Answer the question and explain
Reading File
Running Command
cd /home/daytona/workspace/attachments/48a8d5ad-24a4-45db-9a5b-e8fef318fce5/ && …
Running Command
cd /home/daytona/workspace/attachments/48a8d5ad-24a4-45db-9a5b-e8fef318fce5/ && …
Running Command
cd /home/daytona/workspace/attachments/48a8d5ad-24a4-45db-9a5b-e8fef318fce5/ && …
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Above is a complete answer guide for all major questions in your BPT/BOT Paper XII - General Surgery past year papers (2015-2025). Here is a quick summary of what was covered:
What Was Answered (Summary)
The PDF contains 10 years of question papers (2015-2025). Every question has been answered with exam-ready explanations. Topics covered:
Section A - Trauma & Emergency Surgery
- Shock - Definition, classification (5 types), ATLS Classes I-IV, full management of hemorrhagic shock
- Burns - Classification by depth, Wallace Rule of Nines, Parkland formula, airway management, surgical management
- Tension Pneumothorax - Pathophysiology, clinical features, immediate needle decompression
- Flail Chest - Paradoxical movement, management with analgesia + ventilation
- Primary & Secondary Survey (ATLS ABCDE)
- Damage Control Resuscitation - Permissive hypotension, 1:1:1 blood products, tranexamic acid
Section B - Wound & Soft Tissue
- Wound Healing - 4 phases, factors affecting healing (local + systemic)
- Chronic Ulcers - TIME framework, venous/arterial/diabetic/pressure ulcer management
- Surgical Site Infections - Classification, organisms, prevention, treatment
- Skin Grafts - SSG vs FTG comparison table, degloving injury
- Keloid vs Hypertrophic Scar
- Gas Gangrene - Clostridium, features, treatment (debridement + penicillin + HBO)
Section C - Elective Surgery
- Hernia - Classification, direct vs indirect inguinal hernia, Lichtenstein mesh repair
- Incisional Hernia - Risk factors, mesh repair
- Abdominal Incisions - 9 types with uses, criteria for ideal incision
- Uterine Prolapse - Degrees, features, pessary/surgical management (Manchester, vaginal hysterectomy)
- Laparoscopic vs Robotic Surgery - Pros and cons
Section D - ENT & Ophthalmology (included in this paper)
- Hearing Aids - 7 types (BTE, ITE, CIC, BAHA, Cochlear implant) with indications
- Conjunctivitis - Bacterial, viral, allergic, gonococcal, trachoma
- Refractive Errors - Myopia, hypermetropia, astigmatism, presbyopia
- Blindness - Causes and prevention (SAFE strategy for trachoma)
Section E - Miscellaneous
- Blood Transfusion Complications - Immediate + delayed + massive transfusion
- SIRS & Sepsis - Definitions, Sepsis-3, Surviving Sepsis bundle
- Anaesthesia - General, spinal, epidural, local with complications
- GCS - Full scoring table
- Intracranial Haemorrhages - Extradural (biconvex, lucid interval), subdural, SAH, intracerebral
- Urinary Incontinence - 5 types, conservative/medical/surgical management
- Haemolytic Disease of Newborn - Rh incompatibility, anti-D prophylaxis
- Pregnancy Signs by Trimester
Can you explain shock in detail
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Bailey & Love's Surgery 28th Ed, Sabiston, and Robbins Pathology. Here is the detailed explanation of shock:
SHOCK - Detailed Explanation
1. Definition
Shock is a systemic state of low tissue perfusion that is inadequate for normal cellular respiration. With insufficient delivery of oxygen and glucose, cells switch from aerobic to anaerobic metabolism. If perfusion is not restored in time, cell death ensues.
"A manifestation of the rude unhinging of the machinery of life" - Gross, 1872 (Sabiston Textbook of Surgery)
The modern definition acknowledges that shock is not merely about blood pressure - it involves failure of oxygen delivery, transport, and/or utilization at the cellular level.
2. Classification of Shock
(Bailey & Love's Surgery 28th Ed)
| Type | Primary Mechanism | Common Causes |
|---|---|---|
| Hypovolaemic | Reduced circulating volume | Haemorrhage, burns, vomiting, diarrhoea, third-spacing (pancreatitis, bowel obstruction) |
| Cardiogenic | Primary pump failure | Myocardial infarction, arrhythmias, valvular disease, cardiomyopathy, blunt myocardial injury |
| Obstructive | Mechanical obstruction to cardiac filling | Cardiac tamponade, tension pneumothorax, massive pulmonary embolism, air embolism |
| Distributive (Septic) | Peripheral vasodilation + maldistribution of blood flow | Sepsis, anaphylaxis, neurogenic (spinal cord injury) |
| Endocrine | Hormonal failure | Addisonian crisis, hypothyroid coma, hypoglycaemia |
Important point: These types can coexist. For example, a septic patient also has relative hypovolaemia. Hypovolaemia is the most common form and must always be excluded first in every shocked patient.
3. Pathophysiology of Shock
Shock operates at three levels simultaneously:
A. Cellular Level
When tissue perfusion falls, cells are deprived of oxygen and must switch from aerobic to anaerobic metabolism. The product is lactic acid (not CO2). Accumulation of lactic acid causes systemic metabolic acidosis.
As glucose within cells is exhausted:
- Anaerobic respiration ceases
- Sodium-potassium ATPase pumps fail - cells swell with sodium and water
- Intracellular lysosomes rupture and release autodigestive enzymes
- Cell lysis occurs - intracellular potassium floods the bloodstream, causing hyperkalaemia
- This cellular injury is reversible early but becomes irreversible with prolonged shock
B. Microvascular Level
As ischaemia progresses:
- Hypoxia and acidosis activate complement and prime leukocytes
- Generation of oxygen free radicals and cytokine release
- Injury to capillary endothelial cells - they become "leaky"
- Fluid escapes into tissues - tissue oedema forms, worsening cellular hypoxia
- Activation of the coagulation cascade can lead to DIC (Disseminated Intravascular Coagulation)
C. Systemic / Organ Level
The body mounts compensatory responses to maintain perfusion to vital organs:
Cardiovascular compensation:
- Reduced preload and afterload trigger baroreceptors
- Increased sympathetic activity → catecholamine release (adrenaline, noradrenaline)
- Results in: tachycardia, systemic vasoconstriction (except in septic/distributive shock where vasodilation occurs)
Renal compensation:
- Decreased renal perfusion → reduced glomerular filtration → oliguria
- Renin-angiotensin-aldosterone axis activated → further vasoconstriction + sodium/water retention
Endocrine compensation:
- Vasopressin (ADH) released → vasoconstriction + water reabsorption by collecting ducts
- Cortisol released from adrenal cortex → sensitises vessels to catecholamines, promotes sodium/water retention
- Respiratory compensation: Metabolic acidosis drives increased respiratory rate (tachypnoea) to blow off CO2 and produce compensatory respiratory alkalosis
4. ATLS Classification of Haemorrhagic Shock (Grades I-IV)
This is the most clinically used system for blood loss:
| Class | Blood Loss | % of Blood Volume | HR | BP | Pulse Pressure | RR | Urine Output | Mental Status |
|---|---|---|---|---|---|---|---|---|
| I | <750 mL | <15% | <100 | Normal | Normal/increased | 14-20 | >30 mL/hr | Normal, slightly anxious |
| II | 750-1500 mL | 15-30% | 100-120 | Normal | Decreased | 20-30 | 20-30 mL/hr | Mildly anxious |
| III | 1500-2000 mL | 30-40% | 120-140 | Decreased | Decreased | 30-40 | 5-15 mL/hr | Confused, drowsy |
| IV | >2000 mL | >40% | >140 | Very low | Very low | >35 | <5 mL/hr | Lethargic, unconscious |
Key insight: Blood pressure is often well maintained until 30-40% of blood volume is lost. Do not wait for hypotension to diagnose shock - tachycardia and peripheral vasoconstriction appear first.
5. Clinical Stages of Shock
Compensated (Mild) Shock
- Tachycardia, tachypnoea
- Mild reduction in urine output
- Mild anxiety
- Blood pressure maintained (normal), but pulse pressure narrows
- Cool, sweaty peripheries, prolonged capillary refill time
- The body is still fighting - perfusion to skin, muscle, and gut is sacrificed to protect heart and brain
Uncompensated - Moderate Shock
- Compensatory mechanisms begin to fail
- Urine output drops below 0.5 mL/kg/hour
- Blood pressure starts to fall (mild hypotension)
- Increasing tachycardia
- Patient becomes drowsy and confused
Uncompensated - Severe Shock
- Profound hypotension
- Maximal tachycardia, then bradycardia as a preterminal sign
- Patient is comatose or unresponsive
- Anuric (no urine output)
- Labouring respiration
- Peripheries no longer respond to vasopressors
- Death is imminent without intervention
(Clinical features table from Bailey & Love's Surgery 28th Ed, Table 2.2)
6. Specific Types - Additional Details
Hypovolaemic / Haemorrhagic Shock
Most common type in surgical practice. The body loses blood (or fluid), reducing preload, cardiac output, and tissue perfusion.
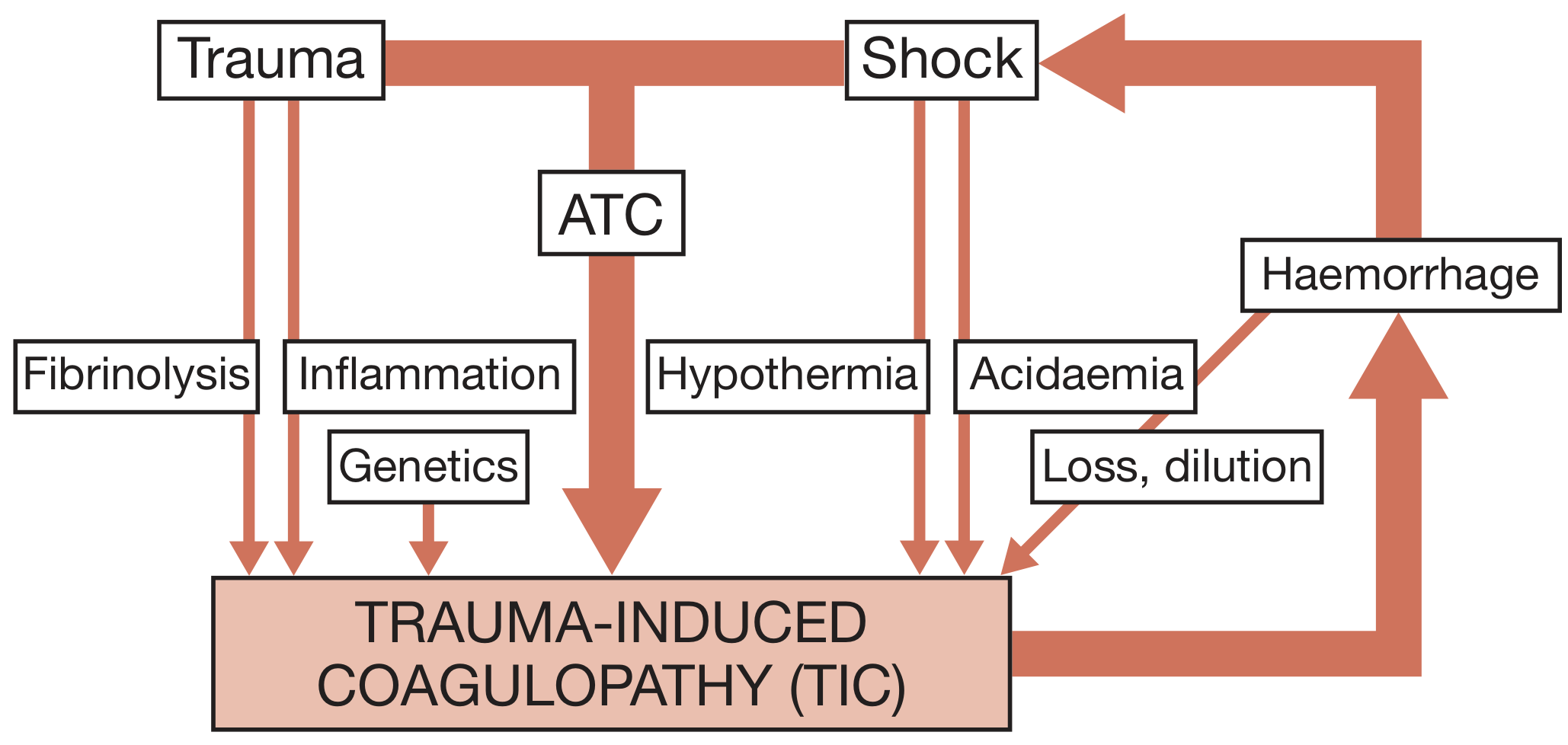
Triad of Death in trauma:
Hypothermia + Coagulopathy + Acidosis Each factor worsens the others in a deadly spiral: bleeding → acidosis and hypothermia → impaired coagulation → more bleeding.
Cardiogenic Shock
- Heart fails as a pump
- Evidence of venous hypertension (JVP raised, pulmonary oedema) alongside signs of low output
- NOT hypovolaemic - the problem is pump failure, NOT volume depletion
- Treating with aggressive fluids can worsen pulmonary oedema
Obstructive Shock
- Mechanical obstruction reduces cardiac filling (preload)
- Tension pneumothorax, tamponade: the heart is compressed externally
- Beck's triad of tamponade: Hypotension + raised JVP + muffled heart sounds
- Treatment is removing the obstruction (needle decompression, pericardiocentesis)
Distributive / Septic Shock
- Peripheral vasodilation causes blood to "pool" in the periphery
- Cardiac output is actually high (hyperdynamic circulation) but tissue extraction is impaired
- Features: warm peripheries, bounding pulse, widened pulse pressure (opposite to hypovolaemic shock)
- Pathogenesis: Microbial substances (endotoxin, LPS) → activate TLRs → massive cytokine release (TNF, IL-1, IL-6) → vasodilation + endothelial damage + coagulation activation → DIC + multi-organ failure
- Mortality: 20-40% despite treatment (Robbins Pathology)
Neurogenic Shock
- Loss of sympathetic vasomotor tone following spinal cord injury (above T6)
- Bradycardia + hypotension (in contrast, hypovolaemic shock causes tachycardia)
- Warm, dry skin (vasodilated, not vasoconstricted)
Anaphylactic Shock
- IgE-mediated hypersensitivity reaction → massive histamine release
- Vasodilation + increased vascular permeability
- Trigger: Bee sting, drug (penicillin, NSAID), food (peanut)
- Adrenaline (epinephrine) is the first-line treatment
7. Ischaemia-Reperfusion Injury and SIRS
When circulation is restored after a period of shock, a second wave of injury can occur:
- The acid and potassium load that built up during hypoperfusion floods the circulation
- Causes direct myocardial depression and further vasodilation
- Molecules from dead cells (DAMPs - Damage-Associated Molecular Patterns) activate leukocytes
- Complement, neutrophils, and microvascular thrombi cause injury to distant organs (lungs, kidneys, brain)
- Leads to: ARDS (Acute Respiratory Distress Syndrome), Acute Kidney Injury, cerebral oedema
- This is the basis of Multiple Organ Failure (MOF)
Multiple Organ Failure = 2 or more failed organ systems; carries 60% mortality. The only treatment is organ support - there is no specific therapy; prevention by early aggressive reversal of shock is the key.
8. Management of Shock
Universal Principles (All Types)
- Treat the cause (haemorrhage control, drain pus, fix the heart)
- Correct hypovolaemia first - give IV fluids before any vasopressor; giving vasopressors to an empty heart is dangerous and depletes myocardial oxygen rapidly
- Airway and O2 - high-flow oxygen, intubate if GCS <8 or airway at risk
- IV access - two large-bore (14-16G) peripheral cannulae; short, wide-bore cannulae allow rapid infusion (central lines have too high resistance for rapid resuscitation)
Management of Haemorrhagic Shock
Step 1 - Stop the bleeding:
- External: direct pressure, tourniquet, wound packing
- Internal: emergency surgery or angioembolisation
- Haemorrhage control is the single most important step - no amount of resuscitation corrects ongoing bleeding
Step 2 - Damage Control Resuscitation (DCR):
(Bailey & Love's Surgery 28th Ed)
The four key principles of DCR:
- Rapid haemorrhage control (surgical or interventional)
- Permissive hypotension - allow SBP 80-90 mmHg (MAP ~50 mmHg) until bleeding is controlled; aggressive normalization of BP increases bleeding. Exception: Traumatic Brain Injury (maintain CPP, do not allow hypotension)
- Avoid dilutional coagulopathy - minimize crystalloid; use blood products instead
- Haemostatic resuscitation - blood products in a 1:1:1 ratio (packed red cells : fresh frozen plasma : platelets) to mimic whole blood
Additional measures:
- Tranexamic acid (TXA): antifibrinolytic; 1g IV over 10 min, then 1g over 8 hours; must be given within 3 hours of injury (after 3 hours, it is harmful)
- Warm all fluids (prevent hypothermia)
- Calcium supplementation (citrate in blood products chelates calcium)
- Type O negative blood for immediate life-threatening haemorrhage while cross-match is awaited
Step 3 - Monitor response:
- Urine output: target >0.5 mL/kg/hr (adults); >1 mL/kg/hr (children)
- Lactate clearance (normalize within 24 hours)
- Base deficit correction
- Heart rate and blood pressure normalization
Management of Septic Shock (Surviving Sepsis Bundle - 1-hour bundle)
- Blood cultures (before antibiotics)
- Broad-spectrum antibiotics within 1 hour of recognition
- IV crystalloid 30 mL/kg for hypotension or lactate ≥4 mmol/L within 3 hours
- Vasopressor (first choice: noradrenaline/norepinephrine) to achieve MAP ≥65 mmHg if fluids insufficient
- Measure serum lactate; repeat if initial >2 mmol/L
- Source control: identify and drain/remove focus of infection
Management of Cardiogenic Shock
- Treat underlying cause (reperfusion for MI - thrombolysis or primary PCI)
- Careful fluid challenge (do NOT flood the lungs)
- Inotropes (dobutamine - positive inotrope, reduces afterload)
- Mechanical support: Intra-Aortic Balloon Pump (IABP), LVAD in refractory cases
Management of Obstructive Shock
- Tension pneumothorax: Immediate needle decompression (14G, 2nd ICS, MCL) → chest drain
- Cardiac tamponade: Pericardiocentesis (needle drainage of pericardial fluid)
- Massive PE: Systemic thrombolysis or surgical embolectomy
Management of Anaphylactic Shock
- Adrenaline (epinephrine) 0.5 mg IM (1:1000 solution) immediately - repeated every 5 min
- IV fluids (large volumes)
- Antihistamines (chlorphenamine IV) + hydrocortisone IV (second line)
- Remove trigger
- Secure airway early (angioedema can close airway rapidly)
9. Type of Fluids in Shock
| Fluid | Contents | Use | Caution |
|---|---|---|---|
| Ringer's Lactate (Hartmann's) | Na, K, Ca, Cl, lactate | First-line crystalloid for haemorrhagic shock | Avoid in liver failure |
| Normal Saline (0.9% NaCl) | Na, Cl | Second-line crystalloid | Large volumes → hyperchloraemic acidosis |
| Packed Red Blood Cells | RBCs | Haemorrhagic shock | Cross-match or O-negative emergency |
| Fresh Frozen Plasma (FFP) | All clotting factors | Coagulopathy in haemorrhagic shock | 1:1:1 with PRBC and platelets |
| Albumin | Colloid | Septic shock (selected cases) | No proven mortality benefit over crystalloid |
| Dextrose | Free water | NOT used in shock (poor volume expander) | Causes hyponatraemia, cerebral oedema |
Colloids have no proven advantage over crystalloids in most studies; they are more expensive and have worse side-effect profiles - Bailey & Love's Surgery
10. Monitoring the Response to Shock Treatment
| Parameter | Target |
|---|---|
| Heart rate | <100 bpm |
| Blood pressure | SBP >90 (or MAP >65 in sepsis) |
| Urine output | >0.5 mL/kg/hr (adults) |
| Serum lactate | <2 mmol/L; clearance >10% per hour |
| Base deficit | Normalization |
| Temperature | >36°C |
| Haematocrit | Maintain >21% (Hb >7 g/dL) |
Summary Diagram of Shock
CAUSE (haemorrhage / sepsis / pump failure / obstruction)
↓
REDUCED TISSUE PERFUSION
↓
CELLULAR HYPOXIA
↓
Aerobic → Anaerobic metabolism → Lactic acidosis
↓
Na/K pump failure → Cell swelling → Lysosomal rupture → Cell death
↓
Endothelial damage → Capillary leak → Tissue oedema
↓
Coagulation activation → DIC
Immune activation → Cytokine storm
↓
ORGAN FAILURE (Lung-ARDS / Kidney-AKI / Liver / Brain)
↓
MULTIPLE ORGAN FAILURE → DEATH (60% mortality)
Sources: Bailey and Love's Short Practice of Surgery 28th Ed; Sabiston Textbook of Surgery; Robbins & Cotran Pathologic Basis of Disease 10th Ed; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.