Cbc report for virus infect
Reading File
Finding Sources
Finding Sources
Searching the Web
CBC findings viral infection leukopenia lymphocytosis atypical lymphocytes
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough breakdown of CBC findings in viral infections, sourced from authoritative medical textbooks.
CBC (Complete Blood Count) in Viral Infection
Overview
Viral infections produce a distinct CBC pattern that differs markedly from bacterial infections. The key hallmarks are a low-to-normal total WBC count with a shift toward lymphocytes, and the appearance of atypical (reactive) lymphocytes on the peripheral smear.
1. White Blood Cell (WBC) Count
| Finding | Detail |
|---|---|
| Total WBC | Usually low (leukopenia) or normal (4,000-11,000/µL) |
| Neutrophils | Relatively decreased (relative neutropenia) |
| Lymphocytes | Increased (lymphocytosis) |
In rubella and many other viral illnesses, the CBC "usually shows leukopenia with relative neutropenia" - Fitzpatrick's Dermatology.
In gastroenteritis and GI viral illness, the CBC "may reveal leukopenia from a viral [cause]" - Yamada's Textbook of Gastroenterology.
2. Lymphocytes - The Key Finding
Lymphocytosis
- Lymphocytes typically >50% of the differential in viral infections like infectious mononucleosis (EBV)
- Absolute lymphocyte count is elevated
Atypical (Reactive) Lymphocytes
These are the hallmark of viral infection on peripheral smear.
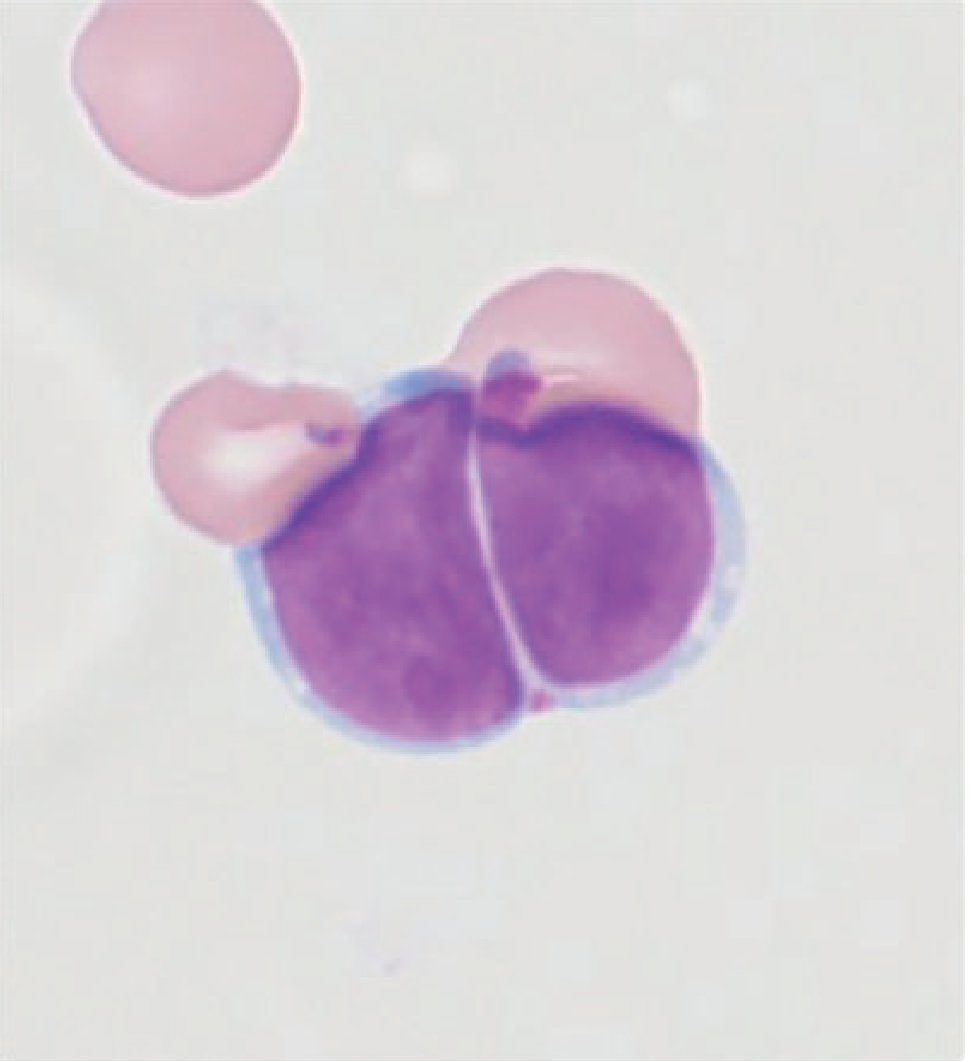
Reactive lymphocyte (Downey type) - note the large, deeply purple nucleus with irregular contour, and pale blue abundant cytoplasm that wraps around neighboring RBCs
Morphology types (Downey classification):
| Type | Description | Appearance |
|---|---|---|
| Downey Type I | Small, irregular, indented nucleus | Monocytoid |
| Downey Type II | Large, abundant gray-blue cytoplasm; cytoplasm abuts RBCs with basophilic margin | Most common in EBV |
| Downey Type III (Immunoblast) | Dispersed chromatin, prominent nucleoli, deeply basophilic cytoplasm | Seen in severe infection |
These reactive lymphocytes are CD8+ cytotoxic T cells responding to viral antigens. They are found in:
- EBV (Infectious Mononucleosis) - most classic association; >10% atypical lymphocytes
- CMV (Cytomegalovirus)
- HIV (acute infection)
- Viral hepatitis (Hep A, B, C)
- Rubella
- SARS-CoV-2 (COVID-19) - immunoblastosis reported
- Hantavirus cardiopulmonary syndrome
- Dengue
(Tietz Textbook of Laboratory Medicine; Tintinalli's Emergency Medicine)
3. Red Blood Cells (RBC) / Hemoglobin
- Usually normal in uncomplicated viral illness
- Can show mild anemia if:
- Hemolytic anemia (EBV-related immune hemolysis)
- Bone marrow suppression (HIV, parvovirus B19)
- Parvovirus B19 specifically causes pure red cell aplasia (very low reticulocytes)
4. Platelets
- Usually normal
- Thrombocytopenia can occur in:
- Dengue - often profound (can drop <100,000/µL or even <20,000)
- EBV - mild thrombocytopenia common
- HIV
- CMV
- Congenital rubella - thrombocytopenia is a neonatal feature
- Measles, chickenpox (VZV)
5. Summary Table: Viral vs. Bacterial CBC
| Parameter | Viral Infection | Bacterial Infection |
|---|---|---|
| Total WBC | Low or normal | High (leukocytosis) |
| Neutrophils | Low or normal | High (neutrophilia) |
| Band forms (left shift) | Absent | Often present |
| Lymphocytes | High (lymphocytosis) | Normal or low |
| Atypical lymphocytes | Present | Absent |
| ESR/CRP | Mildly elevated | Markedly elevated |
| Platelets | Usually normal | Usually normal |
6. Specific Viral Infections and their CBC Profiles
| Virus | WBC | Lymphocytes | Other |
|---|---|---|---|
| EBV (Mono) | Normal/low | >50%, atypical | Thrombocytopenia possible |
| CMV | Normal/low | Atypical lymphs | Mild anemia |
| HIV (acute) | Low | CD4 falls; atypical lymphs | Thrombocytopenia |
| Dengue | Leukopenia | Lymphocytosis | Severe thrombocytopenia |
| Rubella | Leukopenia | Relative lymphocytosis, plasma cells | - |
| Hepatitis (viral) | Normal/low | Atypical lymphs | Elevated LFTs |
| COVID-19 | Normal/low | Lymphopenia (severe disease) | Neutrophilia in severe cases |
| Parvovirus B19 | Normal | Normal | Reticulocytopenia, anemia |
Note on COVID-19: Interestingly, lymphopenia (low lymphocytes) rather than lymphocytosis correlates with severe COVID-19 disease and is a marker of poor prognosis - the reverse of most other viral infections.
Clinical Pearl
A peripheral blood smear showing >10% atypical lymphocytes combined with leukopenia in a young patient with fever, sore throat, and lymphadenopathy is highly suggestive of infectious mononucleosis (EBV). Confirm with a monospot test (heterophile antibody) - Tintinalli's Emergency Medicine, p. 1071.
Sources: Tintinalli's Emergency Medicine; Fitzpatrick's Dermatology 5e; Tietz Textbook of Laboratory Medicine 7e; Yamada's Textbook of Gastroenterology 7e
This is a shared conversation. Sign in to Orris to start your own chat.