D>abetes nephropathy
Reading File
Finding Sources
Searching PubMed
"diabetic nephropathy"[MeSH Terms] AND treatment
Reading File
Reading File
Searching PubMed
"diabetic kidney disease" AND management
Finding Sources
Finding Sources
Searching Images
diabetic nephropathy Kimmelstiel Wilson nodule glomerulosclerosis histology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Diabetic Nephropathy
Definition & Epidemiology
Diabetic nephropathy (DN) — also termed diabetic kidney disease (DKD) — is the leading cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) requiring renal replacement therapy worldwide. It accounts for nearly 50% of all patients on dialysis in the United States and affects 20–40% of all diabetic patients. The vast majority of incident cases are secondary to type 2 diabetes. It is more prevalent in Black, Native American, and Hispanic individuals, and smoking accelerates its progression.
- Goldman-Cecil Medicine, p. 1275; Harrison's Principles of Internal Medicine 22E, p. 3267
Pathogenesis
DN is a microvascular complication driven primarily by chronic hyperglycemia, acting through several overlapping mechanisms:
1. Hemodynamic Alterations
Early diabetes causes glomerular hyperfiltration — renal blood flow and GFR increase by up to 50%. The afferent arteriole dilates while the efferent arteriole constricts under angiotensin II influence, raising intraglomerular capillary pressure. This hyperfiltration initiates and perpetuates glomerular injury.
2. Structural Changes
- Glomerular basement membrane (GBM) thickening — detectable by electron microscopy within a few years of onset, even before functional changes
- Diffuse mesangial sclerosis — mesangial matrix accumulation + mesangial cell proliferation; develops in most with >10 years of disease
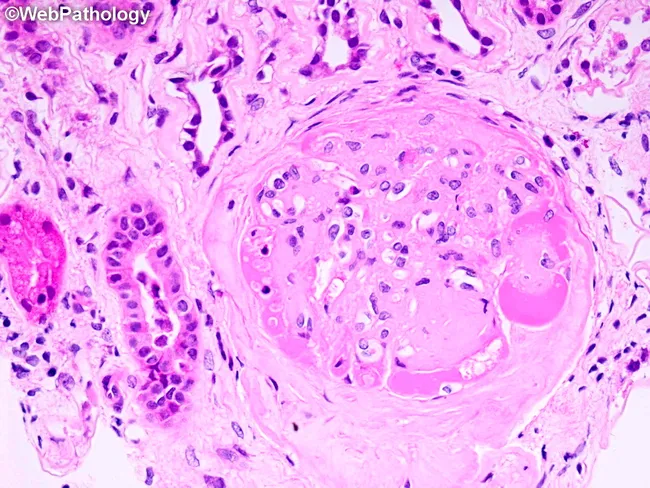
- Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion) — ball-like deposits of laminated matrix in the glomerular periphery; occurs in ~15–30% of long-term diabetics; virtually pathognomonic of diabetes
3. Soluble Mediators & Cytokines
TGF-β, connective tissue growth factor (CTGF), angiotensin II, VEGF, endothelin, prostaglandins, and nitric oxide all play roles. Angiotensin II is particularly important — RAAS blockade is standard therapy.
4. Advanced Glycation End-products (AGEs)
AGEs accumulate in the GBM and mesangium, contributing to structural changes and proteinuria.
5. Oxidative Stress & Inflammation
Reactive oxygen species accumulate; the endothelin system contributes; cytokines (IL-6, IL-10 polymorphisms) affect susceptibility especially in Asian populations.
6. Tubulointerstitial Injury
Tubular hypoxia and progressive tubulointerstitial fibrosis correlate most closely with the decline in GFR.
7. Genetic Factors
DN is likely polygenic. Siblings of type 1 diabetics with DN have >70% lifetime risk. ACE gene insertion/deletion (I/D) polymorphisms, APOL1 risk alleles (accelerate progression in Black Americans), and IL-6 gene polymorphisms have been implicated.
- Harrison's 22E, p. 3268; Goldman-Cecil Medicine, p. 1275–1276
Renal Pathology
Three categories of lesions occur:
| Category | Lesion |
|---|---|
| Glomerular | GBM thickening, diffuse mesangial sclerosis, nodular glomerulosclerosis (KW nodules) |
| Vascular | Hyaline arteriolosclerosis of both afferent and efferent arterioles (efferent involvement is virtually unique to diabetes) |
| Tubulointerstitial | Pyelonephritis, necrotizing papillitis (papillary necrosis) |
Kimmelstiel-Wilson nodules — PAS-positive, laminated mesangial nodules — are pathognomonic but present in only ~25% of cases. Differential diagnosis of nodular glomerulosclerosis includes amyloidosis, light chain nephropathy, and MPGN type II.
- Robbins & Kumar Basic Pathology, p. 751; Goldman-Cecil Medicine, p. 1276
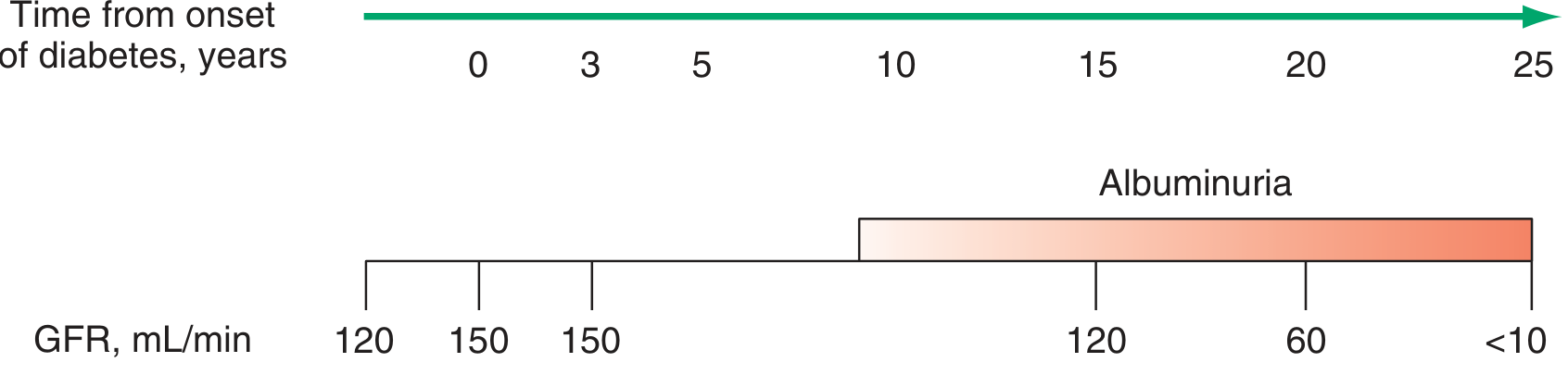
Natural History — Four Stages
| Stage | Features |
|---|---|
| I | ↑ GFR (up to 50%), renal hypertrophy, transient microalbuminuria with stress; no fixed proteinuria |
| II | Fixed microalbuminuria (30–300 mg/day); GBM thickening + mesangial expansion histologically; GFR normal or elevated; median ~10 years after DM onset; ~30% of T1DM progress here |
| III | Overt proteinuria (>500 mg/day), macroalbuminuria; eGFR begins to fall; BP rises in T1DM; worsens in T2DM |
| IV | Advanced DN — relentless GFR decline → ESRD; heavy nephrotic proteinuria (>3.5 g/day), hypertension; no RBC casts |
- Goldman-Cecil Medicine, p. 1275–1276; Harrison's 22E, p. 3268
Screening & Diagnosis
Screening uses two tests annually:
- UACR (urinary albumin-to-creatinine ratio) on spot specimen
- eGFR
Screening starts:
- Type 1 DM: 5 years after diagnosis, then annually
- Type 2 DM: at diagnosis, then annually
ADA definitions:
- Normal: UACR <30 mg/g
- Moderately increased (microalbuminuria): 30–299 mg/g
- Severely increased (macroalbuminuria): ≥300 mg/g
An elevated UACR should be confirmed on 2–3 occasions over 3–6 months (false elevation from exercise, infection, fever, CHF, severe hyperglycemia/hypertension).
Renal biopsy is rarely needed. Indicated only if another cause of renal disease is suspected (absence of retinopathy in T1DM, rapid GFR decline, active urinary sediment).
Diagnosis of overt DN requires all three: (1) proteinuria within appropriate timeframe, (2) retinopathy (90–95% in T1DM; 60–65% in T2DM), and (3) exclusion of other nephropathy causes.
- Harrison's 22E, p. 3268; Goldman-Cecil Medicine, p. 1276
Treatment
Stage-by-Stage Management
| Stage | Interventions |
|---|---|
| I | Tight glycemic control; BP control; consider ACEi/ARB |
| II | Tight glycemic control; BP control; ACEi or ARB; SGLT2 inhibitor; finerenone; smoking cessation; weight loss; exercise; annual eye exam |
| III | BP control; ACEi/ARB; SGLT2 inhibitor or GLP-1 analogue; finerenone; dietary protein restriction (0.8 g/kg/day); antihyperlipidemics |
| IV | BP control; ACEi/ARB; SGLT2 or GLP-1 (if eGFR allows); preparation for renal replacement therapy |
Key Therapeutic Agents
1. Glycemic Control
- Target HbA1c ≤7% (individualize based on comorbidities and hypoglycemia risk)
- Reversal of mesangial lesions shown after 10 years of normoglycemia post-pancreas transplant
- Sulfonylureas contraindicated in eGFR <45; metformin avoided when creatinine >1.7 mg/dL
2. Blood Pressure Control
- Target: <130/80 mmHg
- Lifestyle: sodium restriction, DASH diet, weight loss, exercise, smoking cessation
3. RAAS Blockade — ACEi or ARB (first-line with albuminuria)
- Reduces intraglomerular pressure, proteinuria, and GFR decline in both T1DM and T2DM
- Increase to maximum tolerated dose; a creatinine rise ≤30% is acceptable
- Do NOT combine ACEi + ARB (no additional benefit, more side effects)
- ARB is equivalent and preferred when ACEi causes cough or angioedema
4. SGLT2 Inhibitors (second first-line in T2DM with CKD)
- Canagliflozin, empagliflozin, dapagliflozin reduce cardiovascular events and CKD progression
- Mechanism: reduce intraglomerular pressure by increasing efferent arteriolar tone; glycosuric effect independent benefit
- Recommended when eGFR >20 mL/min/1.73 m² while continuing ACEi/ARB
- Not effective at eGFR <20; use with caution in T1DM (euglycemic DKA risk)
5. GLP-1 Receptor Agonists
- Semaglutide improves kidney outcomes and reduces cardiovascular mortality in T2DM + CKD
- Alternative when SGLT2 inhibitor is inappropriate (low eGFR, contraindication)
6. Finerenone (nonsteroidal mineralocorticoid receptor antagonist)
- Reduces cardiovascular events and CKD progression in T2DM + CKD
- Monitor serum potassium carefully
7. Lipid Management
- Dyslipidemia should be treated; statins have additional cardiovascular and possible renoprotective benefits
Other Renal Complications in DM
-
Type IV renal tubular acidosis (hyporeninemic hypoaldosteronism) → hyperkalemia; worsened by ACEi/ARBs, NSAIDs, heparin
-
Papillary necrosis — much more common in diabetics
-
Pyelonephritis — higher incidence; more severe
-
Renal artery stenosis — suspect if BP uncontrolled or creatinine rises acutely after ACEi/ARB initiation
-
Contrast nephropathy — higher risk; pre-hydration critical
-
Harrison's 22E, p. 3268–3269; Goldman-Cecil Medicine, p. 1276–1278
Recent Evidence (2024–2026)
A 2026 review in Nature Reviews Endocrinology (PMID 40935879) by Martinez Leon et al. summarizes established and emerging treatments, confirming the central role of SGLT2 inhibitors, GLP-1 agonists, and finerenone, while highlighting novel targets under investigation. No major contradictions with the above guidance were identified.
Summary of key points:
- DN is the leading cause of ESRD; affects ~20–40% of diabetics
- Pathognomonic lesion: Kimmelstiel-Wilson nodules (nodular glomerulosclerosis), present in ~25%
- Efferent + afferent arteriolar hyalinosis is distinctive to diabetes
- Screen with UACR + eGFR annually (T1DM at 5 yrs; T2DM at diagnosis)
- Treatment backbone: glycemic control + BP <130/80 + ACEi/ARB + SGLT2 inhibitor + finerenone in eligible T2DM patients
This is a shared conversation. Sign in to Orris to start your own chat.