Limitations of TEG
- Does not assess primary hemostasis: Cannot detect von Willebrand disease, platelet adhesion defects, or vascular endothelial function
- Sample heated to 37°C: Masks effects of hypothermia and hypocalcemia on coagulation
- Re-calcification of citrated blood: Does not reflect in vivo ionized calcium levels
- Cannot reliably detect Warfarin (INR-based assays remain superior)
- Nonspecific for DOACs: Cannot differentiate DOAC effect from TIC
- Vibration sensitivity: First-generation devices (TEG 5000) prone to vibration artifact
- Operator variability: High intra- and inter-operator variability with older devices; improved with cartridge-based TEG 6s
- Learning curve: Steep learning curve for both performance and interpretation
- Cost: More expensive than conventional coagulation tests
- Limited sensitivity for mild factor deficiencies: Some patients with mild hemophilia may have normal TEG
- Limited evidence in non-surgical patients: Most robust data in cardiac surgery; limited data in general ward patients
Barash Clinical Anesthesia, 9e, p. 4525-4526 | Miller's Anesthesia, 10e, p. 6748-6749
TEG vs Conventional Tests: Evidence Summary
- Cardiac surgery with CPB: Strongest evidence - TEG/ROTEM-guided algorithms reduce blood product transfusion (Level I evidence, multiple RCTs)
- Liver transplantation: RCT evidence shows significantly lower blood component use vs INR/platelet-guided transfusion (Maiwall et al., Hepatology 2020)
- Trauma: Two large RCTs showed adding viscoelastography to routine coagulation studies did not improve overall outcomes after major trauma; however rTEG is still useful in massive transfusion protocols
- PPH: TEG-guided management led to only small reduction in blood loss vs conventional tests (RCT)
Goldman-Cecil Medicine, 2024 | Miller's Anesthesia, 10e
Comparison with Sonoclot
The Sonoclot analyzer is another VHA that measures the rate of fibrin polymerization using an ultrasonic probe. It is less commonly used but provides similar parameters. It is particularly useful in cardiac surgery for protamine monitoring.
Summary Table: TEG Parameters at a Glance
| Parameter | TEG | ROTEM | Reflects | Abnormal if |
|---|---|---|---|---|
| R / CT | R (min) | CT (sec) | Clotting factor activity (thrombin generation) | Prolonged → Factor deficiency, heparin |
| K / CFT | K (min) | CFT (sec) | Fibrin polymerization rate | Prolonged → Low fibrinogen |
| α-angle | α° | α° | Speed of clot propagation | Reduced → Low fibrinogen/thrombocytopenia |
| MA / MCF | MA (mm) | MCF (mm) | Clot strength (platelets 80% + fibrinogen 20%) | Low → Thrombocytopenia/platelet dysfunction/low fibrinogen; High → Hypercoagulable |
| LY30 / LI30 | LY30 (%) | LI30 (%) | Fibrinolysis at 30 min | Elevated → Hyperfibrinolysis |
Key Points for Examination
- TEG was first described by Hartert (1948) - a viscoelastic hemostatic assay, not just a coagulation test.
- It measures global hemostasis - primary + secondary hemostasis + fibrinolysis in whole blood.
- The key difference: TEG uses a rotating cuvette; ROTEM uses a rotating pin - both measure clot viscoelasticity.
- R value (reaction time) - reflects coagulation factors/thrombin; prolonged by heparin, factor deficiency.
- MA (maximum amplitude) - reflects clot strength; primarily reflects platelet function and number (80%) + fibrinogen (20%).
- LY30 - detects fibrinolysis; most important in liver transplantation and trauma.
- FIBTEM channel (ROTEM) - isolates fibrinogen contribution from platelet contribution to clot strength.
- HEPTEM channel (ROTEM) - distinguishes heparin effect from intrinsic factor deficiency.
- Most robust clinical evidence for TEG use is in cardiac surgery (reduces blood product use).
- TEG cannot detect primary hemostasis defects (VWD, platelet adhesion), warfarin reliably, or the effect of hypothermia (sample is heated).
References:
- Miller's Anesthesia, 10th Edition - Viscoelastic Measures of Coagulation, p. 6747-6749
- Barash, Cullen and Stoelting's Clinical Anesthesia, 9th Edition - Viscoelastic Testing, p. 1278; Table 53-3, Figures 53-1, 53-2
- Goldman-Cecil Medicine, International Edition - Thromboelastography section
- de Oliveira et al. [Systematic Review & Meta-Analysis, 2025] - Viscoelastic tests and blood products in liver transplantation [PMID: 40288081]
This is a shared conversation. Sign in to Orris to start your own chat.