analyse_media
Reading File
This is a peripheral blood smear (Wright-Giemsa stain) with the task "Identify the types of WBCs." Here is a complete analysis:
WBC Identification - Peripheral Blood Smear
WBCs Identified: 2 Types
1. Neutrophils (Segmented/Polymorphonuclear Neutrophils)
Count visible: 2 (upper-right quadrant and lower-left quadrant)
Morphological features:
- Size: ~10-15 µm (roughly 2x the diameter of surrounding RBCs)
- Nucleus: Multi-lobed (3-4 lobes) connected by thin chromatin strands - this is the hallmark feature. Dense, dark purple-staining chromatin.
- Cytoplasm: Pale pink-gray, abundant, filled with fine neutral-staining (neither deeply pink nor blue) granules - these contain myeloperoxidase, elastase, and defensins
- Normal differential: 50-70% of circulating WBCs
Function: First-line defense against bacterial and fungal infections; phagocytosis and degranulation
2. Lymphocytes (Small Lymphocytes)
Count visible: 2 (one just below the upper neutrophil; one in the lower-middle area)
Morphological features:
- Size: ~7-10 µm (similar to or slightly larger than an RBC)
- Nucleus: Large, round to slightly kidney-shaped, occupying ~90% of the cell volume. Deeply clumped, dark purple chromatin ("clock-face" or "soccer ball" condensation pattern)
- Cytoplasm: Scant, narrow crescent-shaped pale blue rim - barely visible around the nucleus
- Agranular (no specific granules visible)
- Normal differential: 20-40% of circulating WBCs
Function: Adaptive immunity - T cells (cell-mediated), B cells (humoral/antibody production), NK cells
Other Cells Visible
- Red blood cells (erythrocytes): Abundant, biconcave discs with central pallor (~1/3 diameter), normal morphology
- Platelets: Small purple granular fragments visible in clusters (lower-middle area of the smear)
Summary Table
| Cell Type | Nucleus | Cytoplasm | Size | % Normal |
|---|---|---|---|---|
| Neutrophil | Multi-lobed (3-5 lobes) | Pale pink, fine granules | 10-15 µm | 50-70% |
| Lymphocyte | Round, dense, large | Scant pale blue rim | 7-10 µm | 20-40% |
Note: No monocytes, eosinophils, or basophils are visible in this particular field, though they would normally be present in a complete differential (monocytes 2-8%, eosinophils 1-4%, basophils <1%).
Cushing syndrome key points
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Here are the key points on Cushing Syndrome, drawn from multiple textbooks:
Cushing Syndrome - Key Points
Definition
- Cushing Syndrome = clinical state resulting from prolonged, excessive exposure to glucocorticoids (endogenous or exogenous)
- Cushing Disease = specifically caused by an ACTH-secreting pituitary adenoma (subset of Cushing syndrome)
Causes (Etiology)
| Category | Cause | Notes |
|---|---|---|
| Most common overall | Exogenous glucocorticoids | Iatrogenic; >20 mg prednisone/day for >1 month |
| ACTH-dependent | Pituitary adenoma (Cushing disease) | 65-80% of endogenous cases; usually microadenoma (<1 cm) |
| ACTH-dependent | Ectopic ACTH production | Small cell lung carcinoma, carcinoid, pancreatic islet cell tumors, medullary thyroid Ca |
| ACTH-independent | Adrenal adenoma | ~10% of endogenous cases |
| ACTH-independent | Adrenal carcinoma | ~8% of endogenous cases |
Endogenous breakdown: 65% pituitary, 12% ectopic ACTH, 10% adrenal adenoma, 8% adrenal carcinoma (Robbins/Adams & Victor).
Pathophysiology
- The hypothalamic-pituitary-adrenal (HPA) axis normally regulates cortisol via negative feedback
- CRH (hypothalamus) → ACTH (anterior pituitary) → Cortisol (zona fasciculata of adrenal cortex)
- Cortisol normally peaks in the morning; nadir at ~11 PM - loss of this circadian rhythm is pathologic
- High cortisol: induces gluconeogenesis, inhibits glucose uptake, promotes catabolism, suppresses immunity
Clinical Features
Classic "moon face + buffalo hump" triad:
- Central obesity - truncal fat deposition
- Moon facies - round, full face
- Buffalo hump - dorsocervical fat pad
Full feature list:
- Hypertension (most common cardiovascular sign)
- Proximal muscle weakness / myopathy (type 2 myofiber atrophy)
- Purple/violaceous abdominal striae (wide, >1 cm - distinguishes from normal striae)
- Thin, fragile skin with easy bruising
- Impaired wound healing
- Osteoporosis / vertebral fractures / thoracic kyphosis
- Hyperglycemia / secondary diabetes (18-30% prevalence)
- Hirsutism, acne
- Menstrual irregularities / amenorrhea
- Hyperpigmentation (particularly in ectopic ACTH - due to very high ACTH stimulating melanocortin receptors)
- Psychiatric disturbances (depression, psychosis, cognitive impairment)
- Hypokalemia (especially in ectopic ACTH syndrome)
Ectopic ACTH differs by more rapid onset, greater hypokalemia, more severe hyperpigmentation, and ACTH levels often >50 pg/mL.
Diagnosis
Step 1 - Screening (confirm hypercortisolism)
Three options:
- Late-night (11 PM) salivary cortisol - most sensitive and specific screening test
- 24-hour urinary free cortisol (do 2 consecutive days to increase sensitivity)
- 1 mg overnight dexamethasone suppression test (DST) - give 1 mg dexamethasone at midnight; measure cortisol at 8 AM; normal = suppression to <1.8 µg/dL
Pseudo-Cushing (false positives): alcoholism, major depression, eating disorders, severe stress.
Step 2 - Localization (find the cause)
| Test | Interpretation |
|---|---|
| Plasma ACTH | Low/undetectable = ACTH-independent (adrenal source); Normal/high = ACTH-dependent |
| High-dose DST (2 mg q6h × 2 days or 8 mg single dose) | Suppression (>90% reduction in urinary cortisol) = pituitary (Cushing disease). No suppression = ectopic or adrenal |
| CRH stimulation test | Rise in ACTH/cortisol = pituitary; no rise = ectopic |
| Inferior petrosal sinus sampling (IPSS) | Gold standard to confirm pituitary source when imaging is negative |
| MRI pituitary | Identifies adenoma (enlarged sella in only ~20% of cases) |
| CT adrenals | For adrenal causes |
Adrenal Pathology (Robbins)
| Cause | Adrenal Finding |
|---|---|
| Exogenous steroids | Bilateral cortical atrophy (lack of ACTH stimulation) |
| Pituitary/ectopic ACTH | Bilateral diffuse hyperplasia (up to 30 g each) |
| Adrenal adenoma | Unilateral yellow tumor <30 g; contralateral adrenal atrophied |
| Adrenal carcinoma | Large unencapsulated mass >200-300 g; anaplastic features |
| Primary macronodular hyperplasia | Both glands replaced by 10-30 mm nodules |
Treatment
| Cause | Treatment |
|---|---|
| Pituitary adenoma (microadenoma) | Transsphenoidal pituitary surgery (first-line) |
| Pituitary (failed surgery) | Gamma knife / proton beam radiation |
| Adrenal adenoma | Unilateral adrenalectomy |
| Adrenal carcinoma | Adrenalectomy + mitotane |
| Ectopic ACTH | Treat primary tumor; bilateral adrenalectomy if tumor unresectable |
| Exogenous | Taper steroids gradually |
Nelson Syndrome
- Occurs in ~10% of patients with Cushing disease treated with bilateral adrenalectomy
- Removal of adrenal glands removes cortisol-mediated feedback → pituitary adenoma enlarges rapidly
- Features: severe hyperpigmentation (very high ACTH) + mass effects from expanding pituitary tumor
- Now rare because transsphenoidal surgery is preferred over bilateral adrenalectomy
Cardiac Effects (Braunwald's)
- ECG changes: altered PR and QT intervals
- Cortisol excess → cardiac remodeling, fibrosis, impaired diastolic relaxation
- Hypertension interacts with cortisol excess to worsen structural/functional changes
- Metabolic syndrome: central obesity + insulin resistance + dyslipidemia + prothrombotic state
Sources: Adams & Victor's Principles of Neurology 12e, Robbins & Cotran Pathologic Basis of Disease, Campbell-Walsh Urology, Braunwald's Heart Disease, Bradley & Daroff's Neurology in Clinical Practice
Functions of glucocorticoid sumnary
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent content from Katzung's Pharmacology and Guyton's Physiology. Here is a clean summary:
Functions of Glucocorticoids - Summary
Primary glucocorticoid: Cortisol (hydrocortisone) - secreted by the zona fasciculata of the adrenal cortex; ~90% bound to CBG in plasma; t½ = 60-90 minutes; follows a circadian rhythm (peak in early morning).
1. Metabolic Effects
Carbohydrate Metabolism
- Stimulates gluconeogenesis (upregulates phosphoenolpyruvate carboxykinase, glucose-6-phosphatase)
- Stimulates glycogen synthesis in the liver
- Inhibits peripheral glucose uptake by muscle cells → hyperglycemia
- Net effect: raises blood glucose (anti-insulin action)
Protein Metabolism
- Catabolic in peripheral tissues (muscle, skin, lymphoid, connective tissue) - releases amino acids for gluconeogenesis
- Anabolic in the liver (stimulates hepatic protein and RNA synthesis)
- Results in: muscle wasting, thin skin, poor wound healing, growth retardation in children
Fat Metabolism
- Stimulates lipolysis via hormone-sensitive lipase → increases free fatty acids and glycerol in blood
- Promotes fat redistribution to visceral, facial (moon face), nuchal (buffalo hump), and supraclavicular depots
- Stimulates insulin release (secondary to hyperglycemia) → net lipogenesis at central depots
2. Anti-inflammatory Effects
- Dramatically reduce manifestations of inflammation by:
- Suppressing inflammatory cytokines and chemokines
- Inhibiting leukocyte adhesion molecules → prevents extravasation into tissues
- Inducing lipocortin (annexin-1) → inhibits phospholipase A2 → blocks arachidonic acid release → suppresses both COX and lipoxygenase pathways (prostaglandins + leukotrienes ↓)
- Blocking production of IL-1, IL-2, IL-6, TNF-α, IFN-γ
- Inhibiting NF-κB pathway
Effect on WBC counts (after a single dose, maximal at 6 hours):
| Cell | Effect | Mechanism |
|---|---|---|
| Neutrophils | ↑ (neutrophilia) | ↑ release from bone marrow + ↓ migration out of vessels |
| Lymphocytes | ↓ | Redistribution to lymphoid tissue |
| Monocytes | ↓ | Redistribution |
| Eosinophils | ↓ | Redistribution |
| Basophils | ↓ | Redistribution |
3. Immunosuppressive Effects
- Suppresses cell-mediated immunity (T-cell function)
- Reduces antibody production at high doses
- Promotes apoptosis of lymphocytes and eosinophils
- Decreases circulating immunoglobulins
4. Cardiovascular Effects ("Permissive" Functions)
- Maintain the responsiveness of vascular smooth muscle to catecholamines (vasopressor effect) - without cortisol, vessels lose tone → hypotension (seen in Addison disease)
- Contribute to sodium retention and blood pressure maintenance (via weak mineralocorticoid activity at high levels)
- Excessive cortisol → hypertension (multiple mechanisms: mineralocorticoid receptor activation, enhanced pressor response)
5. Renal Effects
- Maintain normal glomerular filtration rate
- Help excrete free water (cortisol deficiency → impaired water excretion + inappropriate ADH secretion)
- High cortisol overwhelms 11β-HSD2 in kidney → activates mineralocorticoid receptors → Na⁺ retention, K⁺ loss, hypokalemia, hypertension
6. Bone Effects
- Inhibit osteoblasts (↓ bone formation)
- Enhance osteoclast activity (↑ bone resorption)
- Antagonize vitamin D → ↓ intestinal calcium absorption → ↑ PTH secretion → secondary hyperparathyroidism
- Net result: osteoporosis (major long-term complication of glucocorticoid therapy)
7. CNS / Neurological Effects
- Modulate mood and cognition - deficiency causes slowing of EEG, depression
- Excess causes: insomnia → euphoria → depression; rarely pseudotumor cerebri
- Suppress pituitary ACTH, GH, TSH, and LH secretion (chronic use)
8. Pulmonary / Developmental Effects
- Stimulate fetal lung maturation and surfactant production (used clinically in preterm labor)
- Used therapeutically for respiratory distress syndrome (RDS) prophylaxis
9. Hematopoietic Effects
- ↑ platelets and red blood cells
- ↑ neutrophils (as above)
- ↓ lymphocytes, eosinophils, monocytes, basophils
10. GI Effects
- Promote peptic ulcer (possibly by suppressing local immune defense against H. pylori)
- Increase gastric acid secretion
Mechanism of Action (Summary)
- Cortisol enters cell (lipid-soluble steroid)
- Binds cytoplasmic glucocorticoid receptor (GR) (dissociates hsp90)
- GR dimerizes → translocates to nucleus
- Binds glucocorticoid response elements (GREs) in gene promoters
- Regulates transcription of ~10-20% of all expressed genes
- Also inhibits NF-κB directly (key anti-inflammatory mechanism)
- Rapid (non-genomic) effects also occur via membrane-associated receptors
Quick Reference Table
| System | Physiologic Effect |
|---|---|
| Glucose | ↑ gluconeogenesis, ↑ glycogen synthesis, ↓ peripheral uptake → hyperglycemia |
| Protein | Catabolism in periphery, anabolism in liver → muscle wasting |
| Fat | Lipolysis + central redistribution → central obesity |
| Immunity | ↓ cytokines, ↓ adhesion molecules → anti-inflammatory / immunosuppressive |
| WBCs | ↑ neutrophils; ↓ lymphocytes, eosinophils, monocytes |
| Bone | ↓ formation, ↑ resorption → osteoporosis |
| CVS | Maintains vascular tone (permissive for catecholamines), supports BP |
| Kidney | Maintains GFR, free water excretion |
| CNS | Mood effects; suppresses ACTH/GH/TSH/LH |
| Lung | Surfactant production (fetal) |
| Platelets/RBC | ↑ |
Sources: Katzung's Basic & Clinical Pharmacology 16e, Guyton & Hall Textbook of Medical Physiology
Rickets sumnary
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a complete summary of Rickets from multiple textbook sources:
Rickets - Summary
Definition
Rickets is a metabolic disorder of failure of bone mineralization at the growth plates in children (= osteomalacia in adults), caused by a reduced calcium-phosphate product in the extracellular fluid surrounding developing physes. The core defect is disruption of the normal chondrocyte scaffold at the metaphyses.
Vitamin D / Calcium / Phosphate Pathway
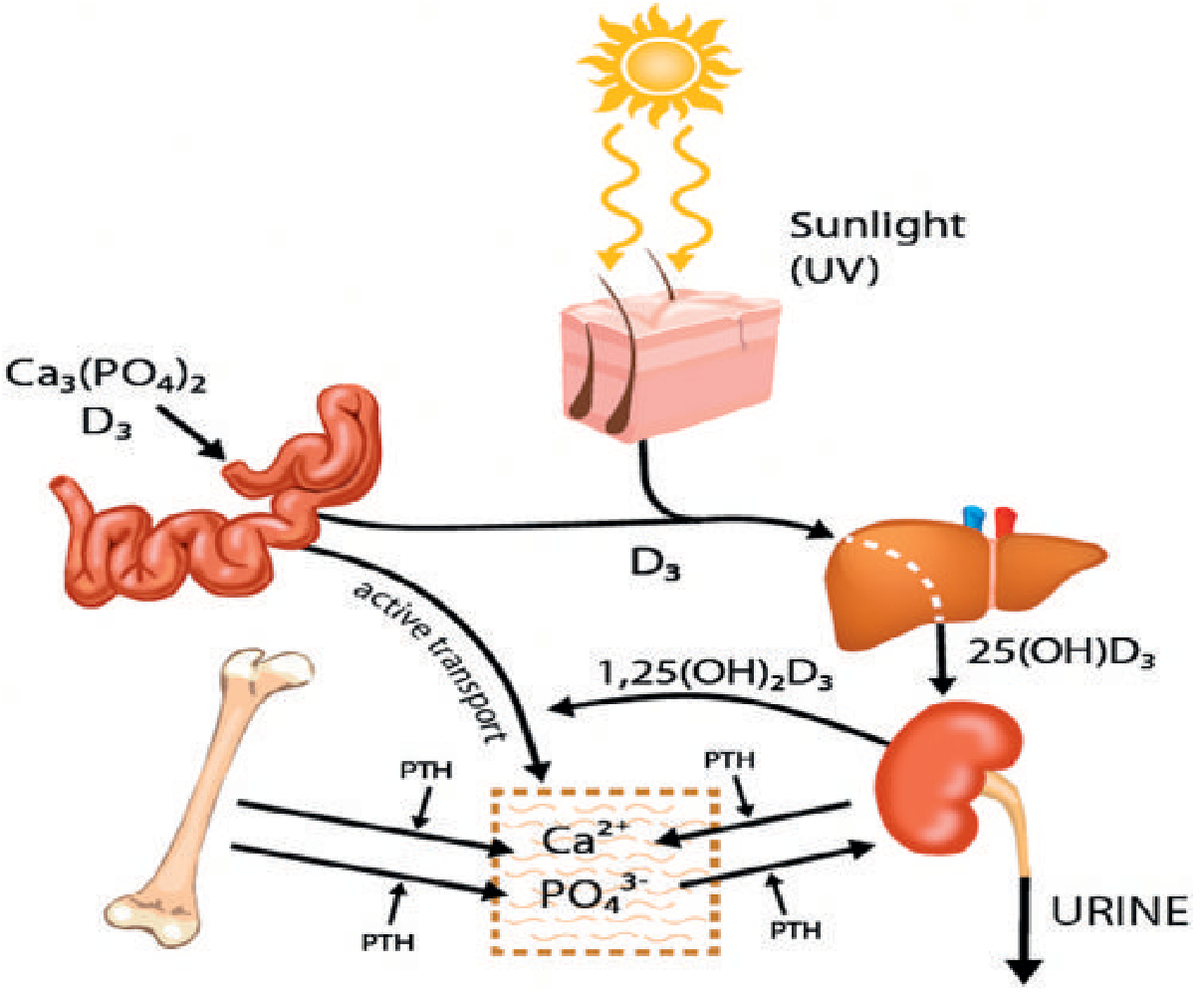
- Sunlight (UV) → skin → Vitamin D3 (cholecalciferol)
- Liver → 25(OH)D3 (25-hydroxyvitamin D) - storage form, measured in blood
- Kidney (1α-hydroxylase) → 1,25(OH)2D3 (calcitriol) - active form
- Active vitamin D → enhances intestinal absorption of Ca²⁺ and PO₄³⁻
- Without vitamin D: only 10-15% of dietary calcium and 60% of phosphorus are absorbed
Causes / Classification
A. Nutritional / Vitamin D-Deficiency Rickets
Most common type. Rare in developed countries since vitamin D fortification of milk, but still seen in:
- Asian immigrants, breastfed infants (breast milk is low in vitamin D)
- Premature infants
- Malabsorption syndromes (celiac disease, steatorrhea)
- Patients with little sunlight exposure
- Long-term parenteral nutrition
Pathophysiology:
Low vitamin D → ↓ Ca/PO₄ absorption → ↓ serum Ca²⁺ → PTH rises (secondary hyperparathyroidism) → PTH mobilizes bone Ca²⁺ (maintains Ca near normal) BUT increases urinary PO₄ excretion → PO₄ falls markedly
B. Calcium-Deficiency Rickets
- Adequate vitamin D but inadequate dietary calcium intake
- Common in parts of Africa and Asia
C. Phosphate-Deficiency Rickets
- Low dietary phosphate or excessive urinary loss
D. Hereditary Vitamin D-Dependent Rickets (VDDR)
Both are autosomal recessive:
| Type | Defect | Features |
|---|---|---|
| Type I | Deficient renal 1α-hydroxylase (chromosome 12q14) | Cannot activate 25(OH)D3 → low 1,25(OH)2D3; presents <2 years; severe bony changes, hypocalcemic tetany, seizures |
| Type II | Defective VDR (vitamin D receptor) on target organs | Normal or high 1,25(OH)2D3 levels; presents <1 year; associated with alopecia, poor dentition |
E. Familial Hypophosphatemic Rickets (Vitamin D-Resistant Rickets / Phosphate Diabetes)
- Most common heritable form of rickets
- X-linked dominant - mutation in PHEX gene (phosphate-regulating neutral endopeptidase)
- Impaired renal tubular reabsorption of phosphate → phosphaturia → low serum PO₄
- Elevated FGF23 is the key mediator
- Labs: normal Ca, low PO₄, low 1,25(OH)2D3, high ALP; normal PTH
- Features: severe bowing, short stature, dental abnormalities
- Treatment: Burosumab (anti-FGF23 monoclonal antibody) - first-line; or elemental phosphate + calcitriol (second-line)
F. Renal Osteodystrophy (Renal Rickets)
- Chronic kidney disease → failure of second hydroxylation step (no 1α-hydroxylase)
- Phosphate retention + hypocalcemia → secondary hyperparathyroidism
- Labs: ↑ PO₄, ↑ ALP, ↑ PTH, low-normal Ca
Pathology at the Growth Plate
Normal: chondrocytes organize into columns → hypertrophy → apoptosis → mineralization
Rickets: Low Ca-PO₄ disrupts chondrocyte apoptosis → disorganized, expanded, hypomineralized growth plate
- Widened zone of hypertrophy
- Poorly defined zone of provisional calcification
- Widened osteoid seams ("Swiss cheese trabeculae")
Bones also show: osteoclastic resorption (PTH-driven) + osteoblastic laying of uncalcified osteoid → progressively weak, deformable bone.
Clinical Features
| Feature | Description |
|---|---|
| Short stature | Height below 5th percentile |
| Limb bowing | Genu varum (bow legs) - most common deformity |
| Rachitic rosary | Enlarged costochondral junctions - beaded ribs |
| Harrison's sulcus | Groove along lower chest from diaphragm pull |
| Craniotabes | Softening of skull bones in infants |
| Frontal bossing | Prominent forehead |
| Delayed dentition / dental disease | |
| Muscle hypotonia | Generalized weakness, waddling gait |
| Pathologic fractures | Looser zones (pseudofractures) |
| Bone pain | |
| Tetany | Late finding when Ca finally falls below 7 mg/dL - may cause respiratory spasm |
Laboratory Findings (Vitamin D-Deficiency Rickets)
| Test | Result | Reason |
|---|---|---|
| Serum Calcium | Low-normal (maintained) | PTH compensates via bone resorption |
| Serum Phosphate | Markedly low | PTH increases urinary excretion |
| Alkaline Phosphatase | ↑↑ (elevated) | Increased osteoblastic activity |
| PTH | ↑ (secondary hyperparathyroidism) | Response to low Ca |
| 25(OH)D3 | Low | Confirms deficiency |
| 1,25(OH)2D3 | Low or inappropriately normal |
Radiographic Findings
| Finding | Description |
|---|---|
| Physeal widening | Wide, hazy growth plates - key sign |
| Metaphyseal cupping and fraying | "Paintbrush" or "celery stalk" appearance |
| Coxa vara | Hip deformity |
| Codfish vertebrae | Biconcave vertebral bodies |
| Looser zones | Transverse radiolucent pseudofractures (stress zones) at pubic rami, medial femoral neck, axillary scapula, ribs |
| Bowing of long bones | Lower limbs most affected |
| Reduced bone density overall | Osteopenia |
Treatment
| Type | Treatment |
|---|---|
| Nutritional (Vit D deficiency) | Vitamin D 1000-6000 IU/day (based on weight) + adequate dietary Ca/PO₄; most deformities resolve |
| VDDR Type I | Calcitriol (1,25(OH)2D3) replacement |
| VDDR Type II | High-dose calcitriol; calcium infusions |
| XLH (phosphate diabetes) | Burosumab (anti-FGF23) first-line; or elemental phosphate + calcitriol |
| Renal osteodystrophy | Calcitriol, phosphate binders, manage CKD |
Osteomalacia (Adult Rickets)
- Same pathology as rickets but in adults (no growth plates)
- Growth plate changes absent; features are bone pain, tenderness, Looser zones, fractures
- Common causes: steatorrhea (fat malabsorption → vitamin D and Ca lost in feces), malabsorption, CKD
- Less likely to develop tetany than children
Sources: Miller's Review of Orthopaedics 9e, Grainger & Allison's Diagnostic Radiology, Guyton & Hall Medical Physiology, Adams & Victor's Neurology
This is a shared conversation. Sign in to Orris to start your own chat.