diuretics k sembulingam book topic to take the most imp note
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
K Sembulingam Essentials Medical Physiology diuretics chapter topics classification mechanism
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have everything needed to write a complete, exam-focused set of notes on the Diuretics chapter from K. Sembulingam's textbook (Essentials of Medical Physiology), cross-referenced with authoritative pharmacology sources. Here are the most important notes:
Diuretics - K. Sembulingam (Most Important Notes)
Chapter 58/59 - Essentials of Medical Physiology
Sites of Action Along the Nephron
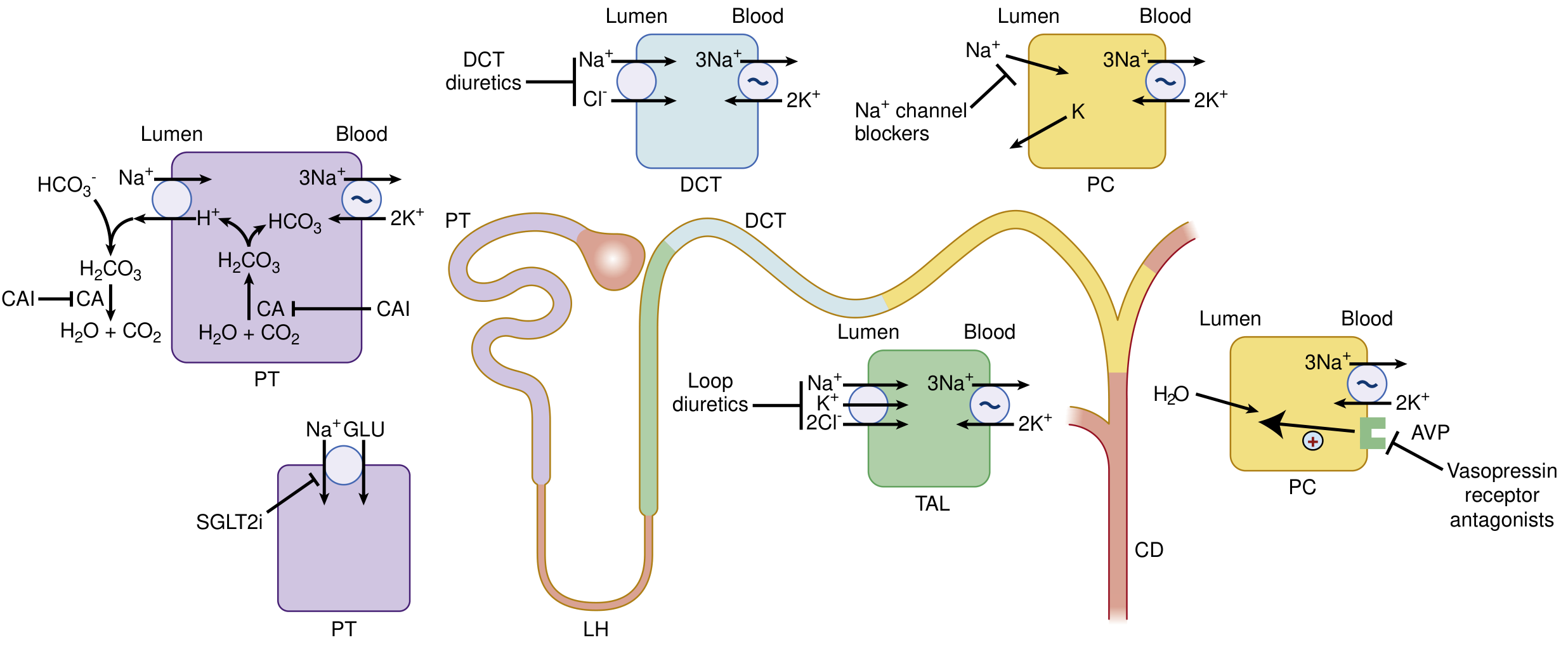
Definition
A diuretic is any substance that increases urine output (diuresis). The term specifically refers to drugs that increase renal excretion of water and solutes (mainly sodium and chloride), thereby reducing extracellular fluid volume.
Classification of Diuretics (Sembulingam - 7 Types)
| Type | Drugs |
|---|---|
| 1. Osmotic diuretics | Mannitol, Urea, Glucose |
| 2. Carbonic anhydrase inhibitors | Acetazolamide |
| 3. Loop diuretics (High-ceiling) | Furosemide, Bumetanide, Ethacrynic acid, Torsemide |
| 4. Thiazide diuretics | Hydrochlorothiazide (HCTZ), Chlorthalidone, Metolazone |
| 5. Potassium-sparing diuretics | Spironolactone, Eplerenone, Amiloride, Triamterene |
| 6. ADH antagonists (Aquaretics) | Demeclocycline, Vaptans (Tolvaptan, Conivaptan) |
| 7. Xanthine diuretics | Theophylline, Caffeine |
1. Osmotic Diuretics
Prototype: Mannitol
Site of action: Proximal tubule (PT) + Descending limb of loop of Henle
Mechanism:
- Freely filtered at glomerulus but NOT reabsorbed
- Acts as non-reabsorbable solute - retains water in tubular lumen
- Reduces medullary tonicity by washing out NaCl and urea
- Opposes ADH action in collecting tubule
- Increases urine volume >> increases NaCl excretion (water diuresis > natriuresis)
Effect on electrolytes: Increases excretion of Na+, K+, Ca2+, Mg2+, Cl-, HCO3-, phosphate
Pharmacokinetics:
- Given IV only (poorly absorbed orally - causes osmotic diarrhea)
- Not metabolized; excreted by glomerular filtration in 30-60 min
- Oral: Glycerin, Isosorbide (for reducing intraocular pressure)
Uses:
- Raised intracranial pressure (1-2 g/kg IV - reduces in 60-90 min)
- Raised intraocular pressure (before ophthalmologic procedures)
- Acute renal failure (maintain urine flow)
- Dialysis disequilibrium syndrome
- Forced diuresis in poisoning
Toxicity:
- Extracellular volume expansion + pulmonary edema (in heart failure - CONTRAINDICATED)
- Hyponatremia (initial dilutional)
- Hypernatremia (after prolonged use - water loss exceeds Na loss)
- Contraindicated in: anuric renal failure, pulmonary edema, heart failure
2. Carbonic Anhydrase Inhibitors (CAIs)
Prototype: Acetazolamide
Site: Proximal tubule
Mechanism:
- Inhibits carbonic anhydrase (CA) enzyme
- CA normally: H2O + CO2 → H2CO3 → H+ + HCO3-
- Inhibition → less H+ available → less Na+/H+ exchange via NHE-3
- Result: Na+, HCO3- retained in urine → alkaline diuresis
- Self-limiting: once plasma HCO3- falls (metabolic acidosis), effect wanes
Effect: Alkaline urine (↑HCO3-, ↑Na+, ↑K+) - relatively weak diuretic
Uses:
- Glaucoma (main use - reduces aqueous humor formation)
- Altitude sickness (mountain sickness prophylaxis)
- Alkalinizing urine (cystinuria, uric acid stones)
- Correcting metabolic alkalosis from thiazide/loop diuretics
- Epilepsy (petit mal seizures)
Toxicity:
- Metabolic acidosis (hyperchloremic)
- Hypokalemia
- Renal stones (alkaline urine + reduced citrate)
- Drowsiness, paresthesia
- Sulfonamide allergy cross-reactivity
3. Loop Diuretics (High-Ceiling Diuretics)
Prototype: Furosemide (Lasix)
Site: Thick ascending limb (TAL) of loop of Henle
Mechanism:
- Inhibits Na+/K+/2Cl- cotransporter (NKCC2) on luminal membrane of TAL
- Blocks reabsorption of NaCl, destroys medullary concentration gradient
- Also abolishes the positive luminal potential → reduces Ca2+ and Mg2+ reabsorption
- "High ceiling" = dose-response curve is steep; can produce very large diuresis
Effect on electrolytes:
- ↑Na+, ↑Cl-, ↑K+ loss → hypokalemic metabolic alkalosis
- ↑Ca2+ excretion (calciuric) - useful in hypercalcemia
- ↑Mg2+ excretion
Drugs:
- Furosemide - sulfonamide; oral + IV; duration 2-4 hours
- Bumetanide - sulfonamide; 40x more potent than furosemide
- Torsemide - sulfonamide; longer duration
- Ethacrynic acid - NOT a sulfonamide (use in sulfa allergy); also uricosuric; most ototoxic
Uses:
- Acute pulmonary edema (IV furosemide - drug of choice)
- Heart failure (edema management)
- Hypertension (especially with renal impairment)
- Acute hypercalcemia (with IV saline)
- Nephrotic syndrome, cirrhosis with ascites
- Anion overdose (forced diuresis)
- Hyperkalemia (acute management)
Toxicity - ABCDEF:
- A - Alkalosis (hypokalemic metabolic alkalosis)
- B - Blood disorders (rare)
- C - Ca2+ loss (hypocalcemia with long use), Cholesterol ↑
- D - Dehydration, Dizziness
- E - Electrolyte disturbances (↓K+, ↓Na+, ↓Mg2+)
- F - Furosemide Ototoxicity (tinnitus, deafness - dose-dependent, more with aminoglycosides)
- Also: Hyperuricemia (compete with uric acid for tubular secretion), Hyperglycemia
4. Thiazide Diuretics
Prototype: Hydrochlorothiazide (HCTZ)
Site: Distal convoluted tubule (DCT)
Mechanism:
- Inhibits Na+/Cl- cotransporter (NCC) in DCT
- Modest increase in NaCl excretion (~3-5% of filtered load)
- Reduces plasma volume → activates RAAS → K+ loss
Effect on electrolytes:
- ↑Na+, ↑Cl-, ↑K+ loss → hypokalemic metabolic alkalosis
- ↓Ca2+ excretion (hypocalciuric) - KEY DISTINCTION from loop diuretics
- Mechanism of hypocalciuria: volume depletion → ↑proximal Ca2+ reabsorption; also direct DCT Ca2+ channel upregulation
Drugs:
- HCTZ - standard; oral; 8-12 h duration
- Chlorthalidone - very long t1/2 (50-60 h) - binds RBCs; preferred for hypertension
- Metolazone - used with loop diuretics for synergy (sequential nephron blockade)
- Indapamide - loop of Henle component; used in hypertension
- Chlorothiazide - only IV thiazide available
Uses:
- Hypertension (first-line, especially uncomplicated)
- Mild heart failure
- Nephrolithiasis due to hypercalciuria (reduces urinary Ca2+)
- Nephrogenic diabetes insipidus (paradoxical - reduces free water by volume contraction)
- Osteoporosis (reduces Ca2+ loss)
Toxicity - GHIK:
- G - Gout (hyperuricemia)
- H - Hyperglycemia (impairs insulin release, increases insulin resistance)
- I - Increased LDL/triglycerides
- K - K+ loss (hypokalemia)
- Also: Hyponatremia (SIADH-like), sexual dysfunction, sulfonamide allergy
Thiazides are INEFFECTIVE when GFR < 30 mL/min (except metolazone - still works)
5. Potassium-Sparing Diuretics
Site: Collecting duct (CD) / Late distal tubule
A. Aldosterone Antagonists
Drugs: Spironolactone, Eplerenone
Mechanism:
- Competitively antagonize aldosterone at mineralocorticoid receptors
- Aldosterone normally → transcription of Na+ channels (ENaC) and Na+/K+ ATPase → Na+ retention + K+ secretion
- Blockade → less Na+ reabsorption, less K+ secretion → K+ sparing
- Slow onset (2-3 days) because must wait for existing aldosterone-stimulated proteins to degrade
Spironolactone vs Eplerenone:
- Spironolactone: also blocks androgen + progesterone receptors → gynecomastia, impotence, menstrual irregularity
- Eplerenone: selective for mineralocorticoid receptor only → no hormonal side effects; more expensive
Uses:
- Primary aldosteronism (Conn's syndrome) - diagnostic + therapeutic
- Heart failure (reduces mortality in severe HF - RALES trial)
- Cirrhosis with ascites
- Hypokalemia from other diuretics (combination therapy)
- Post-MI (eplerenone)
- Hirsutism in women (spironolactone's antiandrogenic effect)
B. ENaC Blockers
Drugs: Amiloride, Triamterene
Mechanism:
- Directly block epithelial Na+ channels (ENaC) in collecting duct
- Act independent of aldosterone levels
- Weak diuretics; mainly used to prevent K+ loss with other diuretics
Amiloride extra uses:
- Reduces lithium-induced polyuria (blocks Li+ entry via ENaC)
- Liddle syndrome (gain-of-function ENaC mutation)
Key toxicity for ALL K+-sparing diuretics:
- Hyperkalemia - can be fatal (especially in renal failure, diabetes, with ACE inhibitors/ARBs/NSAIDs)
- Triamterene: nephrolithiasis (triamterene stones), megalo-blastic anemia (folate antagonism)
- Spironolactone: gynecomastia, menstrual irregularities
6. ADH Antagonists (Vaptans / Aquaretics)
Drugs: Tolvaptan (oral), Conivaptan (IV), Demeclocycline
Site: Collecting duct
Mechanism:
- Block V2 vasopressin receptors → reduce aquaporin-2 insertion → free water diuresis WITHOUT significant Na+ loss ("aquaresis")
Uses:
- SIADH (hyponatremia)
- Euvolemic/hypervolemic hyponatremia
- Heart failure, cirrhosis-related hyponatremia
- Polycystic kidney disease (tolvaptan - slows progression)
Key concern: Risk of overly rapid correction of hyponatremia → osmotic demyelination syndrome (central pontine myelinolysis)
7. Xanthine Diuretics
Drugs: Theophylline, Caffeine, Aminophylline
Mechanism:
- Inhibit phosphodiesterase → ↑cAMP
- Increase renal blood flow and GFR (mild)
- Weak direct tubular effects
- Weakest class of diuretics - rarely used primarily as diuretics
High-Yield Comparison Table
| Feature | Loop | Thiazide | K+-sparing | CAI | Osmotic |
|---|---|---|---|---|---|
| Site | TAL | DCT | CD | PT | PT + LOH |
| Potency | Highest | Moderate | Low | Low | Moderate |
| K+ effect | ↓ (wasting) | ↓ (wasting) | ↑ (sparing) | ↓ | ↓ |
| Ca2+ effect | ↑ (calciuric) | ↓ (hypocalciuric) | No change | ↓ | ↑ |
| Urine pH | Alkaline | Alkaline | Acidic | Alkaline | Neutral |
| Acid-base | Metabolic alkalosis | Metabolic alkalosis | Metabolic acidosis | Metabolic acidosis | Neutral |
| Uric acid | ↑ (hyperuricemia) | ↑ (hyperuricemia) | No change | - | - |
| Glucose | ↑ mild | ↑ (hyperglycemia) | No change | - | - |
| Works in renal failure? | Yes | No (except metolazone) | Avoid | No | Avoid |
Most Important Clinical Points (Exam Favorites)
"Paradoxical" effects (frequently asked):
- Thiazides in nephrogenic DI - cause volume contraction → proximal tubule reabsorbs more → less water to diluting segment → paradoxically reduces polyuria
- Furosemide in hypercalcemia - calciuric; given with IV saline
- Thiazides in hypercalciuria/calcium stones - reduce urinary calcium
Drug of choice scenarios:
| Condition | Diuretic of Choice |
|---|---|
| Acute pulmonary edema | Furosemide (IV) |
| Hypertension (uncomplicated) | Thiazide (HCTZ / Chlorthalidone) |
| Primary aldosteronism | Spironolactone |
| Raised ICP | Mannitol |
| Hypercalcemia (acute) | Furosemide + IV saline |
| Nephrogenic DI | Thiazide (amiloride as second choice) |
| SIADH | Tolvaptan or fluid restriction |
| Heart failure (mortality benefit) | Spironolactone/Eplerenone |
| Glaucoma | Acetazolamide |
| Sulfa allergy + needs loop diuretic | Ethacrynic acid |
| Liddle syndrome | Amiloride |
| Conn's syndrome (diagnosis) | Spironolactone |
Ototoxicity:
- Loop diuretics (especially ethacrynic acid > furosemide)
- Enhanced by concurrent aminoglycosides
Hyperuricemia:
- Loop diuretics and thiazides both cause hyperuricemia (compete with uric acid for OAT secretion)
- Ethacrynic acid is actually uricosuric (unique - promotes uric acid excretion)
K+ effects - rule of thumb:
- Loop + Thiazide = K+ wasting
- K+-sparing = K+ retention
- Combining loop/thiazide + K+-sparing = balanced K+ effect (e.g., furosemide + spironolactone in cirrhosis)
RAAS activation:
- Loop and thiazide → volume depletion → ↑renin → ↑angiotensin II → ↑aldosterone → exacerbates K+ loss
- K+-sparing diuretics blunt this secondary effect
Side Effects Memory Aid
Furosemide OHHHH:
- Ototoxicity
- Hypokalemia
- Hyperuricemia
- Hypomagnesemia
- Hyponatremia
Spironolactone GAME:
- Gynecomastia
- Anti-androgenic effects
- Menstrual irregularity
- Electrolyte: Hyperkalemia
Thiazides GHIICK:
- Gout
- Hyperglycemia
- Impotence
- Increased cholesterol
- Calcium (decreased in urine)
- K+ loss (hypokalemia)
Sources: Essentials of Medical Physiology (K. Sembulingam, 7th/8th ed.) cross-referenced with Katzung's Basic and Clinical Pharmacology 16e, National Kidney Foundation Primer on Kidney Diseases 8e, and Goodman & Gilman's Pharmacological Basis of Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.