Anatomical sites involved in obstructive sleep apnea. Ms ent university exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Searching the Web
obstructive sleep apnea anatomical sites ENT MS exam answer 20 marks
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from Cummings Otolaryngology (the definitive ENT reference). I have everything needed to write a detailed 20-mark MS ENT university exam answer. Let me compose it now.
Anatomical Sites Involved in Obstructive Sleep Apnea (OSA)
MS ENT University Examination - 20 Marks
INTRODUCTION (2 marks)
Obstructive sleep apnea (OSA) is defined by the presence of 5 or more predominantly obstructive respiratory events (apneas, hypopneas, or respiratory effort-related arousals - RERAs) per hour of sleep associated with symptoms or comorbidities, or 15 or more events per hour regardless of symptoms.
The fundamental mechanism is pharyngeal airway collapse during sleep caused by a combination of anatomical compromise and neuromuscular failure. Obstruction can occur at single or multiple levels simultaneously - a concept of cardinal importance for surgical planning.
PATHOPHYSIOLOGY - FOUR KEY PHENOTYPES (2 marks)
Four physiological impairments interact to produce OSA (Cummings Otolaryngology):
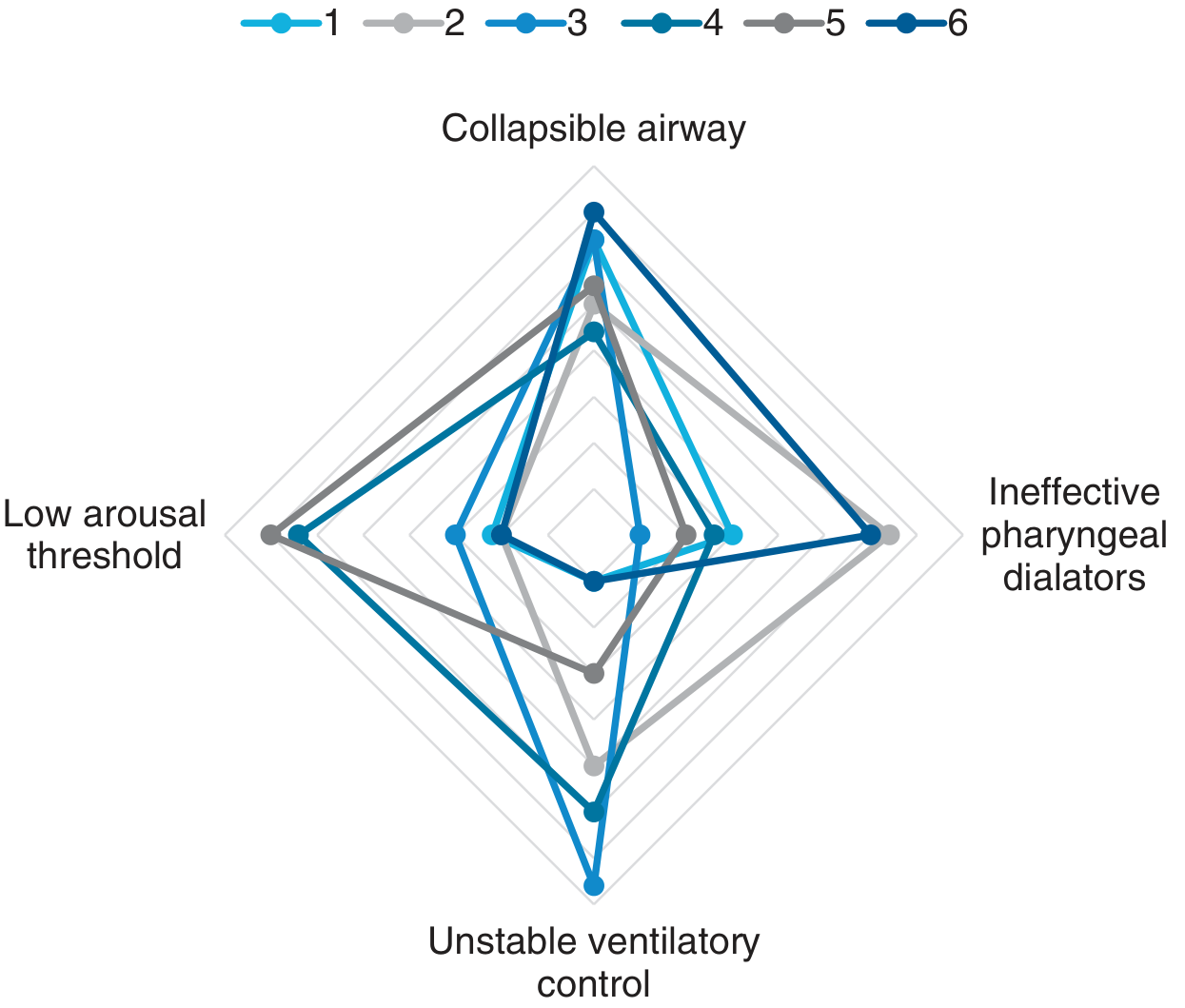
- Impaired upper airway anatomy - narrow or collapsible airway (present in ALL OSA patients)
- Inadequate responsiveness of upper airway dilator muscles during sleep
- Low respiratory arousal threshold - waking too easily before deep-sleep dilator recruitment
- Unstable/high loop gain - oversensitive respiratory control causing airway collapse from excessive negative pressure
FUJITA CLASSIFICATION OF OBSTRUCTION SITES (2 marks)
Fujita's classification remains the cornerstone of anatomical localization in OSA:
| Type | Site of Obstruction | Prevalence in OSA |
|---|---|---|
| Type I | Retropalatal region only | Common |
| Type II | Both retropalatal AND retrolingual | Most common pattern |
| Type III | Retrolingual region only | Less common |
Studies confirm retropalatal obstruction in 100% and retrolingual obstruction in 77% of OSA patients (vs. 70% and 40% respectively in simple snorers).
ANATOMICAL SITES OF OBSTRUCTION (12 marks)
1. NOSE AND NASOPHARYNX
Structures involved:
- Deviated nasal septum
- Inferior turbinate hypertrophy
- Nasal polyps
- Adenoid hypertrophy (nasopharynx)
Mechanism: Nasal obstruction increases airway resistance, promotes mouth breathing during sleep, which:
- Increases upper airway collapsibility
- Decreases efficacy of pharyngeal dilator muscles
- Worsens snoring and apnea
Important caveat: Nasal obstruction is rarely the sole cause of OSA. Treatment of nasal obstruction alone rarely cures OSA but may reduce CPAP pressures required. Adenoid hypertrophy is a major contributor in the nasopharynx, especially in children.
2. OROPHARYNX - RETROPALATAL REGION (Velopharynx)
This is the most consistently involved site in OSA.
Structures involved:
- Soft palate and uvula - elongated, thickened, or redundant soft palate narrows the retropalatal space
- Palatine tonsils - tonsillar hypertrophy is the major cause of OSA in children and a significant contributor in adults (OR 1.88 for tonsil grade >2 on meta-analysis)
- Lateral pharyngeal walls - excess parapharyngeal fat deposition
- Mallampati grade - modified Mallampati score >2 (OR 2.23) strongly associated with OSA
Critical anatomy: The retropalatal airspace is bounded anteriorly by the soft palate/uvula, laterally by the palatine tonsils and lateral pharyngeal wall fat pads, and posteriorly by the posterior pharyngeal wall. All of these can contribute to narrowing.
3. HYPOPHARYNX - RETROLINGUAL REGION (Base of Tongue)
Structures involved:
- Tongue base (posterior tongue/lingual tonsil) - macroglossia (OR 2.44) or relative macroglossia in a small mandible
- Lingual tonsils - often underdiagnosed; important surgical target (TORS lingual tonsillectomy)
- Epiglottis - epiglottic collapse is an increasingly recognized obstruction pattern
Mechanism: During sleep, the genioglossus (the most important dilator muscle) loses tone, allowing the tongue base to fall posteriorly against the posterior pharyngeal wall, obliterating the retrolingual airspace. In awake OSA patients, elevated genioglossal activity compensates - but this compensation fails during sleep.
4. LARYNGOPHARYNX / LARYNX
Though less common, laryngeal-level obstruction occurs in:
- Bilateral vocal cord/laryngeal paralysis
- Laryngomalacia (especially in children)
- Obstructing laryngeal lesions
- Epiglottic collapse (posterior tipping of epiglottis during inspiration)
This site is identified by drug-induced sleep endoscopy (DISE/SNE) and is surgically addressable (epiglottectomy, epiglottopexy).
5. CRANIOFACIAL SKELETON
Bony structural abnormalities reduce airway caliber and increase soft tissue crowding:
| Craniofacial Feature | Effect on Airway |
|---|---|
| Retrognathia (small mandible) | Displaces tongue base posteriorly; OR 3.99 for pharyngeal grade >2 |
| Decreased maxillary projection | Reduces nasopharyngeal dimensions |
| Increased hyoid-to-mandibular plane distance | Positions tongue base inferoposteriorly |
| Increased vertical facial length | Promotes mouth breathing |
| Posterior rotation of mandibular growth | Crowded posterior airway |
Retrognathia and micrognathia are central to OSA in conditions like Pierre Robin sequence, Treacher Collins syndrome, and Down syndrome.
6. NECK AND PARAPHARYNGEAL SOFT TISSUES
- Parapharyngeal fat pads - obesity leads to excess fat deposition in the lateral pharyngeal walls, compressing the airway lumen from outside
- Neck circumference - >40 cm in women, >43 cm in men is a clinical predictor of OSA severity
- Submental/chin fat - contributes to increased critical closing pressure (Pcrit)
Pcrit concept: The passive critical closing pressure determines pharyngeal collapsibility. OSA patients have Pcrit above atmospheric pressure (positive Pcrit), meaning the pharynx collapses even without negative intraluminal pressure. Normal individuals have Pcrit below -5 cm H2O.
DYNAMIC ASSESSMENT OF SITES - DRUG-INDUCED SLEEP ENDOSCOPY (DISE) (1 mark)
Because awake endoscopy misses dynamic collapse patterns, DISE/sedation nasendoscopy (SNE) with propofol is the gold standard for identifying the site and pattern of obstruction:
- VOTE classification: Velum (palate), Oropharynx (lateral walls), Tongue base, Epiglottis
- Multi-channel pressure catheters measure pressure at nasopharynx, oropharynx, hypopharynx, and esophagus simultaneously
- This guides multilevel surgery - operating on all obstructing sites in the same sitting
MULTILEVEL OBSTRUCTION AND SURGICAL IMPLICATIONS (1 mark)
The majority of OSA patients have multilevel obstruction (Fujita Type II). This has direct therapeutic implications:
- Isolated nasal surgery - rarely curative but improves CPAP tolerance
- Uvulopalatopharyngoplasty (UPPP) - addresses retropalatal level
- Tongue base reduction / TORS lingual tonsillectomy - retrolingual level
- Genioglossal advancement / hyoid myotomy - hypopharyngeal level
- Maxillomandibular advancement (MMA) - addresses all levels simultaneously by expanding the entire skeletal framework; highest success rate among surgical procedures
SUMMARY TABLE (marks consolidation)
| Level | Key Structures | Common Pathology |
|---|---|---|
| Nasal | Septum, turbinates, polyps | DNS, hypertrophy |
| Nasopharynx | Adenoids | Hypertrophy (mainly children) |
| Velopharynx (retropalatal) | Soft palate, uvula, palatine tonsils, lateral walls | Elongated palate, tonsillar hypertrophy |
| Hypopharynx (retrolingual) | Tongue base, lingual tonsils | Macroglossia, lingual tonsillar hypertrophy |
| Larynx | Epiglottis, vocal cords | Epiglottic collapse, laryngomalacia |
| Skeletal | Mandible, maxilla, hyoid | Retrognathia, micrognathia |
| Soft tissue/Neck | Parapharyngeal fat | Obesity, large neck circumference |
CONCLUSION
OSA is a multi-level, multi-factorial disorder. The three principal anatomical levels are nose, retropalatal region, and hypopharynx, with craniofacial skeleton and soft tissue bulk providing the structural substrate. The genioglossus is the key neuromuscular guardian of airway patency. Clinical management must address all contributing anatomical levels - confirmed by DISE - to achieve durable surgical success.
Source: Cummings Otolaryngology Head and Neck Surgery, 7th edition; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Marking Scheme Suggestion:
- Introduction + definition of OSA: 2 marks
- Pathophysiology / four phenotypes: 2 marks
- Fujita classification: 2 marks
- Detailed anatomical sites (nose, retropalatal, retrolingual, larynx, craniofacial, soft tissue - 2 marks each for 6 sites): 12 marks
- DISE + surgical implications: 1 mark
- Conclusion / summary: 1 mark
- Total: 20 marks
This is a shared conversation. Sign in to Orris to start your own chat.