Explain me comman 10 heart disease with ecg changes with images various type of myocardial infraction
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common heart diseases ECG changes types myocardial infarction ECG patterns 2024
Finding Sources
Finding Sources
Searching the Web
STEMI NSTEMI inferior anterior lateral posterior ECG pattern images diagram
Reading File
Reading File
Searching the Web
ECG atrial fibrillation heart block ventricular tachycardia pericarditis hypertrophic cardiomyopathy images
Finding Sources
Reading Web Page
https://ecg.utah.edu/lesson/9
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Searching the Web
ECG pericarditis diffuse ST elevation PR depression heart failure LVH Wolff Parkinson White site:litfl.com OR site:ecgwaves.com
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Searching the Web
ECG atrial fibrillation example complete heart block third degree ventricular tachycardia strip image
Loading Image
Here is a thorough guide to 10 common heart diseases with their ECG changes, followed by a detailed breakdown of all major types of myocardial infarction.
ECG Reference: Understanding the Waveform

The standard ECG records P (atrial depolarization), QRS (ventricular depolarization), and T (ventricular repolarization) waves. The ST segment sits between QRS and T - it is the most clinically important zone for detecting ischemia, infarction, and pericarditis.
10 Common Heart Diseases with ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia with full-thickness myocardial injury.
Key ECG Changes:
- ST elevation ≥1 mm in 2 or more contiguous leads (the hallmark finding)
- Hyperacute T waves (tall, broad, peaked T waves) - often the earliest change
- Pathological Q waves develop within hours to days (indicates necrosis)
- T wave inversion in the evolution phase
- Reciprocal ST depression in mirror-image leads (confirms STEMI diagnosis)
ECG Evolution over time:
- Minutes: Hyperacute tall T waves
- Hours: ST elevation, loss of R waves
- Hours-Days: Q wave formation, T wave inversion
- Weeks-Months: ST returns to baseline, T waves may normalize (Q waves persist permanently)
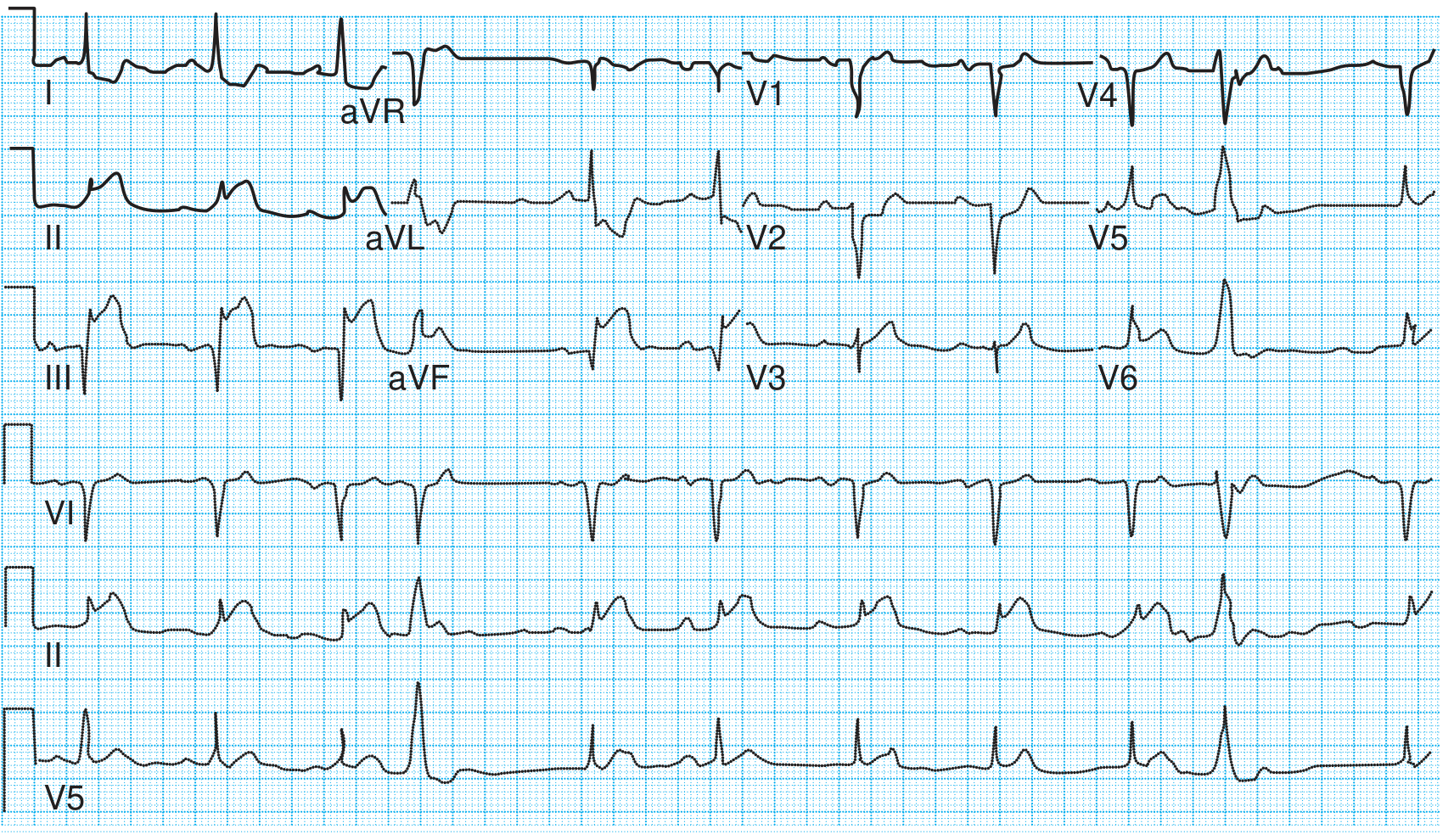
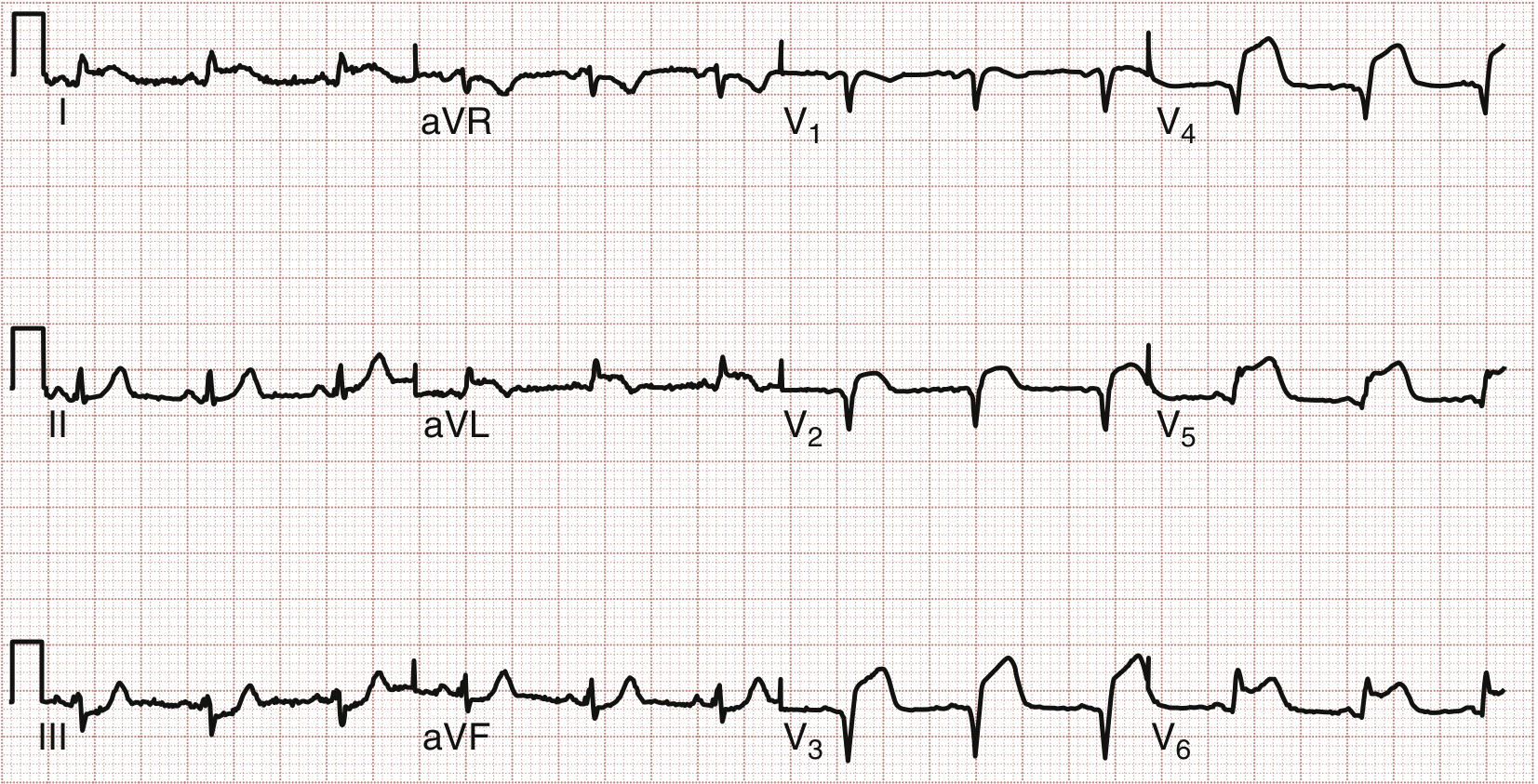
2. Inferior Myocardial Infarction
Artery involved: Right Coronary Artery (RCA) in 80-85%; Left Circumflex (LCx) in 15-20%
ECG Leads Affected: II, III, aVF
Key ECG Changes:
- ST elevation in leads II, III, aVF
- Reciprocal ST depression in leads I and aVL (highly specific - 90% sensitive for RCA occlusion when elevation is greater in III than II)
- ST elevation greater in III than II = RCA occlusion
- ST elevation greater in II than III = LCx occlusion
- ST elevation in V1 during inferior STEMI = right ventricular involvement
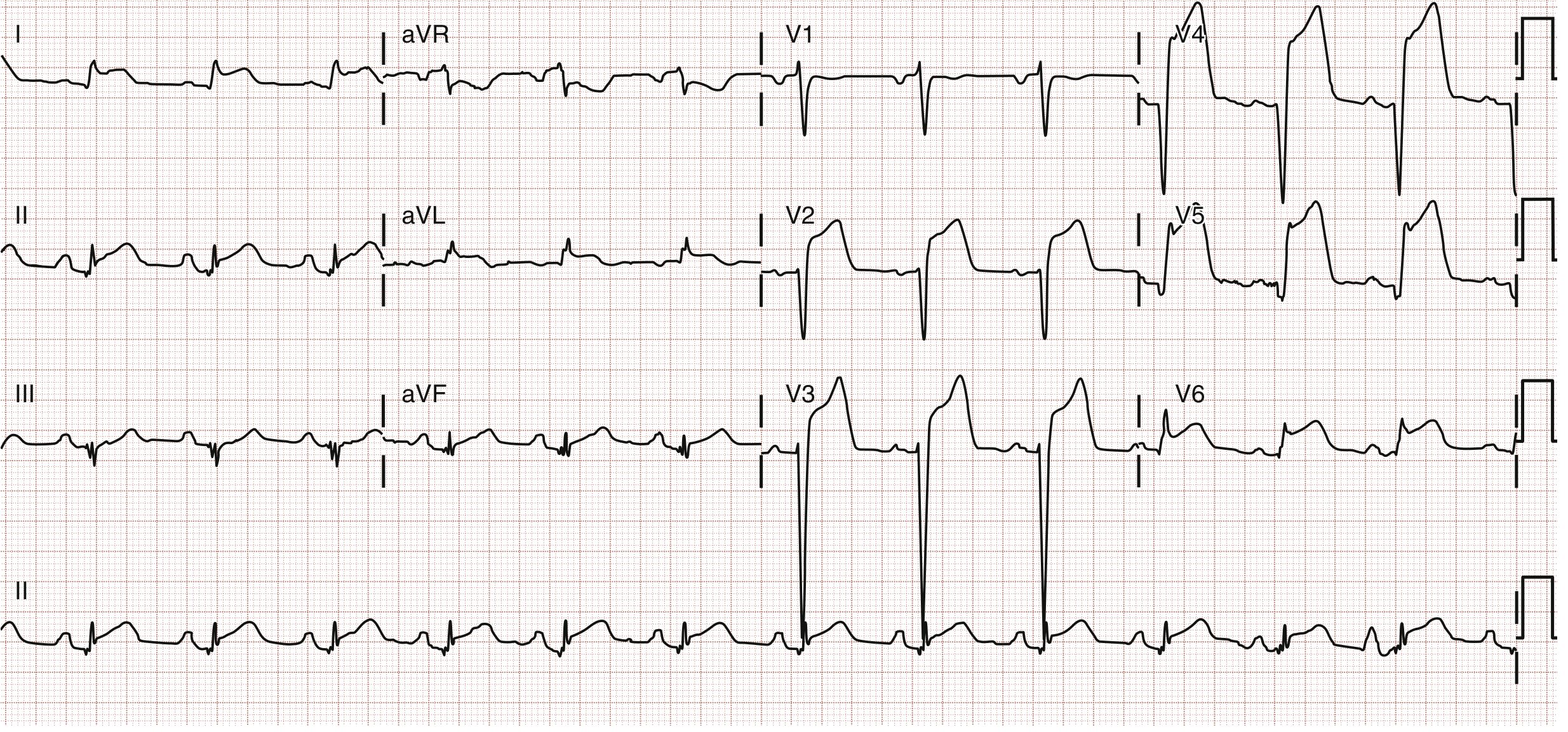
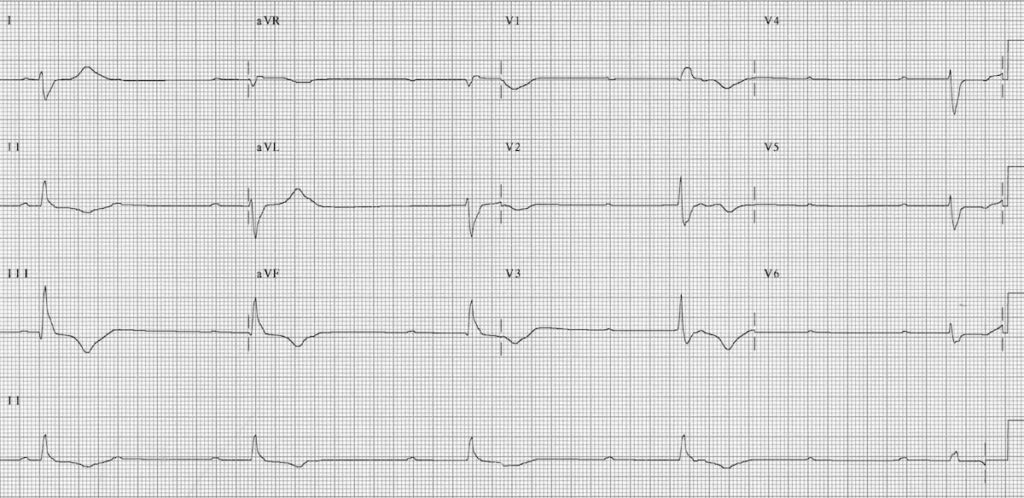
3. Anterior Myocardial Infarction
Artery involved: Left Anterior Descending (LAD)
ECG Leads Affected: V1-V4 (and V5-V6 if anterolateral)
Key ECG Changes:
- ST elevation in V1-V4
- QS or pathological Q waves in V1-V3 (anteroseptal subtype)
- R wave regression (loss of normal R wave progression)
- Reciprocal ST depression may be absent (unlike inferior MI)
- Wellens Syndrome - biphasic or deeply inverted T waves in V2-V3 indicating critical proximal LAD stenosis (pre-infarction pattern)
- de Winter Pattern - J-point depression with upsloping ST depression in precordial leads + ST elevation in aVR = proximal LAD occlusion equivalent
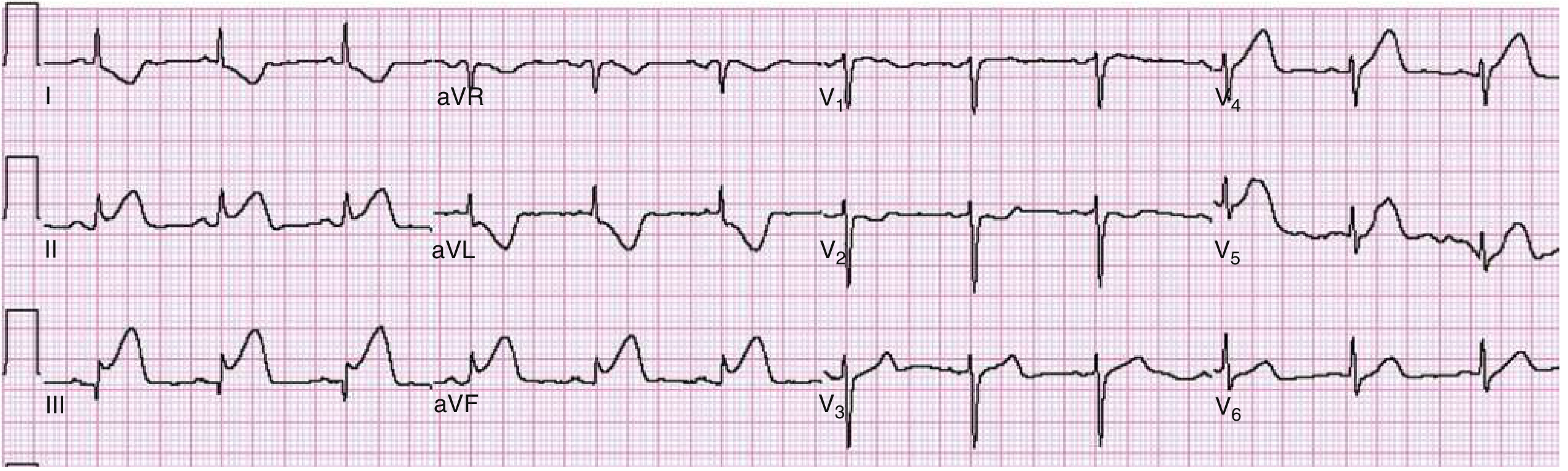
4. Lateral Myocardial Infarction
Artery involved: Left Circumflex (LCx) or first Diagonal branch of LAD
ECG Leads Affected: I, aVL (high lateral), V5-V6 (low lateral)
Key ECG Changes:
- ST elevation in I, aVL, V5, V6
- Reciprocal ST depression in III, aVF, and V1
- "High lateral" MI: changes only in I and aVL
- Isolated lateral STEMI can be subtle and missed
5. Anterolateral Myocardial Infarction
Artery involved: Proximal LAD (large territory)
ECG Leads Affected: V1-V6, I, aVL (combined anterior + lateral)
Key ECG Changes:
- Broad ST elevation spanning V1-V6 plus leads I and aVL
- Large infarct territory = worse prognosis
- More leads involved = larger infarct, higher mortality
6. Posterior Myocardial Infarction
Artery involved: RCA (posterior descending branch) or LCx
ECG Leads Affected: Reciprocal changes in V1-V3; direct changes in V7-V9 (posterior leads)
Key ECG Changes (V1-V3 - reciprocal/mirror image):
- ST depression (horizontal) in V1-V3 - the mirror image of posterior ST elevation
- Tall, broad R waves in V1-V2 (R/S ratio >1 in V1 = pathological, equivalent to Q wave in posterior infarction)
- Large upright T waves in V1-V3
- Posterior leads V7-V9: ST elevation ≥0.5 mm confirms diagnosis
Clinical tip: Posterior MI accompanies 15-20% of all STEMIs, usually with inferior or lateral MI. Isolated posterior MI (5-10% of infarcts) is frequently missed on standard 12-lead ECG.

7. Right Ventricular (RV) Infarction
Artery involved: Proximal RCA (before RV branches)
Setting: Almost always accompanies inferior STEMI
ECG Leads Affected: Right-sided leads (V3R, V4R)
Key ECG Changes:
- Inferior STEMI (II, III, aVF) PLUS
- ST elevation ≥1 mm in V4R (right-sided lead) = highly specific for RV infarction
- ST elevation in V1 during an inferior MI
- ST elevation greater in III than aVF
- Bradycardia/AV block common (RCA supplies AV node)
Clinical significance: RV infarction causes haemodynamic collapse with hypotension, elevated JVP, and clear lung fields. Must avoid nitrates (will worsen hypotension).
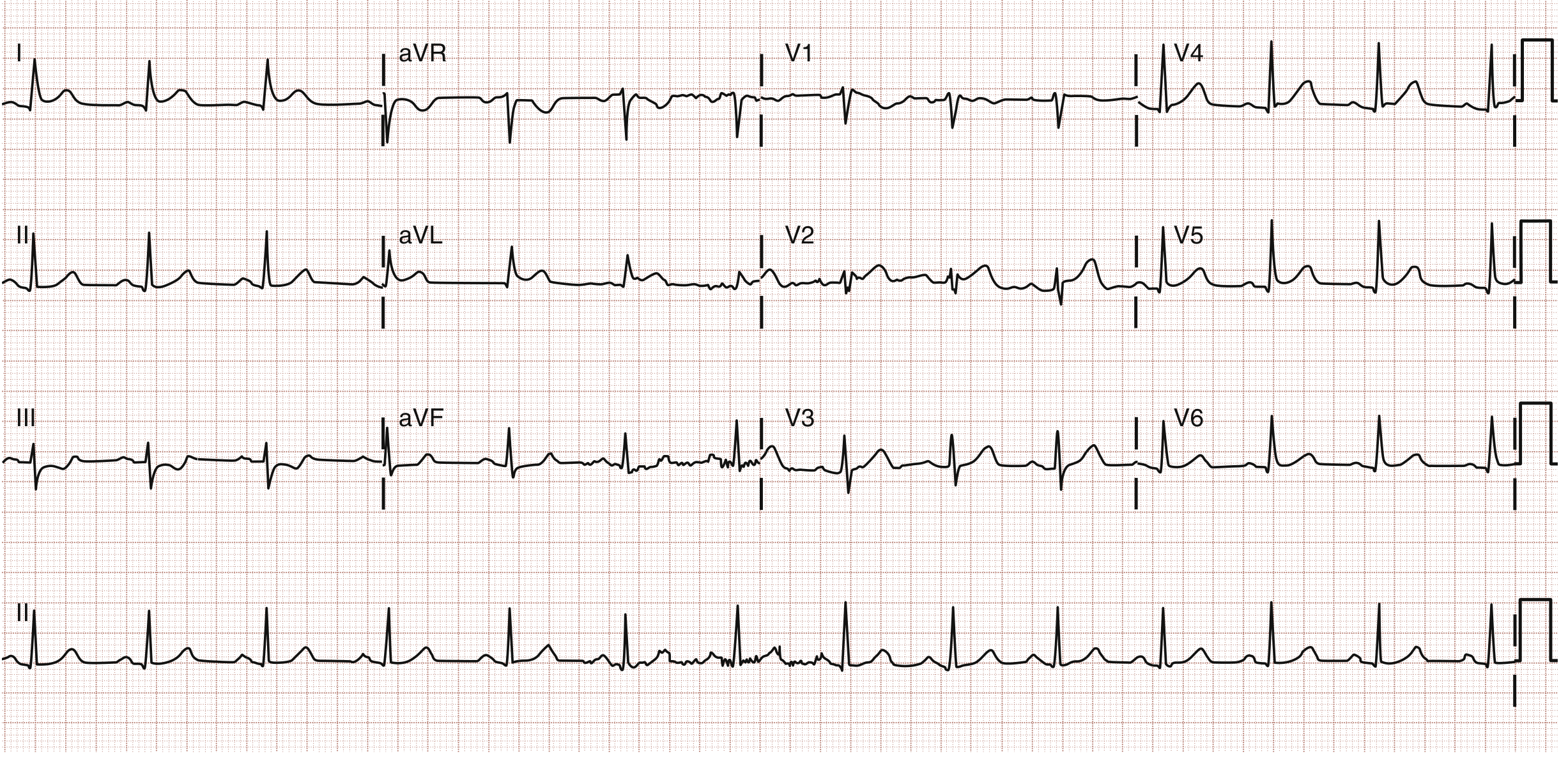
8. Atrial Fibrillation (AF)
Pathophysiology: Chaotic atrial electrical activity - multiple reentrant wavelets firing at 350-600 bpm, causing disorganized atrial contraction and irregular ventricular response.
Key ECG Changes:
- Absent P waves - replaced by irregular fibrillatory baseline (fine or coarse undulations, especially visible in V1)
- Irregularly irregular RR intervals (no fixed pattern between beats) - the signature finding
- Narrow QRS (unless aberrant conduction or pre-existing bundle branch block)
- Rate: ventricular rate 100-180 bpm in uncontrolled AF; slower with rate control or AV nodal disease
- No organized atrial activity
Key distinction: AF with complete heart block shows absent P waves but REGULAR ventricular rhythm (escape rhythm takes over).
Sources: Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; Guyton & Hall Physiology
9. Complete (Third-Degree) Heart Block
Pathophysiology: Complete failure of AV conduction - atrial and ventricular activity are completely dissociated.
Key ECG Changes:
- P waves and QRS complexes fire independently at different rates
- Atrial rate (P waves) > Ventricular rate (QRS complexes)
- No fixed PR interval - PR interval varies beat to beat (AV dissociation)
- Wide QRS if escape rhythm originates below the bundle of His (ventricular escape, 20-40 bpm)
- Narrow QRS if escape rhythm is junctional (AV nodal escape, 40-60 bpm)
- Ventricular rate is slow (bradycardia, often 30-50 bpm)
10. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes diffuse epicardial irritation affecting all leads simultaneously.
Key ECG Changes (4 stages):
| Stage | Timing | Changes |
|---|---|---|
| Stage 1 | Hours to days | Diffuse concave ("saddle-shaped") ST elevation in most leads (except aVR and V1); PR depression in same leads; PR elevation in aVR |
| Stage 2 | Days | ST returns to baseline; PR depression resolves |
| Stage 3 | Weeks | Diffuse T wave inversion |
| Stage 4 | Weeks-months | ECG normalizes |
Key differentiating features from STEMI:
- ST elevation is diffuse (multiple non-contiguous territories) vs. regional in STEMI
- ST morphology is concave upward (saddle-shape) vs. convex (tombstone) in STEMI
- PR depression is unique to pericarditis
- No reciprocal ST depression (except in aVR/V1 - normal in pericarditis)
- No Q waves develop
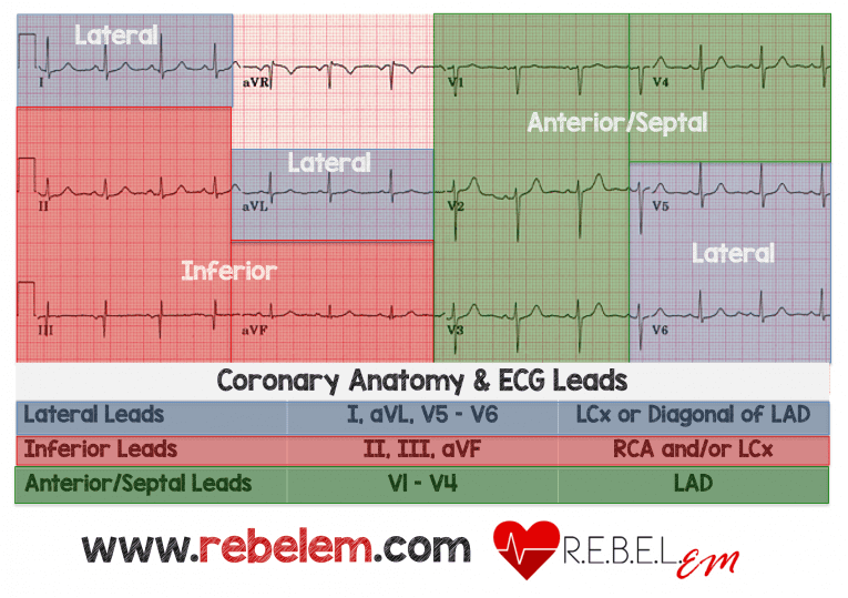
ECG Lead Localization Summary
Quick Reference: All MI Types at a Glance
| MI Type | Leads with ST Elevation | Artery | Reciprocal Changes |
|---|---|---|---|
| Anteroseptal | V1-V3 | LAD (septal) | None typical |
| Anterior | V2-V4 | LAD | None typical |
| Anterolateral | V1-V6, I, aVL | Proximal LAD | None typical |
| High Lateral | I, aVL | LCx/D1 | III, aVF, V1 |
| Low Lateral | V5-V6 | LCx | None typical |
| Inferior | II, III, aVF | RCA (80%) / LCx (20%) | I, aVL |
| Posterior | V7-V9 (direct); ST depression V1-V3 (reciprocal) | RCA/LCx | Tall R, ST depression V1-V3 |
| Right Ventricular | V4R (right-sided leads) | Proximal RCA | Accompanies inferior STEMI |
| Left Main / Multi-vessel | ST elevation aVR + widespread ST depression | LMCA / LAD | Widespread depression in I, II, V4-V6 |
Additional Conditions (Bonus)
Left Ventricular Hypertrophy (LVH)
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- ST depression and T wave inversion in lateral leads (V5-V6, I, aVL) = "strain pattern"
- Left axis deviation
- Broad, notched P wave (P mitrale) indicating left atrial enlargement
- Sources: Harrison's 22e; Tintinalli's Emergency Medicine
Hypertrophic Cardiomyopathy (HCM)
- LVH voltage criteria
- Deep, narrow septal Q waves in lateral leads (I, aVL, V5-V6) - due to septal hypertrophy
- ST depression and T wave inversions
- Markedly abnormal ECG in ~95% of symptomatic patients
- Associated with atrial fibrillation, ventricular tachycardia, and sudden cardiac death
Wolff-Parkinson-White (WPW) Syndrome
- Short PR interval (<120 ms)
- Delta wave - slurred initial upstroke of the QRS complex (pre-excitation via accessory pathway)
- Wide QRS complex
- Secondary ST-T changes (discordant to delta wave direction)
- Risk of very rapid AF conducting down the accessory pathway (dangerous)
Key ECG Patterns to Memorize
| Finding | Think of |
|---|---|
| Diffuse saddle-shaped ST elevation + PR depression | Acute pericarditis |
| Regional ST elevation with reciprocal depression | STEMI |
| ST depression V1-V3 + tall R wave in V1 | Posterior MI |
| ST elevation II, III, aVF + V4R | Inferior MI + RV infarction |
| Absent P waves + irregularly irregular QRS | Atrial fibrillation |
| P-QRS dissociation + slow wide QRS | Complete heart block |
| Short PR + delta wave + wide QRS | WPW |
| Giant R waves in precordial leads + strain pattern | LVH |
| ST elevation aVR + widespread ST depression | Left main / proximal LAD / multi-vessel |
Sources:
- Rosen's Emergency Medicine (Rosen's EM), Electrocardiographic Differential Diagnosis
- Tintinalli's Emergency Medicine, Electrocardiography chapter
- Harrison's Principles of Internal Medicine 22e (2025)
- Goldman-Cecil Medicine
- LITFL ECG Library (litfl.com)
- ECG Utah Learning Center (ecg.utah.edu)
This is a shared conversation. Sign in to Orris to start your own chat.