How nephritic Syndrome csuses hyperkalemia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-grounded explanation of how nephritic syndrome causes hyperkalemia.
How Nephritic Syndrome Causes Hyperkalemia
Nephritic syndrome causes hyperkalemia through two tightly linked mechanisms - reduced tubular flow (oliguria) and hyporeninemic hypoaldosteronism. These are not separate diseases; they are direct consequences of the glomerular inflammation that defines the syndrome.
1. The Core Pathophysiology of Nephritic Syndrome
Nephritic syndrome is characterized by:
- Hematuria (RBC casts)
- Oliguria with azotemia (reduced GFR)
- Proteinuria
- Hypertension
The key driver is inflammatory glomerular injury - proliferative lesions, leukocyte infiltration, and often crescent formation - which directly reduces the number of functioning nephrons and drops GFR sharply. (Robbins & Cotran Pathologic Basis of Disease)
2. Mechanism 1 - Oliguria and Reduced Tubular Flow Rate
Potassium excretion by the kidney is flow-dependent. In the aldosterone-sensitive distal convoluted tubule and collecting duct, K+ secretion into the tubular lumen requires:
- Adequate distal Na+ delivery (which creates the electrochemical gradient)
- Adequate tubular fluid flow rate to "wash away" secreted K+ and maintain the concentration gradient
When GFR drops sharply (as it does in acute nephritic syndrome/acute glomerulonephritis), both distal Na+ delivery and tubular flow rate fall dramatically. The result:
- Less K+ is secreted into the tubule
- Less K+ is excreted in urine
- Plasma K+ rises
"Potassium excretion by the kidney is flow dependent; therefore, oliguria and anuria are important causes of hyperkalemia." - Textbook of Family Medicine 9e
"Hyperkalemia is more common in oliguric acute kidney injury; distal tubular flow rate and Na+ delivery are less limiting factors in non-oliguric patients." - Harrison's Principles of Internal Medicine 22E
Harrison's specifically lists Acute GN (glomerulonephritis/nephritic syndrome) as a cause of hyperkalemia via hyporeninemic hypoaldosteronism with a low TTKG (transtubular K+ gradient) in its diagnostic algorithm (see below).
3. Mechanism 2 - Hyporeninemic Hypoaldosteronism
In acute nephritic syndrome (particularly post-infectious GN, IgA nephropathy, and lupus nephritis), the inflamed and compressed glomerular apparatus can suppress renin release from the juxtaglomerular cells. This leads to:
Low renin → Low angiotensin II → Low aldosterone
Aldosterone normally acts on principal cells of the collecting duct to:
- Upregulate ENaC (apical Na+ channel) → increases lumen-negative potential
- Upregulate ROMK (apical K+ channel) → drives K+ secretion into the lumen
Without adequate aldosterone, this entire secretory machinery is downregulated, and K+ accumulates in the blood.
"Persistent hyperkalemia is usually caused by decreased potassium excretion... Because aldosterone deficiency is an important cause of decreased potassium excretion, hyperkalemia is seen with hyperreninism, hypoaldosteronism, type 4 RTA, and drugs that inhibit aldosterone." - Textbook of Family Medicine 9e
Harrison's diagnostic flowchart (below) explicitly places Acute GN under the "low renin, low aldosterone" branch as a cause of hyperkalemia.
4. Mechanism 3 - Metabolic Acidosis (Compounding Effect)
Nephritic syndrome with reduced GFR also causes metabolic acidosis (retention of H+ and inability to excrete acid load). Acidosis independently worsens hyperkalemia:
- Extracellular acidosis drives H+ into cells
- To maintain electroneutrality, K+ exits cells into the extracellular fluid (K+/H+ exchange)
- This transcellular shift raises serum K+
Conversely, hyperkalemia itself impairs renal NH4+ excretion (K+ competes with NH4+ for reabsorption at the thick ascending limb), creating a vicious cycle. (Harrison's 22E)
Summary Table
| Mechanism | Pathway | Effect |
|---|---|---|
| Reduced GFR / oliguria | Low distal Na+ delivery + low tubular flow | Less K+ secreted and excreted |
| Hyporeninemic hypoaldosteronism | Inflamed JG apparatus → low renin → low aldosterone | ENaC/ROMK downregulated; K+ retained |
| Metabolic acidosis | H+/K+ shift out of cells | Adds to plasma K+ load |
Diagnostic Algorithm (Harrison's 22E)
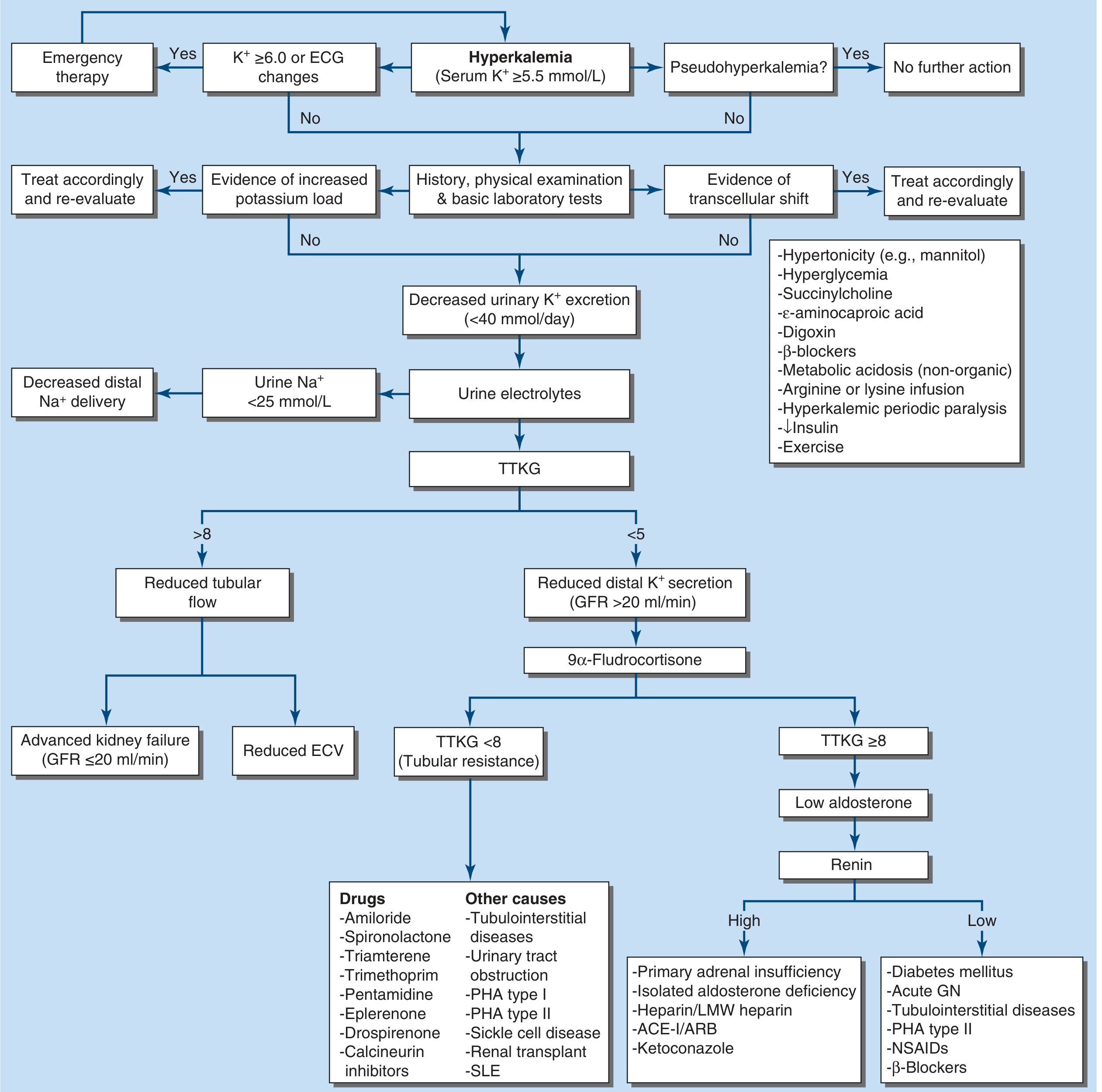
Note "Acute GN" listed in the bottom right under low renin, low aldosterone - exactly as described above.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 56 - Disorders of Potassium Balance
- Robbins & Cotran Pathologic Basis of Disease - Nephritic Syndrome
- Textbook of Family Medicine 9e - Potassium section
- National Kidney Foundation Primer on Kidney Diseases 8e - Physiologic Regulation of Kidney Potassium Excretion

IMG_4297.jpg
read this ecg
analyse_media
ECG Interpretation
Machine Parameters (GE MAC2000):
- Paper speed: 25 mm/s | Gain: 10 mm/mV | Filter: 0.56-20 Hz, 50 Hz notch
- Recorded axis - P/QRS/T: 57 / 42 / 107 degrees
- Format: 4x2.5x3 with rhythm strip
Systematic Analysis
| Parameter | Finding |
|---|---|
| Rate | ~85 bpm |
| Rhythm | Regular sinus rhythm |
| P axis | 57° (normal) |
| QRS axis | 42° (normal) |
| T axis | 107° (borderline) |
P Waves: Normal morphology and duration (<120 ms). Upright in I, II, aVF; inverted in aVR - consistent with normal sinus origin. No signs of atrial enlargement.
PR Interval: ~140 ms - normal, constant. No AV block.
QRS Duration: ~80 ms - narrow, normal. No bundle branch block.
QRS Morphology:
- Normal R-wave progression across precordials
- Transition between V3-V4 (normal)
- No voltage criteria for LVH (Sokolow-Lyon not met)
- No RVH pattern
ST Segments: Isoelectric in all leads. No elevation or depression.
T Waves: Upright in I, II, aVL, aVF, V3-V6. Inverted in aVR (normal). No hyperacute, flattened, or deeply inverted T waves.
Q Waves: No pathological Q waves.
QTc: Visually normal (QT < half the preceding R-R interval).
Impression
Normal ECG - Normal sinus rhythm at ~85 bpm with normal axis, intervals, and morphology. No evidence of ischemia, infarction, hypertrophy, or arrhythmia.
The machine label reads "Unconfirmed" - which simply means it has not been reviewed/signed off by a physician yet, not that there is an abnormality.
One minor note: the T axis of 107° is slightly rightward relative to the QRS axis (42°), giving a QRS-T angle of ~65°. This is within the upper limit of normal but worth noting if there is clinical suspicion of right heart strain or metabolic disturbance.
This is a shared conversation. Sign in to Orris to start your own chat.