Ureteric colic
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ureteric colic" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Here is a complete, structured answer:
Ureteric Colic
Definition and Pathophysiology
Ureteric colic is the acute pain syndrome that results when a calculus passes from the renal pelvis into the ureter, causing partial or complete ureteric obstruction. Despite the name "colic," the pain does not fully remit - it waxes and wanes rather than disappearing between episodes. The most common stones responsible are small 3-5 mm calculi, and they most frequently lodge at the three points of natural ureteric narrowing:
- Pelviureteric junction (PUJ)
- Pelvic brim (where the ureter crosses the iliac vessels)
- Vesicoureteric junction (VUJ) - the most common site
- National Kidney Foundation Primer on Kidney Diseases, 8e, p.470
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Clinical Features
Pain pattern (varies by stone location):
- Upper ureter / PUJ - severe loin pain radiating to the ipsilateral iliac fossa, testis (men), or labium majus (women); nausea and reflex vomiting are common
- Lower ureter crossing pelvic brim - can mimic appendicitis (right) or diverticulitis (left)
- VUJ - urinary frequency, urgency, and dysuria mimicking acute cystitis
- General: the patient is typically in obvious pain and cannot find a comfortable position (unlike peritonitis, where patients lie still)
Examination: Ipsilateral costovertebral angle (renal angle) tenderness; bowel sounds may be absent due to reflex paralytic ileus. Importantly, peritonism is absent in uncomplicated cases.
Investigations
Urine
- Microscopic haematuria - present in the majority (but may be absent if obstruction is complete, as no urine flows through that ureter)
- Pyuria - may be sterile or due to infection
- Leukocytosis - suggests concurrent infection
- Urine culture if infection or definitive surgery is planned
- Pregnancy test in women of childbearing age (mandatory)
Blood
- Usually normal; FBC, U&E, calcium, phosphate, uric acid
- Leukocytosis may reflect stress or infection
Imaging
| Modality | Role |
|---|---|
| Non-contrast CT (NCCT) | Gold standard - detects stones ≥1 mm, including radiolucent uric acid stones; shows secondary signs (hydronephrosis, hydroureter, perinephric fat stranding); reveals alternative diagnoses |
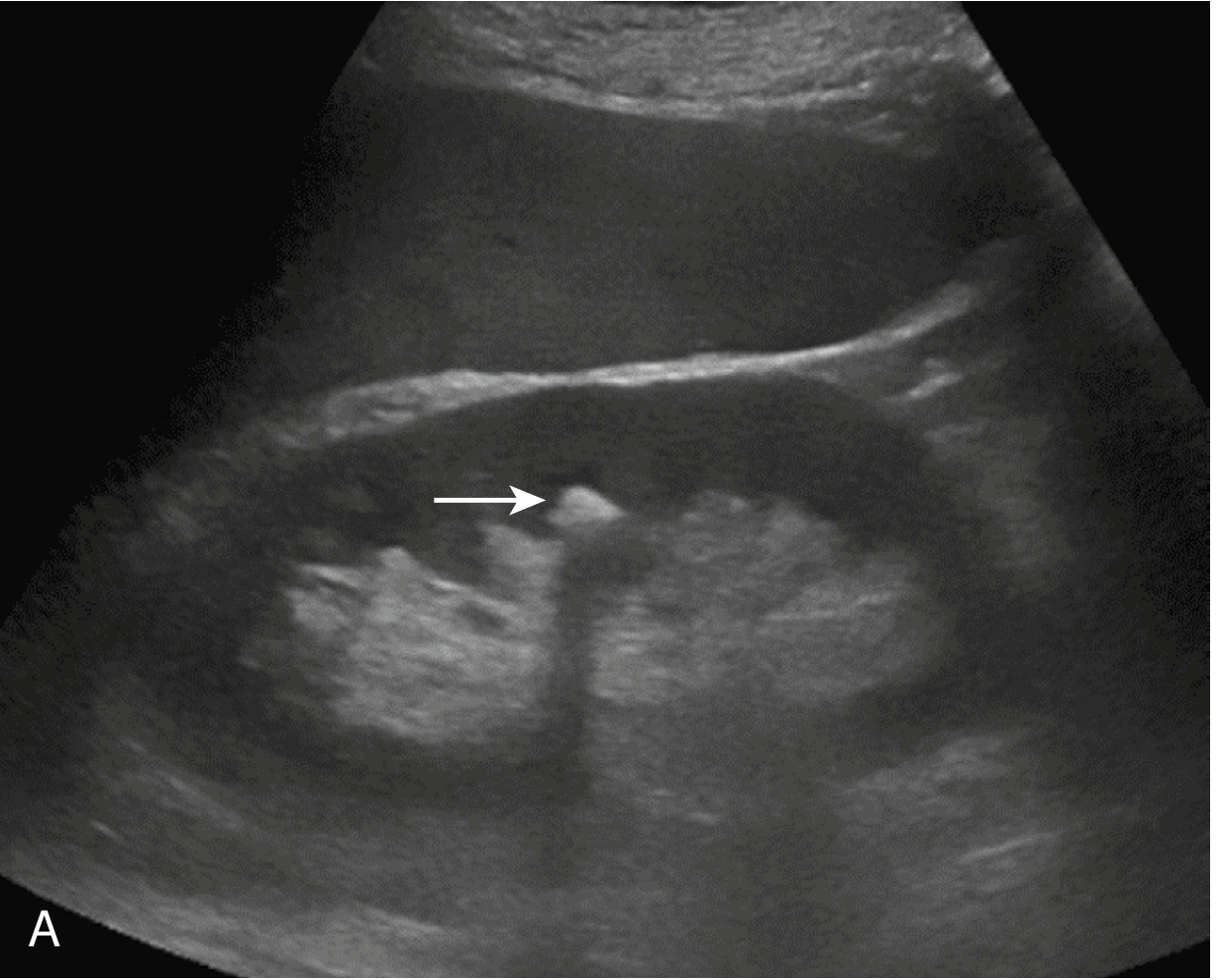
| Ultrasound | Good first-line test; shows hydronephrosis and calculi at kidney/proximal or distal ureter with echogenic foci + posterior acoustic shadowing; limited for mid-ureter (obscured by bowel gas) and small stones <5 mm |
| KUB plain film | Limited - misses radiolucent stones and stones overlying bone (e.g. sacrum); not adequate alone |
| IVU | Largely superseded; requires contrast, delayed films up to 8 hours; cannot give alternative diagnoses |
| MRI | Useful in pregnancy if ultrasound inconclusive; no radiation but expensive and slow |
Non-contrast CT has a dose of approximately 2-3 mSv with low-dose technique (comparable to a limited IVU series). It is the investigation of choice.
Ultrasound image showing kidney stone (arrow) with posterior echo shadow:
Differential Diagnosis
Urinary tract causes:
- Clot colic (anticoagulation, haemophilia, vascular tumours)
- Papillary necrosis (diabetes, NSAIDs, sickle cell disease)
Other organs:
- Acute appendicitis
- Ectopic pregnancy
- Ovarian torsion
- Abdominal aortic aneurysm (AAA) - must be excluded, especially if pulsatile abdominal mass
- Acute intestinal obstruction
- Acute cholecystitis (right PUJ stone)
- Herpes zoster
- Duodenal ulcer
- Musculoskeletal pain
Critical: AAA can mimic ureteric colic and is life-threatening. Always examine the abdomen for a pulsatile mass.
Management
Analgesia (first priority)
- NSAIDs are preferred - diclofenac sodium, indomethacin (can be given per rectum), or parenteral ketorolac. They are effective and have fewer side effects than opioids
- Paracetamol is also effective as adjunct analgesia
- Opioids (pethidine, morphine) for refractory pain
- Antispasmodics are not necessary
Hydration
- Adequate (not excessive) hydration is encouraged
Medical Expulsive Therapy (MET)
- Tamsulosin 0.4 mg once daily (alpha-1 adrenergic blocker) - causes smooth muscle relaxation of the distal ureter, facilitating stone passage
- Indicated for distal ureteric stones 5-10 mm in diameter
- Meta-analysis evidence supports its use for facilitating passage of this stone size
Conservative (Watchful Waiting)
- Up to 95% of stones ≤5 mm pass spontaneously
- Up to 90% of 4-mm stones and 50% of 6-10 mm stones pass spontaneously
- Acceptable for asymptomatic small (<5 mm), non-obstructive lower pole calculi with preserved renal function
Indications for Emergency Urinary Decompression
These are urgent - drain first, treat stone later:
- Obstruction with infection ("pus under pressure") - pyrexia, continuous loin pain, sepsis above an impacted stone - a true emergency; blood and urine cultures + broad-spectrum IV antibiotics + urgent decompression
- Complete obstruction of a solitary functioning kidney
- Bilateral complete ureteric obstruction
- Perforation of the ureter (rare)
Decompression options:
- Ureteric stenting (retrograde JJ stent)
- Percutaneous nephrostomy (PCN)
If clinically unstable, admit to critical care for initial stabilisation before urological intervention.
Surgical Indications (Non-Emergency)
| Timing | Indication |
|---|---|
| Early (prompt) | Stone >1 cm; persistent unremitting bouts of colic despite analgesia |
| Elective | Failure to pass after ~6 weeks of conservative management |
Surgical Options
- Ureteroscopy (URS) with laser lithotripsy - preferred for ureteric stones; also possible in select symptomatic patients as primary treatment even without infection
- Extracorporeal Shockwave Lithotripsy (ESWL/SWL) - non-invasive; localises stone with fluoroscopy or US; acoustic shockwaves fragment the stone. Steinstrasse ("street of stones") is a complication where stone fragments line up in the ureter
- Percutaneous nephrolithotomy (PCNL) - for large renal/upper ureteric stones
Metabolic Evaluation (After Acute Episode)
For stone recurrence prevention:
- Urine pH and crystal analysis
- Serum calcium, phosphate, uric acid - to exclude hypercalcaemia, hyperuricaemia
- Urine culture if surgery planned
- Detailed 24-hour urine metabolic workup for high-risk/recurrent stone formers
Stone composition (first-time formers):
- ~90% contain calcium (most commonly calcium oxalate)
- Others: uric acid, cystine, struvite (magnesium ammonium phosphate)
Key Points Summary
| Feature | Key Fact |
|---|---|
| Most common stone site | Vesicoureteric junction (VUJ) |
| Best imaging | Non-contrast CT KUB |
| First-line analgesia | NSAIDs (e.g. diclofenac) |
| MET drug | Tamsulosin 0.4 mg OD |
| Pass spontaneously | ~95% of ≤5 mm stones |
| Emergency indication | Obstruction + infection ("pus under pressure") |
| Emergency decompression | Ureteric stenting or PCN |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | National Kidney Foundation Primer on Kidney Diseases 8e | Pye's Surgical Handicraft 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.