Herina surgery case all about this
Reading File
Asking for Preferences
Finding Sources
Searching the Web
hernia surgery types anatomy procedure complications surgical case
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from 5 major surgical textbooks plus two excellent anatomical images. Here is the complete surgical case guide on all types of hernia:
Hernia Surgery - Complete Surgical Case Guide
Sources: Bailey & Love's Short Practice of Surgery 28th Ed, Schwartz's Principles of Surgery 11th Ed, Maingot's Abdominal Operations, Fischer's Mastery of Surgery 8th Ed, Sabiston Textbook of Surgery
1. DEFINITION & BASIC PRINCIPLES
A hernia is a protrusion of a viscus or part of a viscus through a defect in the wall of the cavity in which it normally lies. Every hernia has two essential components:
- A defect in the abdominal wall (fascia, muscle, or both)
- Content - tissue forced outwards through that defect (omentum, bowel, fat)
The narrowest part of the sac at the wall defect is called the neck of the sac - this is what determines complication risk.
2. CLASSIFICATION OF HERNIAS
By Location
| Type | Site | Notes |
|---|---|---|
| Indirect inguinal | Lateral to inferior epigastric vessels, through deep ring | Most common overall; congenital or acquired |
| Direct inguinal | Medial to inferior epigastric vessels (Hesselbach's triangle) | Always acquired; middle-aged/elderly men |
| Femoral | Through femoral canal, below inguinal ligament | More common in women; high strangulation risk |
| Umbilical | Through umbilical ring | Common in infants; adults often acquired |
| Paraumbilical | Through linea alba near umbilicus | More common than true umbilical in adults |
| Incisional/Ventral | Through previous surgical scar | Up to 10-15% of laparotomy incisions |
| Epigastric | Through linea alba above umbilicus | Often contain extraperitoneal fat only |
| Spigelian | Through semilunar line, lateral to rectus | Rare; often occult/interparietal |
| Hiatal | Through oesophageal hiatus of diaphragm | Sliding (type I) or rolling (type II) |
| Obturator | Through obturator foramen | Rare; post-menopausal women; Howship-Romberg sign |
| Lumbar | Petit's or Grynfeltt's triangle | Very rare |
By Complexity (Clinical Classification)
| Status | Definition | Action |
|---|---|---|
| Occult | Not detectable clinically | Watchful waiting |
| Reducible | Swelling appears and disappears freely | Elective repair |
| Irreducible | Cannot return to abdominal cavity | Urgent assessment |
| Incarcerated | Irreducible + trapped; at risk of strangulation | Urgent surgery |
| Obstructed | Bowel trapped but blood supply intact | Emergency surgery |
| Strangulated | Blood supply cut off; contents ischaemic | Emergency surgery |
| Infarcted/Gangrenous | Contents gangrenous | Emergency surgery; high mortality |
3. ANATOMY (The Foundation of Safe Surgery)
The inguinal canal is approximately 4-6 cm long, oriented obliquely in the anterior pelvis:
- Anterior wall: External oblique aponeurosis
- Posterior wall: Transversalis fascia
- Roof: Conjoint tendon (fusion of internal oblique + transversus abdominis)
- Floor: Inguinal (Poupart's) ligament
Key landmarks (from Schwartz's):
- Deep (internal) inguinal ring: Defect in transversalis fascia, midway between ASIS and pubic tubercle
- Superficial (external) inguinal ring: Defect in external oblique aponeurosis
- Inferior epigastric vessels: Lie just medial to the deep ring - this is the key landmark separating direct (medial) from indirect (lateral) hernias
- Cooper's (pectineal) ligament: Fused to periosteum of pubic tubercle; used in repair
- Iliopubic tract: Aponeurotic band, forms inferior margin of internal ring
Contents of inguinal canal (male): Testicular artery, veins, lymphatics, vas deferens, and 3 nerves - ilioinguinal, iliohypogastric, and genital branch of genitofemoral nerve
Hesselbach's triangle (site of direct hernia):
- Medially: Lateral border of rectus abdominis
- Superolaterally: Inferior epigastric vessels
- Inferiorly: Inguinal ligament

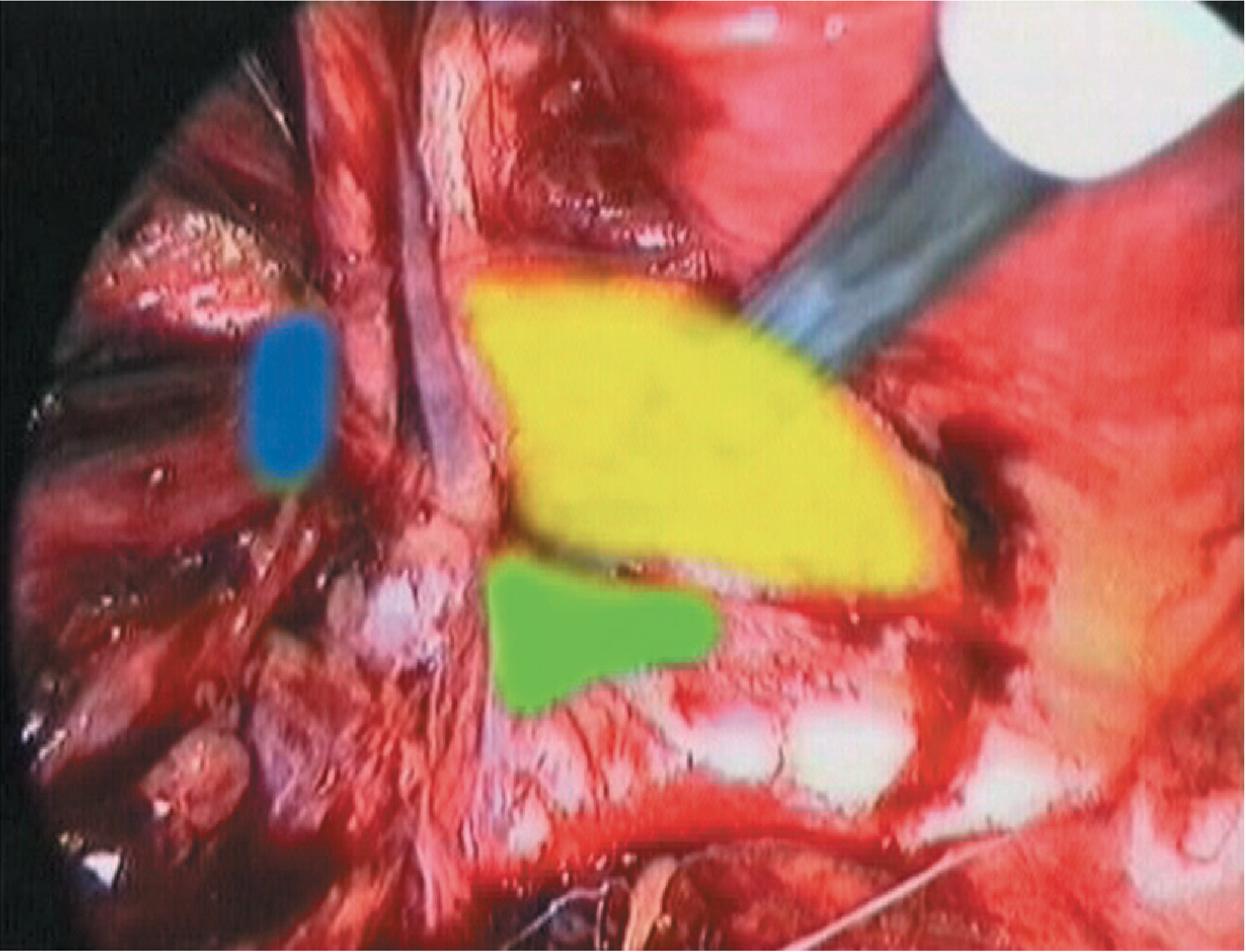
Laparoscopic "Danger Zones" (Schwartz's):
- Triangle of doom: Between the vas deferens and testicular vessels - contains the external iliac artery and vein; never staple here
- Triangle of pain: Lateral to testicular vessels - contains the femoral branch of genitofemoral nerve and lateral femoral cutaneous nerve; stapling causes chronic neuralgia
4. PATHOPHYSIOLOGY & RISK FACTORS
Indirect Inguinal Hernia
Congenital: Patent processus vaginalis (PPV) - the peritoneal tube that accompanies testicular descent fails to obliterate. Very common in premature infants and neonates.
Acquired: Muscle weakness around deep inguinal ring.
Direct Inguinal Hernia
Always acquired. Weakness of transversalis fascia in Hesselbach's triangle due to:
- Age-related collagen changes (decreased type I : type III ratio)
- Chronic raised intra-abdominal pressure
Risk Factors for All Hernias
- Chronic cough / COPD
- Constipation, straining, prostatism
- Heavy lifting, physical exertion
- Family history (8x lifetime risk if positive)
- Positive family history
- Connective tissue disorders (Ehlers-Danlos, Marfan's, osteogenesis imperfecta)
- Ascites
- Previous lower abdominal incisions
- Cigarette smoking
- Collagen synthesis defects (decreased type I collagen)
5. CLINICAL PRESENTATION & EXAMINATION
History
- Lump in groin, umbilical region, or at scar site
- Usually painless but may cause aching or heaviness
- Sharp, intermittent pain = tissue pinching at neck (urgent concern)
- Severe pain = possible strangulation (EMERGENCY)
- Ask: Does it reduce spontaneously? Bowel obstruction symptoms?
Examination Steps
- Examine supine first, then standing (hernias enlarge on standing)
- Ask patient to cough or perform Valsalva to demonstrate hernia
- Check for expansile cough impulse (absent if neck is tight = irreducible/femoral)
- Attempt to reduce the hernia
- Check if hernia is controlled by pressure at deep inguinal ring:
- Controlled = indirect/lateral
- Not controlled = direct/medial
- ALWAYS examine the opposite side - occult contralateral hernias present in up to 20% of patients
Red Flags
- Overlying skin cellulitis = strangulating hernia; treat as emergency
- Absent cough impulse in firm groin swelling = likely femoral hernia (often misdiagnosed as lymph node)
- No upper limit to scrotal swelling = large inguinal hernia, not a hydrocele
Investigations
- Most cases: Clinical diagnosis only, no investigations needed
- Uncertainty: Ultrasound (first-line), CT scan
- Emergency/bowel obstruction: Plain erect AXR + CT (detects obstructing hernia; excludes malignancy)
6. INDIRECT vs. DIRECT INGUINAL HERNIA - COMPARISON
| Feature | Indirect | Direct |
|---|---|---|
| Relation to inferior epigastric vessels | Lateral (exits through deep ring) | Medial (through Hesselbach's triangle) |
| Aetiology | Congenital (PPV) or acquired | Always acquired |
| Age | Any age; common in young males | Middle-aged/elderly |
| Sex | M >> F | M only |
| Path | Through deep ring → along canal → can reach scrotum | Pushes straight through posterior wall |
| Strangulation risk | Higher (narrower neck) | Lower (wide-necked) |
| Controlled by deep ring pressure? | Yes | No |
7. SURGICAL REPAIR - OPTIONS AND TECHNIQUES
Operations for Inguinal Hernia (Bailey & Love)
A. Open Suture Repairs (Tissue Repairs - no mesh)
Used when mesh is contraindicated (contaminated field, infection)
- Herniotomy only: Ligation of sac at deep ring; for children/young adults with indirect hernia
- Bassini repair: Suture of conjoint tendon to inguinal ligament behind spermatic cord
- Shouldice repair: 4-layer imbrication of transversalis fascia + conjoint tendon; best tissue repair, <1% recurrence at expert centres
- Desarda repair: Uses a strip of external oblique for reinforcement (tissue)
- Maloney darn: Lattice of sutures across the posterior wall
B. Open Mesh Repairs (GOLD STANDARD for elective cases)
- Lichtenstein "tension-free" repair: Flat polypropylene mesh placed onlay over posterior wall of inguinal canal, secured with sutures. Mesh wraps around spermatic cord. Simple, reproducible, low recurrence (<5%), local anaesthesia possible. Most widely performed worldwide.
- Mesh plugs and hernia systems: No longer recommended (higher chronic pain rates)
C. Open Preperitoneal Repairs
- Stoppa repair: Large bilateral mesh placed in preperitoneal space via midline incision; for recurrent or bilateral hernias
- Transinguinal preperitoneal (TIPP)
D. Laparoscopic / Robot-Assisted Repairs
| Technique | Approach | Notes |
|---|---|---|
| TEP (Totally Extraperitoneal) | Extraperitoneal dissection; peritoneum never entered | Preferred; faster recovery; no bowel risk |
| TAPP (Transabdominal Preperitoneal) | Transperitoneal; mesh placed in preperitoneal space | Better visualisation of anatomy; bilat. repair easier |
| Robotic | Robotic-assisted TEP or TAPP | Better ergonomics/visualisation; rapidly being adopted |
Laparoscopic vs. Open:
- Laparoscopic: Less postoperative pain, faster return to activity, better for bilateral and recurrent hernias, longer learning curve
- Open (Lichtenstein): Simpler, can be done under local anaesthesia, shorter learning curve
- Recurrence rates are equivalent between mesh repairs (open vs. laparoscopic) when properly performed
Operations for Femoral Hernia
Three open approaches + laparoscopic:
- Low approach (Lockwood): Through groin, simple, local anaesthesia; not if bowel resection needed
- High approach (McEvedy): Vertical incision, via preperitoneal route; allows bowel resection; preferred for emergency/strangulation
- Inguinal approach (Lotheissen): Through inguinal canal floor; rarely used now
- Laparoscopic (TEP/TAPP): Suitable for elective cases
Operations for Other Hernia Types
Umbilical/paraumbilical hernia:
- Small defects (<3 cm): Mayo repair (overlapping fascia, "vest over pants")
- Larger defects: Mesh repair (onlay or sublay); lower recurrence
- Children: Observe until age 3-4 (80% close spontaneously); operate if persistent
Incisional/Ventral hernia:
- Primary closure: Only for very small defects
- Open mesh repair (component separation for large defects): Sublay (retrorectus) placement preferred
- Laparoscopic IPOM (intraperitoneal onlay mesh): Requires anti-adhesion mesh
- Robotic retromuscular repair: Gaining popularity
Hiatal hernia:
- Sliding (type I): Medical management (PPIs); surgery (laparoscopic Nissen fundoplication) if refractory GORD
- Rolling/paraesophageal (type II/III): Surgical repair due to risk of gastric volvulus; laparoscopic with mesh hiatoplasty
8. EMERGENCY HERNIA SURGERY
About 5% of inguinal hernias present as emergency (strangulation/obstruction). Key principles:
- Time is critical when bowel ischaemia is suspected
- Open or laparoscopic depending on surgeon skill and local facilities
- ~20% require bowel resection - may need conversion to midline laparotomy
- Mesh can still be used in most cases if covered by prophylactic antibiotics, unless there is gross contamination/frank perforation
- Femoral hernias: ALL should be repaired urgently (no such thing as a "watchful waiting" approach - femoral hernias strangulate easily due to rigid, bony canal walls)
9. COMPLICATIONS OF HERNIA SURGERY
Immediate (within 24 hours)
- Haematoma/bleeding: From subcutaneous vessels or, rarely, inferior epigastric/iliac vessels
- Urinary retention: Common in elderly males; may need catheterisation
- Femoral nerve block: From local anaesthetic spread; resolves spontaneously
Early (1st week)
- Pain, bruising, swelling: Expected
- Seroma formation: Fluid collection at dissection site; common after laparoscopic repair (may mimic early recurrence); usually resolves spontaneously; aspirate if large/symptomatic
- Wound infection: Less common with modern technique
Late (weeks to years)
- Recurrence: Main benchmark of quality - good centres aim for <5% at 5 years; mesh repairs have lower recurrence than suture repairs
- Chronic groin pain (inguinodynia): Up to 10-12% report chronic pain; caused by nerve entrapment (ilioinguinal, iliohypogastric, genitofemoral); managed by physiotherapy, nerve blocks, or neurectomy
- Testicular complications: Ischaemic orchitis (0.5%) → testicular atrophy; injury to vas deferens (rare)
- Mesh complications: Infection, migration, contraction, fistula formation (uncommon with modern lightweight meshes)
- Visceral injury: Bladder (direct hernia sac), bowel (laparoscopic), ureter
10. SPECIAL/RARE HERNIAS
| Hernia | Eponym/Sign | Key Feature |
|---|---|---|
| Richter's hernia | - | Only the antimesenteric wall of bowel is caught in the sac; no bowel obstruction but gangrenous knuckle |
| Maydl's hernia | "W" hernia | Two loops of bowel in sac with a loop inside abdomen; that central loop strangulates first |
| Littre's hernia | - | Meckel's diverticulum in the sac |
| Sliding hernia | - | Part of sac wall is formed by a viscus (e.g., sigmoid colon, bladder, caecum) |
| Obturator hernia | Howship-Romberg sign (inner thigh pain with extension) | Post-menopausal thin women; often presents with small bowel obstruction |
| Spigelian hernia | - | Through semilunar line; interparietal; occult on examination |
| Pantaloon hernia | - | Combined direct + indirect hernia on same side, straddling inferior epigastric vessels |
11. HERNIA IN SPECIAL POPULATIONS
Children:
- Inguinal hernias are almost always indirect (congenital PPV)
- Herniotomy alone (sac ligation) without repair of posterior wall is sufficient
- Contralateral exploration is controversial but considered in very young/premature infants
Women:
- Indirect inguinal hernias still occur but femoral hernias are proportionally much more common
- Round ligament is at risk during repair
Elderly/High-risk:
- Watchful waiting is acceptable for asymptomatic inguinal hernias in men (AHS/EHS guidelines)
- Local anaesthesia for Lichtenstein repair is excellent for high-risk patients
- Femoral hernias should NEVER be managed conservatively
Recurrent hernias:
- Approach the repair from the opposite side to previous surgery (anterior recurrence → posterior/laparoscopic approach, and vice versa)
- Consider Stoppa repair for multiple recurrences
Summary: Key Surgical Mnemonics
INDIRECT vs DIRECT:
- Indirect = "I" goes In through deep ring (Lateral)
- Direct = "D" goes Directly through weak posterior wall (Medial)
Femoral canal boundaries (MIVELs):
- Medially: Lacunar ligament
- Anteriorly: Inguinal ligament
- Laterally: Femoral vein
- Posteriorly: Pectineal (Cooper's) ligament
Femoral hernia DDx (at groin below inguinal ligament):
Inguinal hernia / Lymph node / Saphena varix / Femoral artery aneurysm / Psoas abscess / Adductor longus haematoma
Bailey and Love's Short Practice of Surgery 28th Ed (pp. 1087-1095) | Schwartz's Principles of Surgery 11th Ed (p. 1631-1645) | Maingot's Abdominal Operations | Fischer's Mastery of Surgery 8th Ed
This is a shared conversation. Sign in to Orris to start your own chat.