Make a algorithm of accidental hypothermia treatment as per latest updated guidelines of wilderness medical society
Wilderness Medical Society accidental hypothermia treatment guidelines 2024 2025
accidental hypothermia treatment guidelines wilderness
https://www.wildmedcenter.com/uploads/5/9/8/2/5982510/wms_hy…
PMID: 41128452
WMS hypothermia guidelines 2024 update Dow Giesbrecht Danzl accidental hypothermia algorithm ECMO cardiac arrest
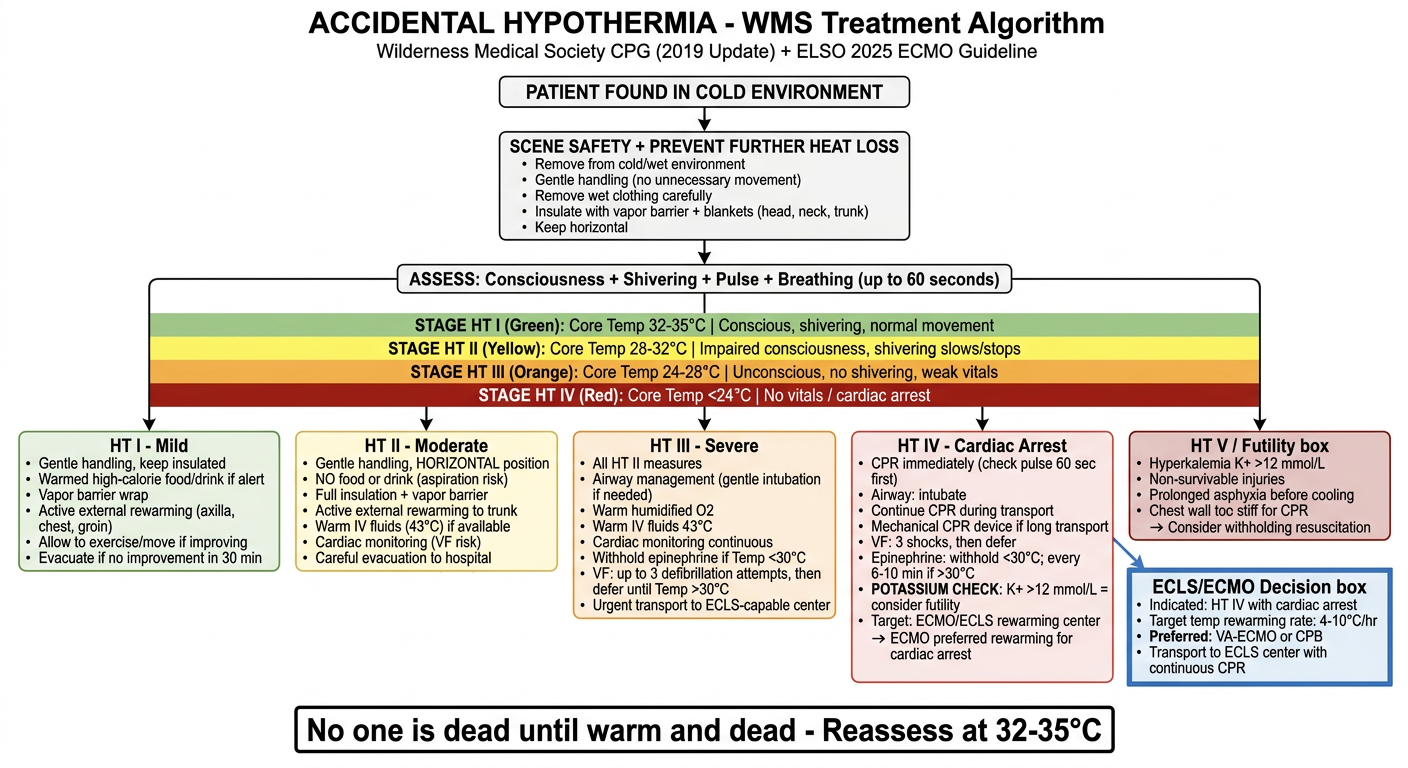
A detailed clinical treatment algorithm flowchart for accidental hypothermia based on Wilderness Medical Society guidelines. The flowchart should show: Title at top: "ACCIDENTAL HYPOTHERMIA - WMS Treatment Algorithm" Subtitle: "Wilderness Medical Society CPG (2019 Update) + ELSO 2025 ECMO Guideline" Starting box: "PATIENT FOUND IN COLD ENVIRONMENT" Flow down to: "SCENE SAFETY + PREVENT FURTHER HEAT LOSS" - Remove from cold/wet environment - Gentle handling (no unnecessary movement) - Remove wet clothing carefully - Insulate with vapor barrier + blankets (head, neck, trunk) - Keep horizontal Next branch: "ASSESS: Consciousness + Shivering + Pulse + Breathing (up to 60 seconds)" Swiss Staging System shown as colored horizontal bands: - STAGE HT I (Green): Core Temp 32-35°C | Conscious, shivering, normal movement - STAGE HT II (Yellow): Core Temp 28-32°C | Impaired consciousness, shivering slows/stops - STAGE HT III (Orange): Core Temp 24-28°C | Unconscious, no shivering, weak vitals - STAGE HT IV (Red): Core Temp <24°C | No vitals / cardiac arrest - STAGE HT V (Dark Red): Hypothermic death For each stage, treatment boxes: HT I - Mild: • Gentle handling, keep insulated • Warmed high-calorie food/drink if alert • Vapor barrier wrap • Active external rewarming (axilla, chest, groin) • Allow to exercise/move if improving • Evacuate if no improvement in 30 min HT II - Moderate: • Gentle handling, HORIZONTAL position • NO food or drink (aspiration risk) • Full insulation + vapor barrier • Active external rewarming to trunk • Warm IV fluids (43°C) if available • Cardiac monitoring (VF risk) • Careful evacuation to hospital HT III - Severe: • All HT II measures • Airway management (gentle intubation if needed) • Warm humidified O2 • Warm IV fluids 43°C • Cardiac monitoring continuous • Withhold epinephrine if Temp <30°C • VF: up to 3 defibrillation attempts, then defer until Temp >30°C • Urgent transport to ECLS-capable center HT IV - Cardiac Arrest: • CPR immediately (check pulse 60 sec first) • Airway: intubate • Continue CPR during transport • Mechanical CPR device if long transport • VF: 3 shocks, then defer • Epinephrine: withhold <30°C; every 6-10 min if >30°C • POTASSIUM CHECK: K+ >12 mmol/L = consider futility • Target: ECMO/ECLS rewarming center • ECMO preferred rewarming for cardiac arrest HT V / Futility box: • Hyperkalemia K+ >12 mmol/L • Non-survivable injuries • Prolonged asphyxia before cooling • Chest wall too stiff for CPR → Consider withholding resuscitation ECLS/ECMO Decision box (separate): • Indicated: HT IV with cardiac arrest • Target temp rewarming rate: 4-10°C/hr • Preferred: VA-ECMO or CPB • Transport to ECLS center with continuous CPR Bottom note: "No one is dead until warm and dead - Reassess at 32-35°C" Clean medical infographic style with white background, color-coded stages, clear arrows, professional typography
Accidental Hypothermia - WMS Treatment Algorithm
Note: There is no standalone WMS "2024 update" specifically for hypothermia as of June 2026. The 2019 version remains the current WMS CPG. It is supplemented here by the 2025 ELSO ECMO guideline.
STEP 0 - SCENE SAFETY & UNIVERSAL PRECAUTIONS
- Ensure rescuer safety first
- Prevent further cooling in ALL patients before any other intervention
- Remove from cold/wet environment; remove wet clothing gently
- Keep patient horizontal to avoid "rescue collapse" (orthostatic hypotension)
- Insulate with vapor barrier + sleeping bag/blanket (especially head, neck, trunk)
SWISS STAGING SYSTEM (Clinical Field Diagnosis)
| Stage | Core Temp | Consciousness | Shivering | Vitals | Key Presentation |
|---|---|---|---|---|---|
| HT I | 35-32°C | Alert, normal | Present | Stable | "Cold and shivering" |
| HT II | 32-28°C | Impaired | Slows/stops | Stable | "Cold and not shivering" |
| HT III | 28-24°C | Unconscious | Absent | Unstable (present) | "Cold and unconscious with pulse" |
| HT IV | <24°C | Unconscious | Absent | Cardiac arrest | "No vital signs" |
| HT V | Any | - | - | - | Hypothermic death (non-survivable) |
STEP 1 - INITIAL ASSESSMENT (ALL PATIENTS)
- Check for breathing and pulse for up to 60 seconds (hypothermia causes profound bradycardia and slow breathing - do not assume death prematurely)
- Assess consciousness (GCS, verbal response)
- Assess shivering (present, diminished, absent)
- ECG/cardiac monitoring if available (look for J/Osborn waves, VF)
- Core temp if equipment available (esophageal preferred; rectal acceptable)
STAGE HT I - MILD (35-32°C)
- Handle gently; sit or lie down for at least 30 minutes
- Insulate with vapor barrier (especially head/neck) + sleeping bag
- Apply active external heat to axillae, chest, groin (chemical heat packs, warm water bottles - cover with cloth to prevent burns)
- Warmed, high-calorie food and drink if patient is alert and no aspiration risk
- Allow gentle exercise/movement if improving after warming period
- Evacuate if no improvement within 30 minutes or clinical deterioration
STAGE HT II - MODERATE (32-28°C)
- Gentle handling is critical - sudden movement can precipitate VF
- Keep strictly horizontal
- No food or drink (aspiration risk)
- Full body insulation with vapor barrier
- Active external rewarming to trunk (axillae, chest, neck, groin) - avoid limbs to prevent "after-drop"
- Warm IV/IO fluids (43°C) if available
- Continuous cardiac monitoring - high risk for VF
- Supplemental warm humidified O2 if available
- Careful evacuation to hospital with rewarming capability
STAGE HT III - SEVERE (28-24°C)
- Airway management: gentle orotracheal intubation if airway compromised (use caution - stimulation can trigger VF)
- Warm humidified O2 (42-46°C) via ventilator/BVM
- Warm IV fluids 43°C
- Cardiac instability: SBP <90 mmHg or HR <30 bpm = transfer immediately to ECLS-capable center
- VF management:
- Attempt defibrillation up to 3 shocks
- If VF persists, defer further shocks until core temp >30°C
- Withhold epinephrine if Temp <30°C
- If Temp >30°C: epinephrine every 6-10 minutes (extended interval vs. normothermic protocol)
- Urgent transfer to ECLS/ECMO-capable center
STAGE HT IV - CARDIAC ARREST (<24°C)
CPR Decision:
| Condition | Action |
|---|---|
| Cardiac arrest with survivable mechanism | Start CPR immediately |
| Chest wall too stiff for compressions | Defer CPR, transport immediately |
| Dangerous terrain / unsafe CPR | Delayed/intermittent CPR permitted |
| Prolonged asphyxia (burial >60 min) + K+ >12 mmol/L | Consider withholding CPR |
CPR Protocol:
- Standard compression:ventilation ratio (30:2 or continuous with advanced airway)
- Continuous CPR during transport; use mechanical CPR device (e.g., LUCAS) if prolonged transport or difficult terrain
- Intermittent CPR (5 min on, 5 min off) only if continuous CPR is impossible
Drug Protocol:
| Temperature | Epinephrine | Defibrillation |
|---|---|---|
| <30°C | Withhold | Max 3 shocks, then defer |
| 30-35°C | Every 6-10 min (not standard 3-5 min) | Standard protocol |
| >35°C | Standard protocol | Standard protocol |
ECMO/ECLS - PRIMARY REWARMING FOR HT IV:
- VA-ECMO (venoarterial) or cardiopulmonary bypass (CPB) is the preferred rewarming method for hypothermic cardiac arrest
- Rewarming rate: 4-10°C/hour
- Continue CPR throughout transport to ECLS center
- Transfer criteria: patient with hypothermic arrest, no non-survivable injury, potassium <12 mmol/L
Potassium as Futility Marker:
| K+ Level | Interpretation |
|---|---|
| <8 mmol/L | Attempt ECMO rewarming |
| 8-12 mmol/L | Consider - individualize decision |
| >12 mmol/L | Non-survivable - withhold/cease CPR |
STAGE HT V - DECLARE DEATH / WITHHOLD RESUSCITATION
- Serum potassium >12 mmol/L (cell lysis indicates lethal tissue damage)
- Non-survivable injuries (decapitation, chest crushed, rigor mortis with no hypothermia)
- Avalanche burial >60 minutes + in cardiac arrest + obstructed airway on extrication
- Prolonged asphyxia clearly preceding the hypothermia
Core WMS principle: "No one is dead until warm and dead" - a patient should not be pronounced dead until rewarmed to 30-35°C with persistent cardiac arrest.
REWARMING METHODS SUMMARY
| Method | Rate | Indication |
|---|---|---|
| Passive external (insulation, remove from cold) | 0.5-2°C/hr | HT I only |
| Active external (heating pads, warm packs to trunk) | 1-2°C/hr | HT I, HT II |
| Warm humidified O2 (42-46°C) | 1-1.5°C/hr | HT II-IV adjunct |
| Warm IV fluids (43°C) | 0.5-1°C/hr | HT II-IV adjunct |
| Body-to-body | 0.5-1°C/hr | Field/wilderness only |
| Warm water immersion (40°C) | 2-3°C/hr | Hospital/controlled setting |
| Bladder/peritoneal lavage (43°C saline) | 1.5-3°C/hr | Hospital, HT III-IV |
| Thoracic lavage (sterile saline 42°C) | 3-6°C/hr | Hospital, cardiac arrest |
| CVVHF/Dialysis | 2-3°C/hr | Hospital, if ECMO unavailable |
| ECMO/CPB | 4-10°C/hr | HT IV - cardiac arrest; PREFERRED |
KEY EVIDENCE UPDATES (2024-2025)
- ELSO 2025 (PMID: 41128452): Formalizes VA-ECMO as standard of care for hypothermic cardiac arrest in ECLS-capable centers; recommends continuous CPR during inter-hospital transport
- K+ >12 mmol/L remains the most robust futility marker (supported across WMS, ERC, ILCOR)
- Epinephrine withholding below 30°C is an important distinction from standard ACLS - drug metabolism is severely impaired and epinephrine can trigger VF
- Osborn/J-waves on ECG are pathognomonic of hypothermia but do not correlate with severity or predict VF
- Avalanche-specific: burial >60 min + arrest + airway obstruction = very poor prognosis; add K+ check before ECMO