Guyton & Hall (Cardiac Failure and Body Fluid Regulation chapters Explained in easy term but in detailed with diagrams and chart
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content and all the key diagrams. Let me compose the full detailed explanation.
Guyton & Hall: Cardiac Failure & Body Fluid Regulation - Explained Simply but in Full Detail
Source: Guyton and Hall Textbook of Medical Physiology (ISBN 9780443111013)
PART 1: CARDIAC FAILURE (Chapter 22)
What is Heart Failure?
Heart failure means the heart cannot pump enough blood to meet the body's needs. Think of the heart as a water pump in a building. If the pump weakens, the building gets too little water pressure, and water backs up in the pipes. The same thing happens in the body.
Section 1: Acute Effects - What Happens Immediately
When the heart is suddenly damaged (like a heart attack / myocardial infarction), two things happen within seconds:
- Cardiac output drops (less blood pumped out)
- Blood dams up in the veins (venous/right atrial pressure rises)
Fig. 22.1 - Progressive changes after acute myocardial infarction:
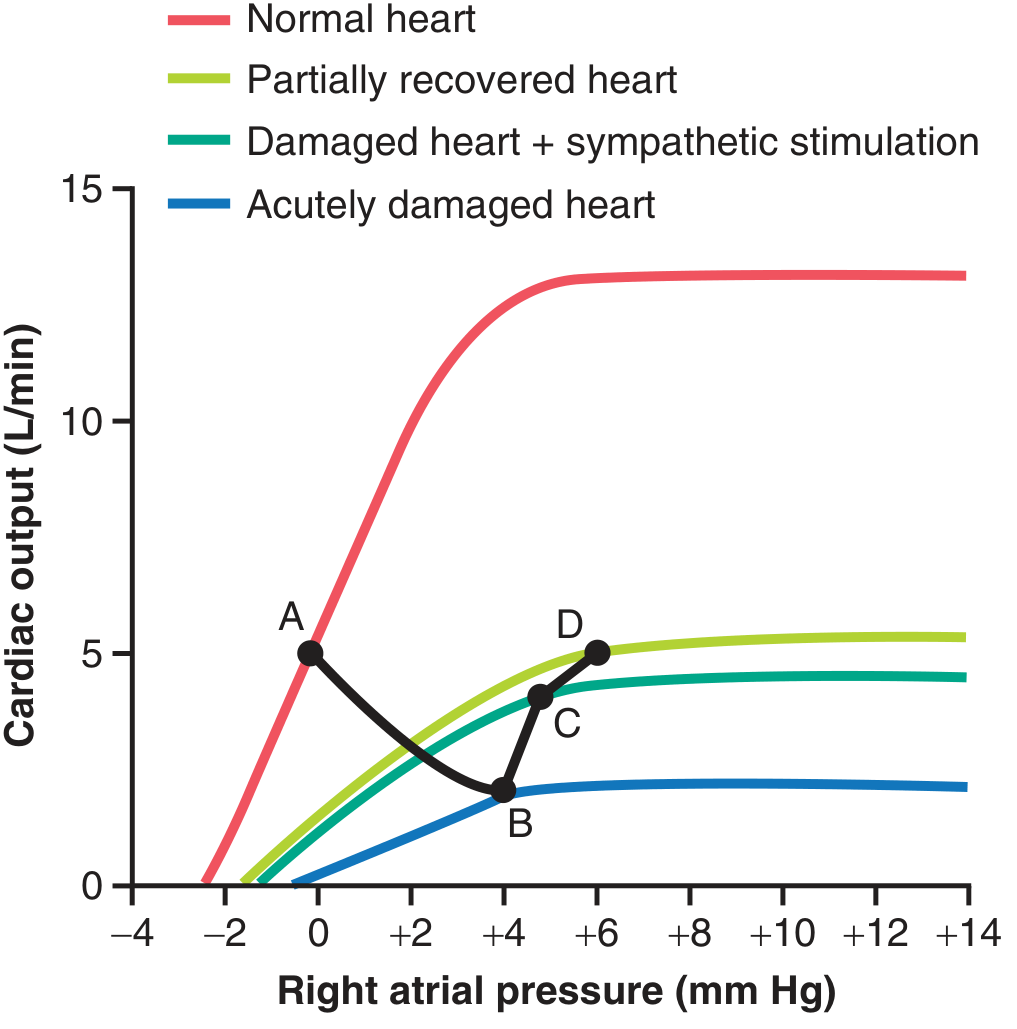
Reading the graph:
| Point | State | Cardiac Output | Right Atrial Pressure |
|---|---|---|---|
| A | Normal | 5 L/min | 0 mm Hg |
| B | Immediately after MI | 2 L/min | +4 mm Hg |
| C | After sympathetic kick | ~4 L/min | +5 mm Hg |
| D | After partial recovery + fluid retention | ~5 L/min | +6 mm Hg |
Section 2: The Body's Emergency Response - Sympathetic Rescue
When the heart fails, the body hits the "emergency button" within seconds:
What the sympathetic nervous system does:
- Strengthens the damaged heart muscle - makes whatever is left pump harder
- Speeds up the heart rate - to try to maintain output
- Squeezes veins - raises mean systemic filling pressure from ~7 mm Hg to 12-14 mm Hg (almost doubles it), pushing more blood back to the heart
- Constricts peripheral arteries - raises blood pressure
The net result: cardiac output often rises from 2 L/min back up to about 4-4.5 L/min within minutes. This is called compensated heart failure - the body buys time.
Simple analogy: Like a car running on 3 cylinders. The engine compensates by working harder. You can still drive, but you can't race.
Section 3: Chronic Compensation - Fluid Retention
Over the next days to weeks, another rescue mechanism kicks in:
Why the kidneys retain fluid in heart failure:
When cardiac output falls, the kidneys don't get enough blood flow. They interpret this as "the body is dehydrated" and try to retain fluid. Three mechanisms drive this:
-
Reduced glomerular filtration rate (GFR) - Less blood in = less urine out. Cardiac output at half-normal can cause almost complete anuria.
-
Renin-Angiotensin system activation:
- Low kidney blood flow → kidneys release renin
- Renin → Angiotensin I → Angiotensin II
- Angiotensin II constricts kidney arterioles further AND stimulates tubular cells to reabsorb sodium and water
- Result: massive fluid retention
-
Aldosterone secretion:
- Angiotensin II stimulates the adrenal gland to release aldosterone
- Aldosterone tells kidney tubules to keep sodium (and water follows sodium)
- Even more fluid is retained
The outcome: More fluid in the body raises venous pressure, which pushes more blood back to the heart, which raises cardiac output back toward 5 L/min. This is the body trying to restore kidney function.
Section 4: Why There Is NO Peripheral Edema Acutely
This is a key exam point. In acute heart failure, peripheral edema does NOT appear immediately. Here's why:
Fig. 22.3 - Pressure changes as cardiac output falls:
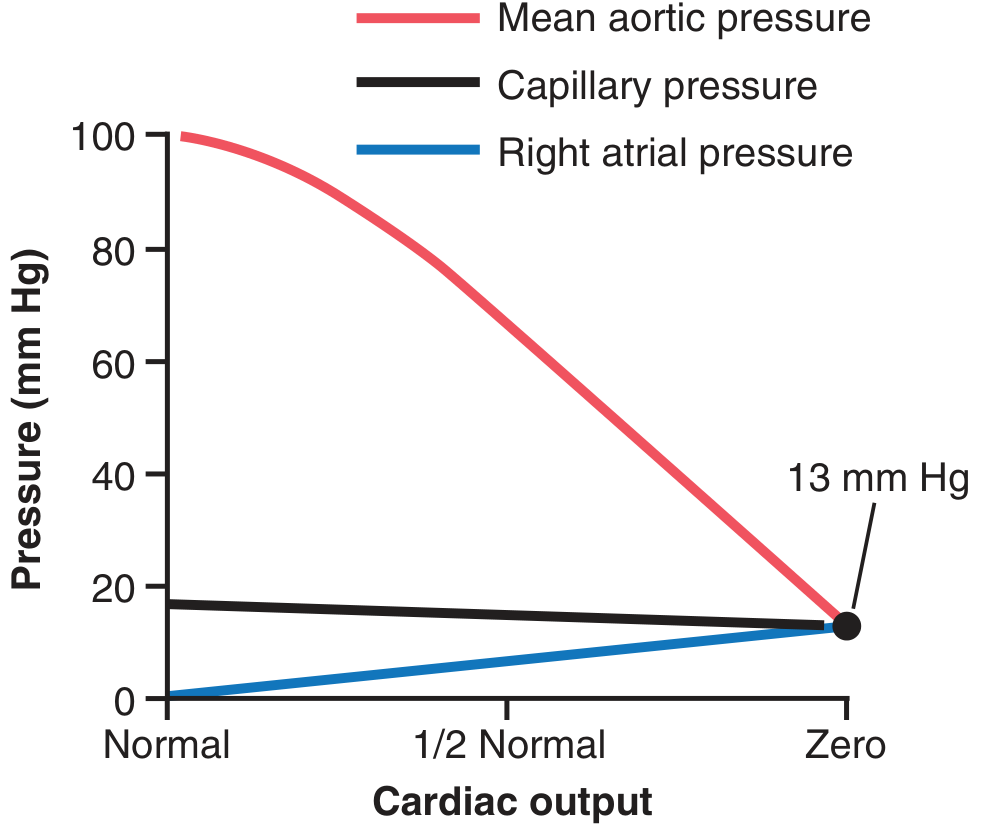
As cardiac output falls toward zero:
- Mean aortic pressure falls from 100 mm Hg → 13 mm Hg
- Right atrial pressure rises from 0 → 13 mm Hg
- Capillary pressure actually falls from 17 mm Hg → 13 mm Hg
Since capillary pressure falls, fluid is not pushed out of capillaries into tissues. No edema yet.
Peripheral edema only appears after 1-2 days, when kidney fluid retention raises total body fluid volume enough to elevate venous and capillary pressures.
Section 5: How Chronic Heart Failure Causes Edema
After 1-2 days of fluid retention:
Heart fails → Low cardiac output
↓
Kidneys retain Na+ and water (RAAS activated)
↓
Blood volume increases → Mean systemic filling pressure rises
↓
More blood returns to heart (venous return ↑)
↓
Right atrial pressure rises → Capillary pressure rises
↓
Fluid leaks out of capillaries into tissues = EDEMA
The three causes of reduced kidney output in heart failure:
| Cause | Mechanism |
|---|---|
| Reduced GFR | Low renal blood flow, afferent arteriole constriction |
| RAAS activation | Angiotensin II → Na+ and H2O reabsorption |
| Aldosterone excess | Tubular Na+ retention → water follows |
Section 6: Decompensated Heart Failure - When the Body Loses the Fight
Fig. 22.2 - The downward spiral of decompensated heart failure:
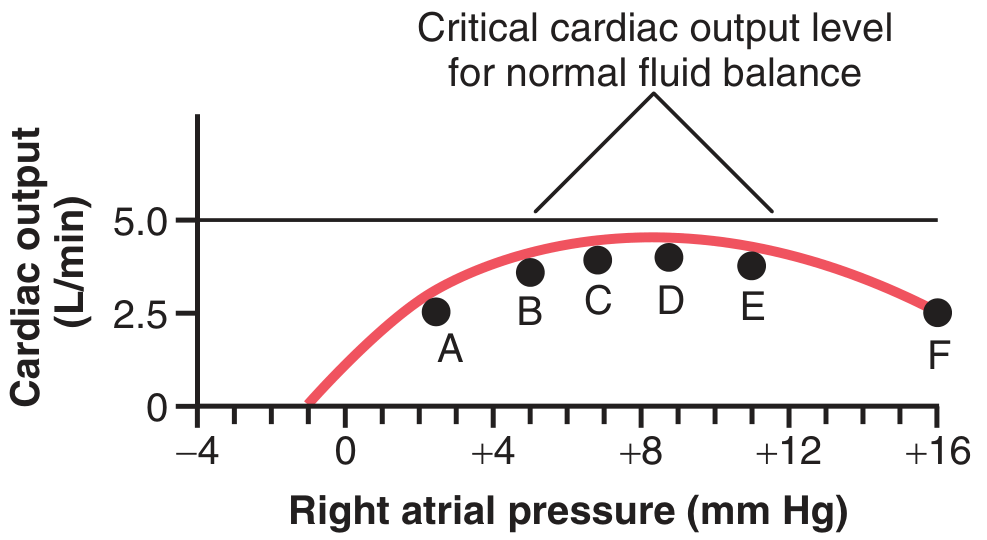
The critical cardiac output for normal kidney function is 5 L/min. If the heart is too damaged to reach this level, a fatal vicious cycle begins:
| Stage | Event |
|---|---|
| Point A | Initial failure - CO ~2.5 L/min, low RAP |
| Point B | Sympathetic compensation - CO rises to ~3.5 L/min, RAP +5 |
| Points C, D, E | Day by day fluid retention raises RAP further; CO stays below 5 L/min |
| Point F | Heart muscle becomes overstretched + edematous; begins to FAIL further → death |
The key insight: The heart never gets cardiac output above 5 L/min, so kidneys never excrete enough fluid. More and more fluid accumulates. The overfilled heart becomes overstretched and weakens further (like a balloon over-inflated). This is the vicious cycle of decompensation.
Section 7: Unilateral Left Heart Failure - Pulmonary Edema
When only the left heart fails:
- Blood dams up in the pulmonary circulation (lungs)
- Pulmonary capillary pressure rises sharply
- Fluid leaks into lung tissue = pulmonary edema
- Patient becomes severely breathless (pink frothy sputum in extreme cases)
Left failure: affects lungs first
Right failure OR biventricular failure: affects body (peripheral edema, ascites, hepatomegaly)
Section 8: Low-Output vs. High-Output Heart Failure
| Type | Description | Examples |
|---|---|---|
| Low-output HF | Heart can't pump enough (most common) | MI, cardiomyopathy, hypertension |
| High-output HF | Body demands MORE than a normal heart can supply | Anemia, thyrotoxicosis, AV fistula, beriberi |
In high-output failure, the cardiac output may actually be above normal - but still isn't enough for what the body needs.
Section 9: HFrEF vs. HFpEF
| Feature | HFrEF (Reduced EF) | HFpEF (Preserved EF) |
|---|---|---|
| Ejection fraction | < 40% | ≥ 50% |
| Problem | Heart can't squeeze | Heart can't relax/fill |
| Common cause | MI, dilated cardiomyopathy | Hypertension, obesity, diabetes |
| Treatments with proven mortality benefit | ACE-i, ARB, ARNI, beta-blockers, MRA, SGLT2-i | SGLT2-i, MRA (reduce hospitalizations) |
Section 10: Treatment of Chronic Heart Failure
The treatments target the very compensatory mechanisms that eventually become harmful:
| Drug Class | Target | Effect |
|---|---|---|
| ACE inhibitors / ARBs | Block Angiotensin II | Reduce Na+/water retention; reduce afterload |
| ARNI (sacubitril/valsartan) | Block Ang II + preserve natriuretic peptides | More natriuresis + diuresis |
| Aldosterone antagonists (spironolactone) | Block aldosterone | Reduce Na+ retention; prevent cardiac/renal fibrosis |
| Beta-blockers | Reduce sympathetic drive | Less myocardial O2 consumption, less workload |
| SGLT2 inhibitors | Multiple (anti-fibrotic, natriuresis, metabolism) | Reduce hospitalizations in both HFrEF and HFpEF |
| Diuretics (furosemide) | Directly remove excess fluid | Relieve congestion and edema |
Note: Beta-blockers should NOT be given in decompensated heart failure because the failing heart relies on sympathetic drive to maintain output.
PART 2: BODY FLUID REGULATION (Chapter 25 + Related Chapters)
Body Fluid Compartments - The Big Picture
Fig. 25.1 - Body fluid compartments for a 70-kg man:
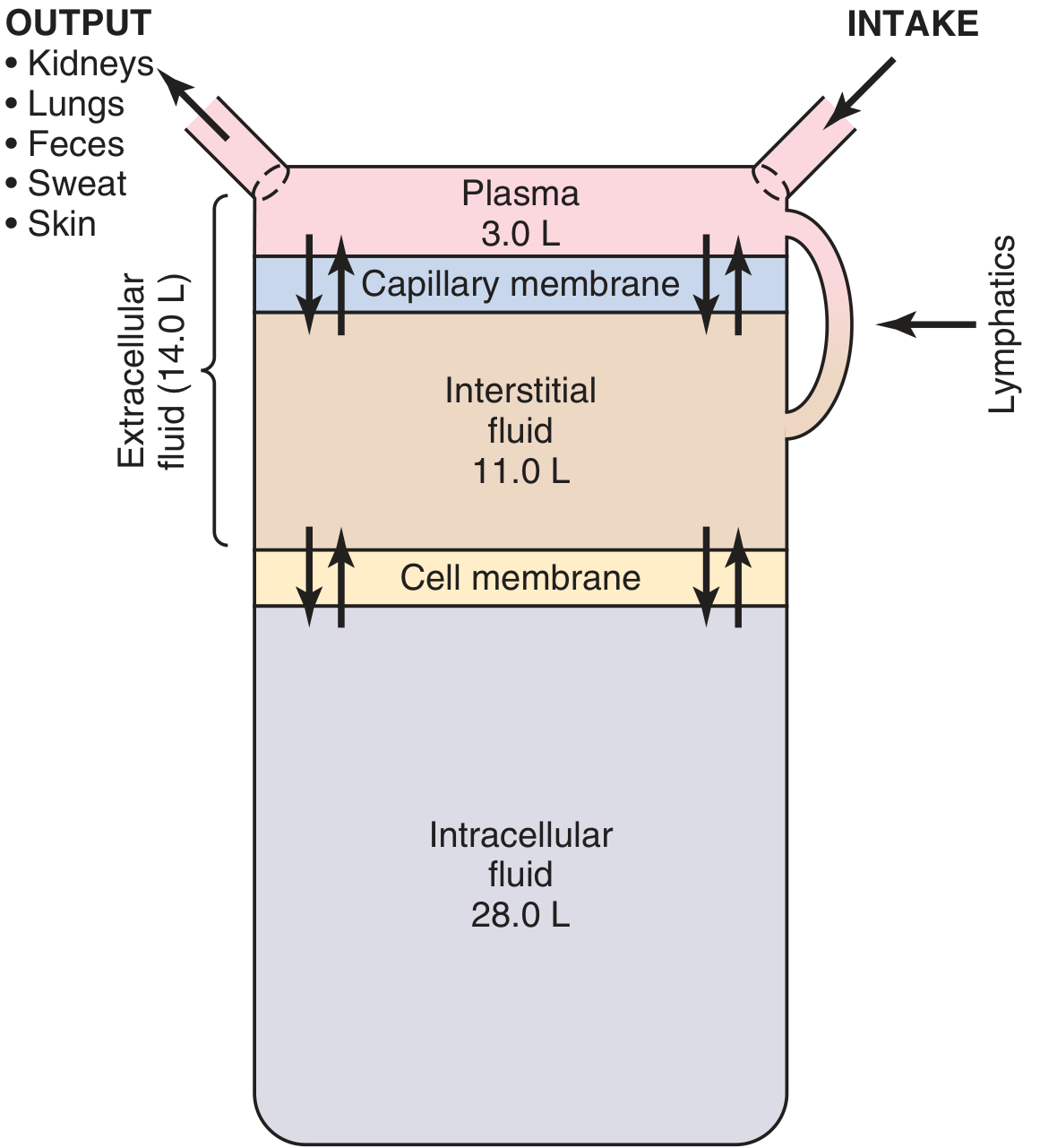
Total body water = ~60% of body weight = 42 L in a 70-kg man
| Compartment | Volume | % of Total Body Water |
|---|---|---|
| Intracellular fluid (ICF) | 28 L | 67% |
| Extracellular fluid (ECF) | 14 L | 33% |
| - Interstitial fluid | 11 L | 26% |
| - Plasma | 3 L | 7% |
| - Transcellular fluid | 1-2 L | ~3% |
Transcellular fluid = special spaces: synovial fluid, cerebrospinal fluid, peritoneal, pericardial, intraocular fluid.
Key Composition Differences Between Compartments
| Ion | Plasma | Interstitial | Intracellular |
|---|---|---|---|
| Na+ (main ECF cation) | 142 mEq/L | 139 mEq/L | 14 mEq/L |
| K+ (main ICF cation) | 4 mEq/L | 4 mEq/L | 140 mEq/L |
| Ca2+ | 2.4 mEq/L | 1.2 mEq/L | ~0 |
| Cl- | 103 mEq/L | 108 mEq/L | 4 mEq/L |
| Protein | 16 mEq/L | 0.2 mEq/L | 54 mEq/L |
The key rule: Na+ stays outside cells; K+ stays inside cells. The Na-K ATPase pump maintains this difference, using energy (ATP) to keep pumping Na out and K in.
How the Body Regulates Fluid Volume - The Renal-Body Fluid System
This is the master long-term pressure and volume controller:
↑ Blood volume
↓
↑ Arterial pressure
↓
Kidneys excrete more Na+ and water
(Pressure diuresis + Pressure natriuresis)
↓
↓ Blood volume → pressure returns to normal
The key: A tiny rise in arterial pressure (just a few mm Hg) can DOUBLE kidney water and salt output.
This feedback loop is:
- Slow (minutes to hours to days)
- Powerful - can completely normalize pressure in the long term
- The only true infinite-gain pressure control system (unlike baroreceptors which adapt)
Hormonal Refinements to Fluid Regulation
The renal-body fluid system is refined by several hormones:
| Hormone | Trigger | Effect on Kidneys |
|---|---|---|
| Aldosterone | Low BP, low Na+, high K+ (via RAAS) | Retain Na+ (and water), excrete K+ |
| ADH (vasopressin) | High plasma osmolarity, low volume | Retain water (inserts aquaporins in collecting duct) |
| Angiotensin II | Low BP/renal perfusion | Constrict efferent arteriole, stimulate Na+ reabsorption, stimulate aldosterone |
| ANP/BNP (natriuretic peptides) | High atrial stretch (volume overload) | Excrete Na+ and water - a "pressure relief valve" |
| Sympathetic nerves | Low BP | Constrict renal vasculature, retain Na+ |
How These Systems Connect: Heart Failure + Fluid Regulation
The two chapters directly link. In heart failure:
Heart fails → CO falls → Arterial pressure falls
↓
Baroreceptors activate sympathetic system
↓
RAAS activated (renin → Ang II → aldosterone)
↓
ADH secreted (low pressure, low sodium delivery to hypothalamus)
↓
Kidneys retain massive Na+ and water
↓
Blood volume rises → Venous pressures rise
↓
Body tries to restore cardiac output
BUT if heart is too damaged → Decompensation → Edema → Death
This is why understanding body fluid regulation is essential for understanding heart failure - the two chapters are really one story about the heart-kidney axis.
Measuring Body Fluid Compartments
| Compartment | Substance Used (Indicator-Dilution) |
|---|---|
| Total body water | Deuterium (heavy water) or antipyrine |
| ECF volume | Radioactive sulfate, inulin |
| Plasma volume | Radioactive iodine-labeled albumin or Evans blue dye |
| ICF volume | Calculated: Total body water - ECF |
| Interstitial volume | Calculated: ECF - Plasma volume |
Principle: Inject a known amount of a marker that distributes only in the compartment you want to measure. Measure concentration at equilibrium. Volume = Amount / Concentration.
Quick Summary Chart
| Topic | Key Numbers/Concepts |
|---|---|
| Normal cardiac output | 5 L/min |
| Critical CO for renal fluid balance | 5 L/min |
| CO immediately after severe MI | ~2 L/min |
| Sympathetic compensation of CO | Doubles the depressed output |
| Mean systemic filling pressure (normal) | 7 mm Hg |
| Mean systemic filling pressure (CHF) | 12-14 mm Hg |
| Total body water (70-kg man) | 42 L (60% of body weight) |
| ICF | 28 L (40% of body weight) |
| ECF | 14 L (20% of body weight) |
| Plasma | 3 L |
| Interstitial fluid | 11 L |
| Pressure diuresis effect | +few mm Hg → 2x urine output |
The "Story" in One Paragraph
The heart pumps blood. When it fails, less blood reaches the kidneys. The kidneys, fooled into thinking the body is dehydrated, activate the RAAS system (renin→angiotensin→aldosterone), retain sodium and water, and expand blood volume. This helps initially - the extra volume pushes more blood back to the failing heart, raising cardiac output back toward normal. But if the heart is too damaged to pump enough (below 5 L/min), the kidneys keep retaining fluid endlessly, the heart gets over-filled and over-stretched, pulmonary pressure skyrockets causing breathlessness, and the body fills with edema. This is the story of cardiac failure and body fluid regulation - told across two chapters of Guyton & Hall, but really one unified physiological narrative about what happens when the heart-kidney axis breaks down.
This is a shared conversation. Sign in to Orris to start your own chat.