Schimitar syndrome full details for md exams 10 marks answer from fishman only
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the key content from Fishman's. Let me compile the full 10-mark answer.
Scimitar Syndrome (Pulmonary Venolobar Syndrome)
Source: Fishman's Pulmonary Diseases and Disorders, Chapter 105
1. Definition and Nomenclature
Scimitar syndrome, also termed pulmonary venolobar syndrome, is a rare congenital disorder of the lung and pulmonary vasculature characterized by partial or total anomalous pulmonary venous return of the right lung (most commonly the right lower lobe) to the inferior vena cava (IVC).
The name derives from the appearance of the anomalous pulmonary vein on chest radiograph: a curvilinear shadow along the right heart border that resembles the curve of a Persian scimitar sword.
2. Epidemiology
- Prevalence: 1 to 3 cases per 100,000 live births
- Female predominance (male:female ratio of 1:2)
- Represents only 5% of all partial anomalous pulmonary venous return (PAPVR) abnormalities
3. Embryology and Pathogenesis
During early embryogenesis, pulmonary venous blood drains into the splanchnic venous circulation. As cardiac structures develop, drainage transitions to the left atrium, with regression of the systemic connection. Initially both lungs drain via a common pulmonary vein, which later divides into four separate ostia in the left atrium.
A defect during this transition from splanchnic to cardiac drainage leads to total or partial anomalous pulmonary venous return of the right lung - the fundamental defect in scimitar syndrome.
4. Associated Anomalies
Scimitar syndrome is frequently associated with:
- Right pulmonary hypoplasia (small right lung)
- Systemic arterial blood supply of the right lung (aortopulmonary collaterals)
- Congenital heart disease (most commonly a secundum ASD)
- Dextrocardia or mesocardia (cardiac shift to the right due to lung hypoplasia)
- Horseshoe lung (rare variant)
5. Clinical Presentation
Infantile Form (Severe):
When pulmonary-to-systemic shunting is severe, patients present in infancy or early childhood with:
- Tachypnea
- Pulmonary hypertension
- Evidence of right heart failure
Adult Form (Mild):
With lesser degrees of shunting, patients may be asymptomatic or present in early adulthood with:
- Recurrent pneumonia (31%)
- Dyspnea on exertion (19%)
- Hemoptysis (6%)
6. Diagnostic Investigations
Chest Radiograph
The classic finding is a curvilinear tubular opacity in the right lower hemithorax coursing from the right hilum toward the IVC, with:
- Right lung hypoplasia
- Ipsilateral mediastinal shift to the right
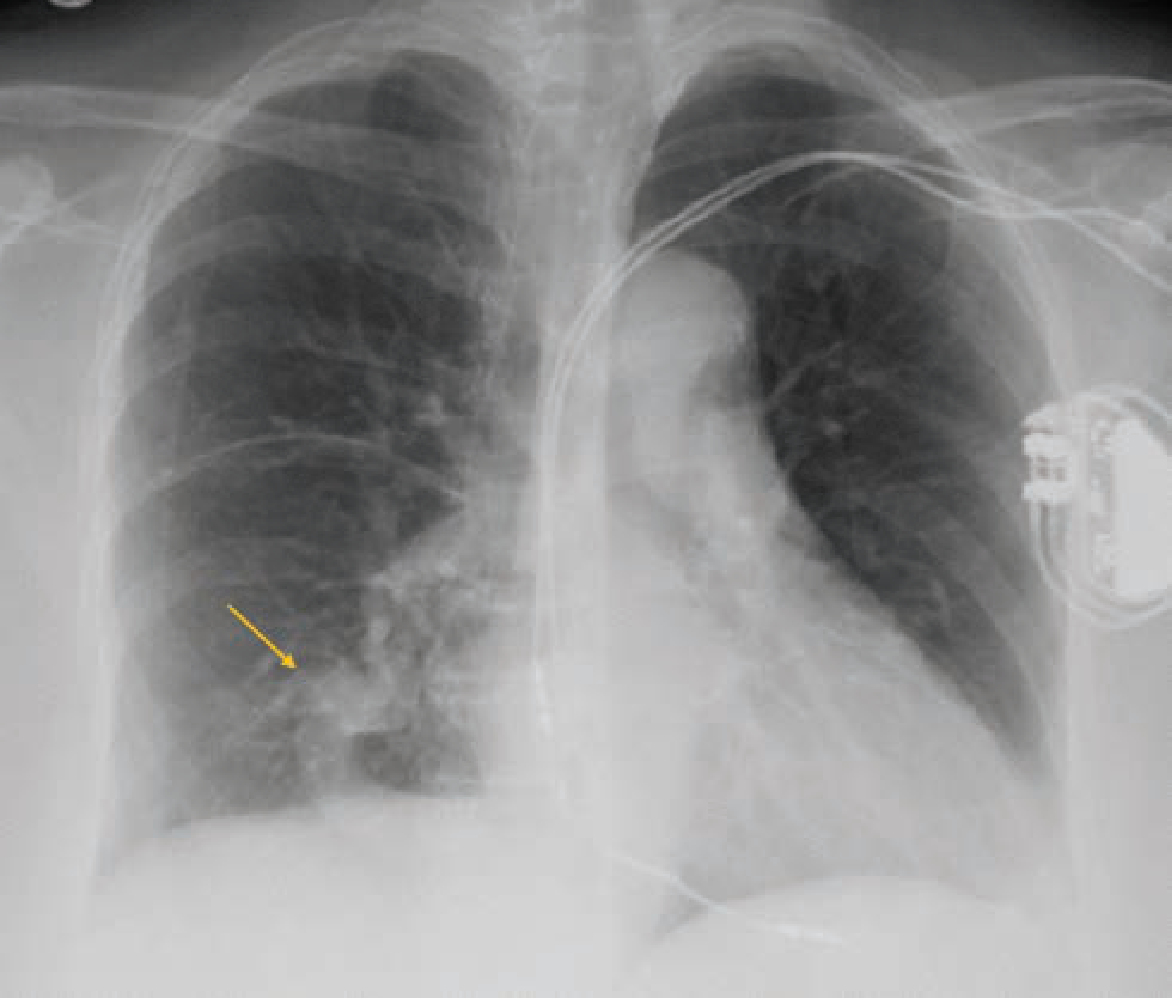
Fig. 105-19 (Fishman's): Chest radiograph reveals a curvilinear tubular opacity in the right lower hemithorax (arrow) that courses from the right hilum toward the IVC.
Two-Dimensional Transthoracic Echocardiography (TTE)
- Used to assess right ventricular function and estimate pulmonary artery pressure
- In the suprasternal short-axis view with color Doppler: the left pulmonary vein can be seen entering the left atrium, but the right pulmonary vein cannot be identified entering the left atrium
- Parasternal short-axis view may show a small right main pulmonary artery compared to the normal-sized left PA
- Findings can be confirmed on transesophageal echocardiogram (TEE)
CT Chest (Contrast-Enhanced)
The scimitar vein is clearly delineated on CECT as the anomalous vessel draining into the IVC:
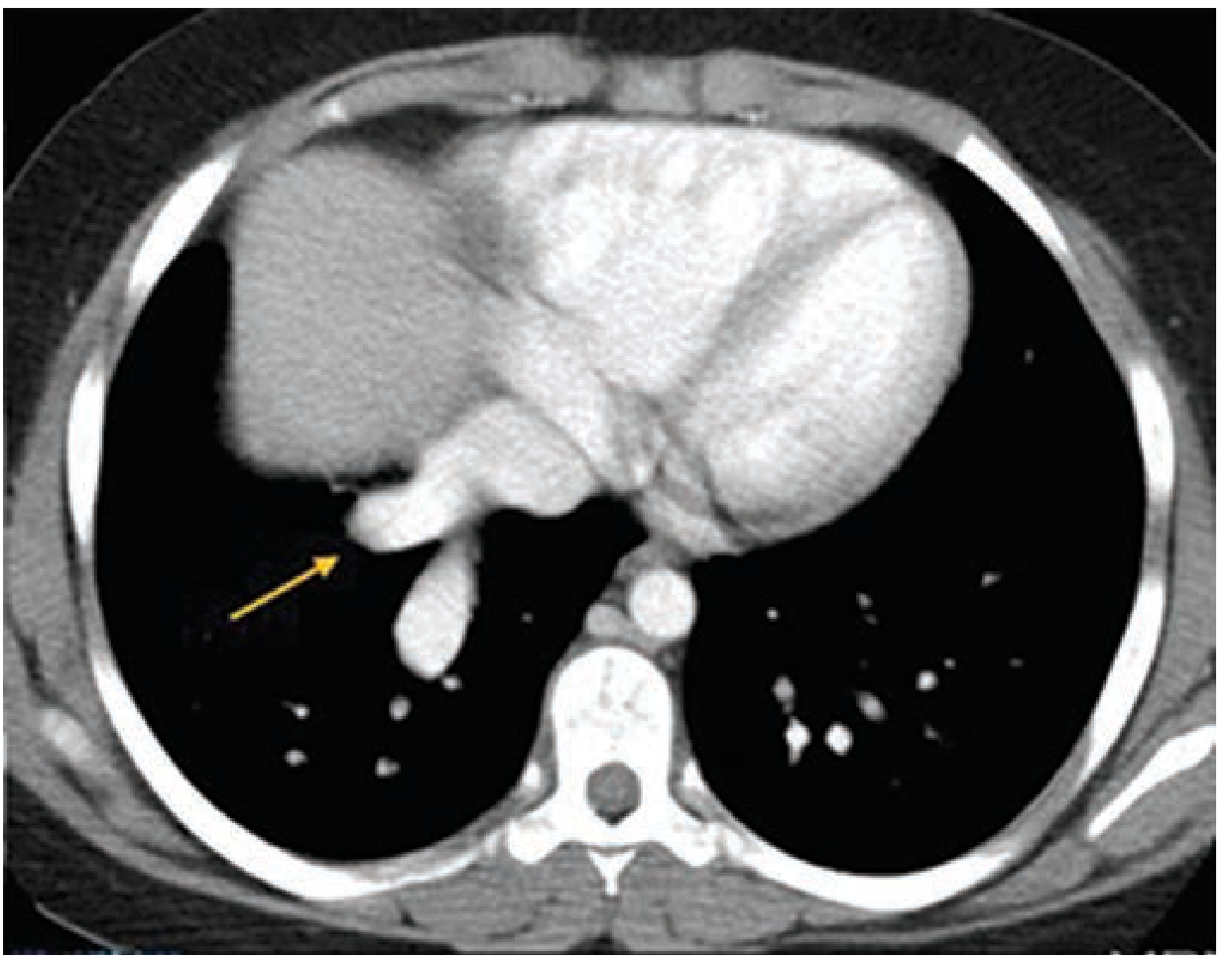
Fig. 105-20 (Fishman's): Contrast-enhanced CT chest axial image revealing the anomalous scimitar vein (arrow) draining into the IVC, with right lung hypoplasia.
Lung Scintigraphy
- Technetium-99m labeled macroaggregated albumin (MAA) scintigraphy can quantify the shunt fraction - an important factor in management decisions
Cardiac Catheterization / MR Angiography
- Used for definitive delineation of the anomalous vein, assessment of pulmonary artery pressures, and identification of systemic arterial collaterals
7. Pathophysiology of Hemodynamic Compromise
The anomalous pulmonary vein draining into the IVC creates a left-to-right shunt. The degree of shunting determines clinical severity:
- Large shunt → right ventricular volume overload → pulmonary hypertension → right heart failure
- Small shunt → may remain asymptomatic for decades
- The left-to-right shunt fraction tends to decrease with age in most patients
8. Management
Management depends on the severity of pulmonary-to-systemic shunting and its hemodynamic impact.
Conservative Management:
- For small shunt fractions with minimal symptoms: conservative management with follow-up echocardiography is recommended
- Life expectancy is normal with small shunts
Surgical Intervention:
Indicated primarily for:
- Large shunt with right ventricular volume overload
- Pulmonary hypertension
Two surgical techniques:
- Traditional approach: Direct anastomosis of the anomalous pulmonary vein to the left atrium - associated with frequent thrombosis or stenosis at the anastomotic site
- Novel technique: Anastomosis of the anomalous pulmonary vein to a Gore-Tex vascular graft placed through the right atrial wall, sutured into a surgically created atrial septal defect to direct blood flow into the left atrium (avoids the high anastomotic failure rate of the direct approach)
9. Prognosis
- Patients with small shunts and no pulmonary hypertension have normal life expectancy
- Surgical outcomes in infantile-type disease (with pulmonary hypertension) are significantly worse
- The left-to-right shunt fraction decreasing with age is a favorable prognostic feature
Summary Table for Quick Revision
| Feature | Detail |
|---|---|
| Other name | Pulmonary venolobar syndrome |
| Core defect | Partial/total APVR of right lung to IVC |
| Prevalence | 1-3 per 100,000; F > M (1:2) |
| % of all PAPVR | 5% |
| Embryological basis | Failed transition from splanchnic to cardiac venous drainage |
| CXR finding | Curvilinear opacity right heart border (scimitar sign) + right lung hypoplasia |
| Common associations | Right pulmonary hypoplasia, ASD, systemic arterial supply to right lung |
| Infantile presentation | Tachypnea, pulmonary HTN, right heart failure |
| Adult presentation | Recurrent pneumonia, dyspnea, hemoptysis (or asymptomatic) |
| Best imaging | CECT chest / MR angiography |
| Shunt quantification | Tc-99m MAA scintigraphy |
| Surgical technique | Gore-Tex graft via right atrium to surgically created ASD (preferred over direct anastomosis) |
All content sourced from: Fishman's Pulmonary Diseases and Disorders (2-Volume Set), Chapter 105 - Vascular Disorders / Scimitar Syndrome (Pulmonary Venolobar Syndrome), pp. 1867-1869
This is a shared conversation. Sign in to Orris to start your own chat.