Can you tell about how to decide which suture I have to give in which wound generally in blunt trauma cut accidental cut can explain in images how can I give perfect sutures tell me about types of sutures where which suture used with perfect images
Reading File
Finding Sources
Searching the Web
types of sutures wound closure techniques blunt trauma laceration repair guide images
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Searching the Web
running continuous suture mattress suture subcuticular technique images when to use
Reading File
Loading Image
Loading Image
Reading File
Searching the Web
suture selection guide body region wound type size chart scalp face hand trunk
Loading Image
Reading File
Loading Image
Searching the Web
vertical mattress suture horizontal mattress suture technique diagram comparison
Loading Image
Loading Image
Now I have all the material needed for a thorough, well-illustrated answer. Let me compile it.
Complete Guide to Suturing: Types, Techniques & When to Use Them
1. Before You Suture - Wound Assessment
The first decision is whether a wound even needs sutures. Ask yourself:
| Factor | Consider Sutures | Avoid / Delay Sutures |
|---|---|---|
| Time since injury | < 6 hours (face < 12 hrs) | > 6-8 hours (high contamination risk) |
| Wound type | Clean cut, accidental laceration | Animal/human bites, puncture wounds, high-velocity missile wounds |
| Contamination | Clean, irrigated wound | Heavily contaminated, devitalized tissue |
| Tension | Low to moderate tension | Very high tension without deep layer first |
| Location | Face, scalp, trunk, extremities | Hand/foot bites, infected wounds |
Key prep steps (from Rosen's Emergency Medicine): Irrigate heavily with tap water or 0.9% saline using high-pressure syringe (18-gauge needle + 30 mL syringe = 7-8 psi). Debride only clearly devitalized edges. Avoid povidone-iodine directly in the wound at >1% concentration.
2. Suture Materials - Absorbable vs. Non-absorbable
Absorbable Sutures (used deep / inside tissues)
| Name | Material | Absorption Time | Best Use |
|---|---|---|---|
| Vicryl (Polyglactin 910) | Braided synthetic | 56-70 days | Deep dermal, subcutaneous, fascia |
| Monocryl (Poliglecaprone) | Monofilament synthetic | 90-120 days | Subcuticular skin closure |
| PDS (Polydioxanone) | Monofilament synthetic | 180+ days | Fascia, tendons, long-term support |
| Plain Gut | Natural | 7-10 days | Oral mucosa, scalp (no removal needed) |
| Chromic Gut | Treated natural | 10-21 days | Oral/vaginal mucosa |
Non-absorbable Sutures (used on skin surface - must be removed)
| Name | Material | Properties | Best Use |
|---|---|---|---|
| Nylon (Ethilon) | Monofilament synthetic | Low reactivity, good tensile strength | Skin closure everywhere |
| Prolene (Polypropylene) | Monofilament | Least reactive, very smooth | Face, running subcuticular |
| Silk | Natural braided | Easy handling, highest reactivity | Oral sutures, eyelid (temporary) |
| Mersilene (Polyester) | Braided | High tensile strength | Cardiovascular, fascia |
3. Suture Size Chart (USP Scale)
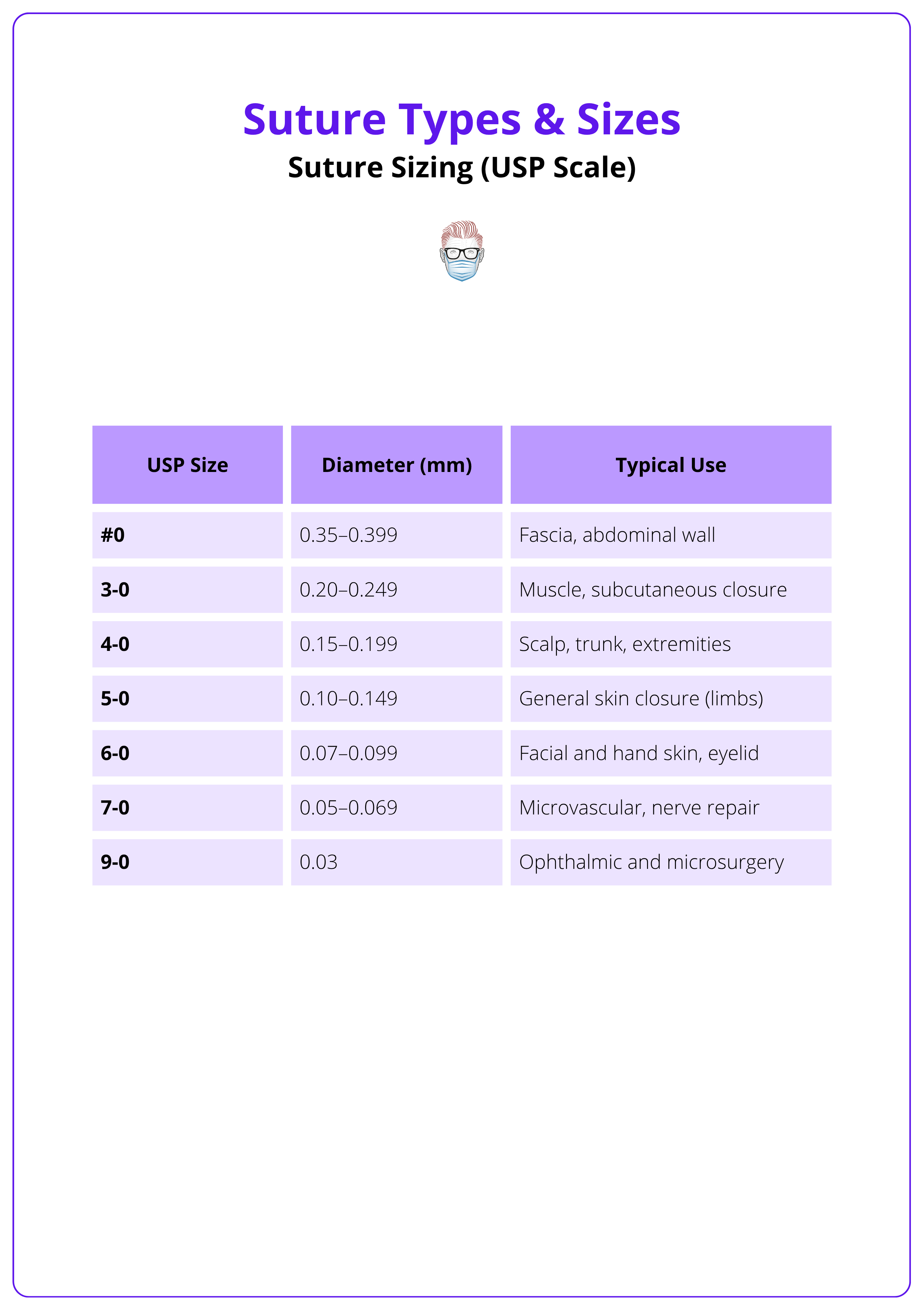
Simple rule: The larger the number, the finer/thinner the suture. Face needs fine (5-0, 6-0). Trunk/scalp needs thicker (3-0, 4-0).
4. Needle Types

- Reverse cutting (3/8 circle) - Most common for skin; the cutting edge faces outward, reducing tissue tear-through
- Conventional cutting - Edge faces inward; tends to cut toward wound; less preferred for skin
- 3/8 circle - Standard for most skin closures
- 1/2 circle - Deep, confined spaces (abdominal wall, oral cavity)
5. Types of Suture Techniques


A. Simple Interrupted Suture
The workhorse of emergency wound closure.

How to place:
- Enter needle at 90° to skin, ~5 mm from wound edge
- "Scoop" through dermis and exit equidistant on the other side
- Leave a 2-3 cm tail; tie with instrument tie (2-1-1 throws minimum)
- Place sutures ~5 mm apart along the wound
- Wound edges should be slightly everted (not flat or inverted)
When to use:
- Most standard lacerations - face, scalp, trunk, extremities
- Irregular/jagged wounds and curvilinear lacerations (interrupts distribute tension better)
- High-tension wounds (each stitch is independent; one failure doesn't open the whole wound)
- Blunt trauma cuts with irregular edges
From Rosen's: "Wound closure with simple interrupted sutures is the most common method of laceration repair in the ED and the majority of wounds can be closed with this technique."
B. Running (Continuous) Suture
One continuous thread from one end of the wound to the other.
When to use:
- Linear lacerations under minimal tension
- Longer wounds where speed matters
- Scalp lacerations
- When there is low risk of infection
Variants:
- Simple running - faster, good for scalp
- Running locked (Ford interlocking) - more hemostatic, good for bleeding wounds
- Running subcuticular - passes horizontally in the dermis; best cosmetic result, no cross-hatch marks
From Rosen's: "The running technique is appropriate for linear lacerations under minimal tension when there is a low risk of infection. Curvilinear or jagged wounds are best closed with interrupted sutures."
C. Vertical Mattress Suture

How it works: Two passes - one deep and wide (far-far), one superficial and close (near-near). Achieves maximum eversion of wound edges.
When to use:
- Wounds prone to inversion (back of hand, foot, interdigital areas)
- High-tension wounds (joints, back, shoulders)
- Wounds where skin edges tend to roll inward
- Thick skin areas
Tintinalli's Emergency Medicine notes: "Simple interrupted sutures often lead to skin inversion and risk of failure of the initial wound repair with interdigital lacerations. The more effective closure technique is to place horizontal or vertical mattress sutures."
D. Horizontal Mattress Suture
A side-to-side stitch that distributes tension across a wider area of tissue.
When to use:
- Very high-tension wounds (fasciotomy closures, scalp)
- Fragile or thin skin (elderly patients)
- Areas needing hemostasis (bleeding scalp edges)
- As retention sutures in abdominal closures
E. Corner / Half-Buried Horizontal Mattress Suture (Three-Point Stitch)
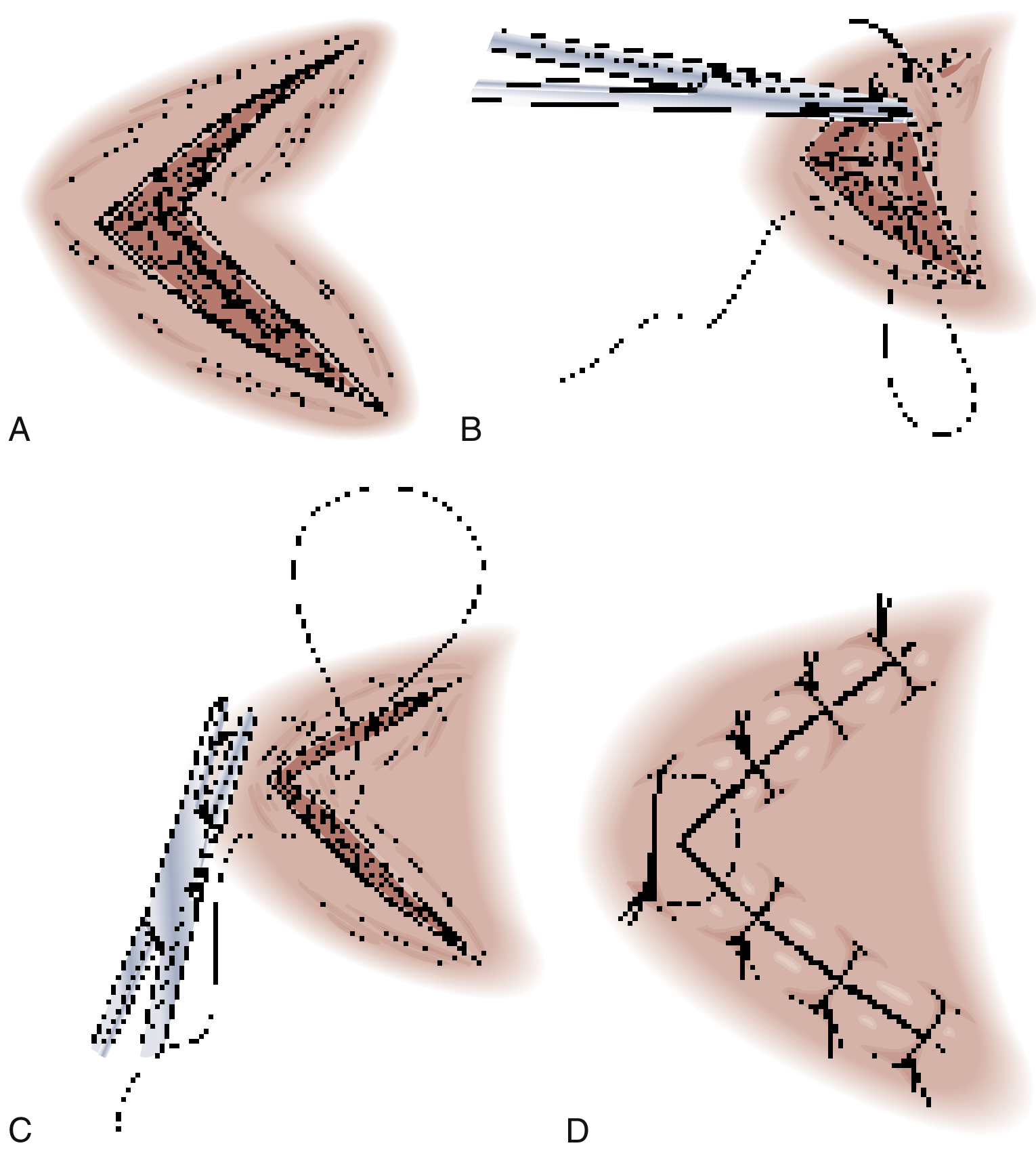
When to use:
- Flap tip closures (triangular / V-shaped lacerations)
- Stellate lacerations
- The needle never directly passes through the flap tip, so blood supply is preserved
F. Buried / Intradermal (Deep Dermal) Suture
How it works: Knot buried deep in subcutaneous tissue; suture runs through the dermis and exits at the same level. Done with absorbable suture (Vicryl, Monocryl).
When to use:
- Deep wounds to eliminate dead space
- Reducing skin tension before surface closure
- NOT in contaminated wounds (increases infection risk)
- NOT through adipose tissue alone
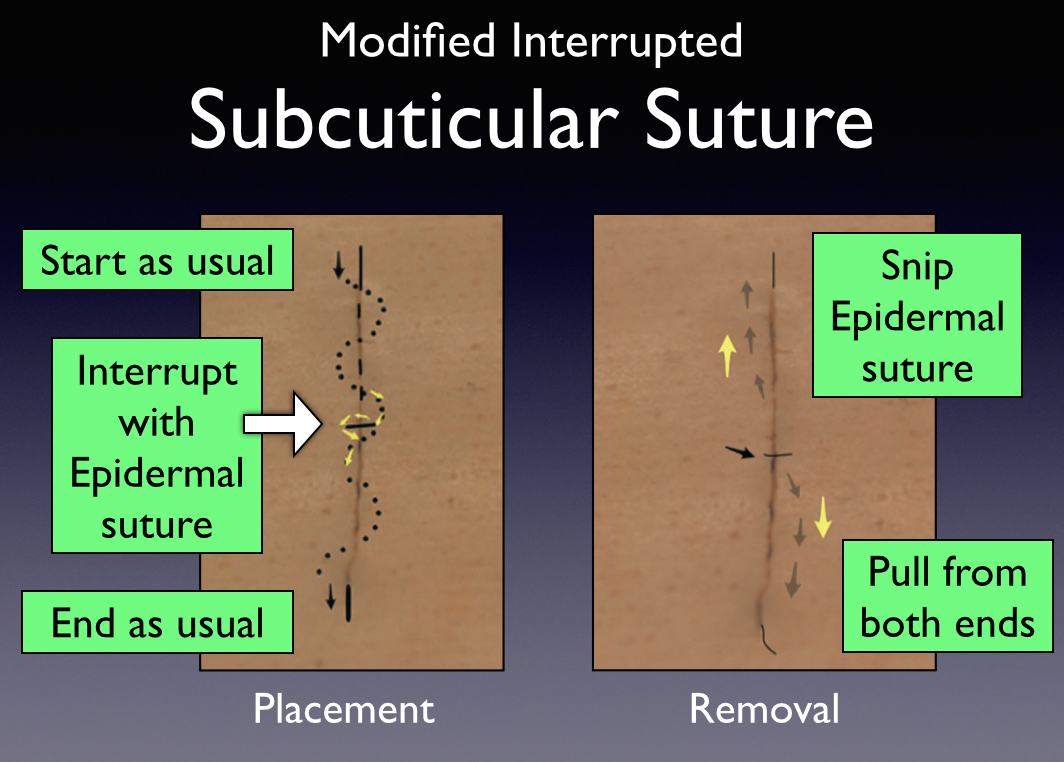
G. Subcuticular (Intradermal Running) Suture
Thread runs continuously inside the dermis parallel to the skin surface - no suture crosses the skin externally.
When to use:
- Best cosmetic result (no "railroad track" marks)
- Elective surgical wounds, facial lacerations, clean accidental cuts
- Used with absorbable (Monocryl) or removable (Prolene) suture
6. Which Suture Where - By Body Region
| Region | Material | Size | Technique | Removal |
|---|---|---|---|---|
| Scalp | Nylon / Staples | 3-0, 4-0 | Simple interrupted or running locked | 7-10 days |
| Face / forehead | Nylon or Prolene | 5-0, 6-0 | Simple interrupted or subcuticular | 3-5 days |
| Eyelid | Nylon or Silk | 6-0 | Simple interrupted | 3-5 days |
| Lip | Nylon (skin) / Vicryl (mucosa) | 4-0 / 3-0 | Interrupted; align vermillion border first | 4-5 days |
| Ear | Nylon | 6-0 | Simple interrupted | 5-7 days |
| Trunk / back | Nylon + deep Vicryl | 3-0, 4-0 | Buried deep + interrupted surface | 7-10 days |
| Extremity (arm/leg) | Nylon | 4-0 | Simple interrupted | 7-10 days |
| Hand / finger | Nylon | 4-0, 5-0 | Simple interrupted | 7-10 days |
| Foot / sole | Nylon | 3-0, 4-0 | Interrupted or mattress | 10-14 days |
| Joints (knee/elbow) | Nylon + deep Vicryl | 3-0, 4-0 | Vertical mattress + buried deep | 10-14 days |
| Oral mucosa | Plain/Chromic gut or Vicryl | 3-0, 4-0 | Interrupted; absorbable = no removal | Dissolves 7-10 days |
| Fascia | PDS or Vicryl | 0, 1 | Running or interrupted | Absorbable |
7. Blunt Trauma Cuts vs. Clean Accidental Cuts
Blunt Trauma (e.g., falling on concrete, head hit on wall)
- Wound edges are irregular, crushed, or stellate
- More contamination, more devitalized tissue
- Use: Interrupted sutures (best tension distribution), vertical mattress at high-tension areas, corner stitch for flap tips
- Irrigate more aggressively before closing
- Consider delayed primary closure if heavily contaminated
Clean Accidental Cuts (e.g., knife, glass)
- Wound edges are sharp and well-defined
- Minimal contamination
- Use: Simple interrupted or running suture; subcuticular for cosmetically sensitive areas (face)
- Can approximate edges more precisely
8. Alternative Closure Methods
- Staples - Scalp, trunk, extremities where cosmesis is less important. Fast, low infection risk. NOT for face, hands, joints.
- Tissue adhesive (Dermabond) - Short (<4 cm), low-tension, clean wounds on face. No injection needed. Not for joints or hands alone.
- Steri-strips - Very superficial, low-tension wounds; or as backup after suture removal.
Key Decision Summary
Is the wound contaminated / bite? → Do NOT close primarily
↓ No
Is it >6-8 hours old (or >12h face)? → Consider delayed closure
↓ No
Clean, sharp cut, low tension? → Running or subcuticular suture
↓
Jagged / irregular / high tension? → Interrupted sutures
↓
Skin edges inverting? (hand, foot) → Vertical mattress
↓
Triangular flap / stellate? → Corner stitch (3-point mattress)
↓
Deep wound / dead space? → Buried deep Vicryl first, then surface suture
Sources: Rosen's Emergency Medicine (9th ed.), Tintinalli's Emergency Medicine (9th ed.), Pfenninger and Fowler's Procedures for Primary Care (3rd ed.), Roberts and Hedges' Clinical Procedures in Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.