pericarditis
Reading File
Finding Sources
Searching PubMed
pericarditis
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have comprehensive information from Braunwald's and Rosen's. Now I'll compile a thorough answer.
Pericarditis
Definition and Overview
Pericarditis is inflammation of the pericardium - the two-layered fibroserous sac surrounding the heart. It is a common cause of chest pain, accounting for approximately 5% of all non-ischemic chest pain presentations in the emergency department, with an incidence of ~27.7 cases per 100,000 population/year. Men aged 16-65 are at higher risk than women (RR ~2.0).
Etiology
In developed countries, 80-90% of cases are idiopathic (presumed viral - testing for specific viruses has low yield and little impact on management).
| Category | Examples |
|---|---|
| Viral (most common) | Coxsackievirus, echovirus, adenovirus, EBV, CMV, HIV, influenza |
| Bacterial | Staphylococcus, Streptococcus, TB (most common cause in developing countries) |
| Fungal/parasitic | Histoplasma, Candida, Toxoplasma |
| Post-cardiac injury | Post-MI (early), Dressler syndrome (2-8 wks post-MI), post-cardiac surgery, trauma |
| Systemic/autoimmune | SLE (40-80% at autopsy), RA, SSc, sarcoidosis, amyloidosis |
| Uremia | Most common systemic disorder associated - treat with intensive dialysis |
| Malignancy | Metastatic (lung, breast, lymphoma); often bloody effusion |
| Radiation | Mediastinal irradiation |
| Drugs | Hydralazine, procainamide, isoniazid, phenytoin |
TB is the most common cause in endemic/developing regions and must always be considered in those populations.
Pathophysiology
The pericardium consists of two layers with a narrow space containing 15-35 mL of fluid normally. Inflammation causes:
- Edema and thickening of the parietal layer
- Production of exudative pericardial fluid
- Increased friction between layers (causing the rub)
Morphological patterns (from Robbins Pathology):
- Fibrinous/fibrinopurulent - viral/uremic (shaggy, "bread-and-butter" appearance)
- Suppurative/purulent - bacterial (pus formation)
- Caseous - tuberculous
- Hemorrhagic - malignancy
Clinical Presentation
Symptoms
- Chest pain - sharp, pleuritic, retrosternal; worsened by lying supine, deep inspiration, and swallowing; relieved by sitting forward
- Radiation to the trapezius ridge or back (characteristic - from phrenic nerve involvement)
- Low-grade fever and myalgias
- Dyspnea
Signs
- Pericardial friction rub - pathognomonic, present in ~1/3 of cases
- Best heard: lower left sternal border, patient leaning forward in full expiration
- Classic rub = 3 components (ventricular systole + early diastole + atrial contraction), described as "walking on crunchy snow"
- Evanescent and intermittent - may require repeated auscultation
- Low-grade fever (<38°C), sinus tachycardia
- Atrial fibrillation/flutter in ~5%
Diagnostic Criteria
Diagnosis requires at least 2 of the 4 classic criteria:
- Characteristic chest pain (positional/pleuritic)
- Pericardial friction rub
- ECG changes
- New or worsening pericardial effusion
ECG Changes (4 classic stages)
| Stage | Findings |
|---|---|
| I (acute) | Diffuse, concave ("saddle-shaped") ST elevation in most leads; PR depression (most specific) |
| II | ST returns to baseline; T waves flatten |
| III | T-wave inversions (diffuse) |
| IV | ECG normalizes |
Key ECG distinction from STEMI: pericarditis has diffuse ST elevation (not focal/territorial) with PR depression, and ST elevation is concave (saddle-shaped), not convex.
Laboratory Testing
- CRP/ESR/WBC - elevated; CRP is the best marker for activity and guides treatment duration
- Troponin - mildly elevated in ~30% (myopericarditis); significant elevation suggests concurrent myocarditis
- BUN/Cr - check for uremia
- ANA, rheumatoid factor if autoimmune etiology suspected
- Blood cultures, PPD/IGRA if infectious etiology suspected
Imaging
- Chest X-ray - often normal in uncomplicated pericarditis; "water-bottle" cardiac silhouette if large effusion (>250 mL)
- Echocardiography - should be performed in all cases; detects effusion, wall motion abnormalities (myocarditis), tamponade physiology
- Cardiac MRI - gold standard for detecting pericardial inflammation (gadolinium enhancement); defines extent of involvement and differentiates pericarditis from myocarditis
High-Risk Features (Hospitalize)
The following "red flags" warrant hospitalization and workup for specific etiology:
- Fever >38°C
- Subacute onset
- Large pericardial effusion or cardiac tamponade
- Failure to respond to NSAIDs after 1 week
- Myocarditis (elevated troponin)
- Immunocompromised state
- Trauma
- Oral anticoagulant use
- Pregnancy
Treatment
Acute/Idiopathic Pericarditis
First-line (dual therapy):
| Drug | Dose | Duration |
|---|---|---|
| Aspirin | 750-1000 mg every 8 hr | 1-2 weeks, then taper over 2-3 weeks |
| Ibuprofen | 600-800 mg every 8 hr | 1-2 weeks, then taper over 2-3 weeks |
| Colchicine | 0.5 mg once daily (<70 kg) or 0.5 mg twice daily (≥70 kg) | 3 months |
- NSAID + colchicine is the recommended combination - colchicine significantly reduces recurrence
- Taper only when asymptomatic AND CRP normalized
- Gastric protection (PPI) with NSAIDs
Corticosteroids - use is minimized because they may:
- Impair clearance of infectious agents
- Increase risk of recurrence
- Reserved for: NSAID/colchicine failure or contraindications, autoimmune disease, renal failure, pregnancy
- If used: low dose prednisone 0.2-0.5 mg/kg/day, taper over 6-12 weeks guided by symptoms and CRP; concurrent colchicine recommended
Specific Causes
- Uremic pericarditis: intensive dialysis + NSAIDs (indomethacin 25 mg TID); steroids for refractory cases
- Post-MI (early): aspirin (preferred; avoid ibuprofen which affects infarct healing)
- Dressler syndrome: NSAIDs (ibuprofen 600 mg QID or indomethacin 25 mg TID); discontinue anticoagulants if possible
- Tuberculous pericarditis: antituberculous therapy + corticosteroids to reduce constrictive pericarditis risk
- Bacterial/purulent: IV antibiotics + urgent pericardial drainage
- Activity restriction: until asymptomatic + CRP normal (athletes: minimum 3 months)
Recurrent Pericarditis
- Occurs in 15-30% of idiopathic cases
- Definition: new episode after a symptom-free interval of ≥4-6 weeks with objective evidence of recurrence (rub, ECG changes, new effusion, elevated CRP)
- Treatment: repeat NSAID + colchicine (same doses)
- Refractory recurrences: corticosteroids ("triple therapy"); anakinra (IL-1 blocker) shown effective in corticosteroid-dependent recurrent pericarditis
- Recurrences have not been associated with evolution to constrictive pericarditis in idiopathic cases
Complications
| Complication | Notes |
|---|---|
| Pericardial effusion | Common (small effusions in most cases) |
| Cardiac tamponade | ~3% over 31 months; more common with identified specific cause (bacterial, malignant, TB) |
| Constrictive pericarditis | ~1.5-1.8%; extremely rare in idiopathic pericarditis (0.48%) |
Cardiac Tamponade (emergency)
- Beck's triad: hypotension + elevated JVP + muffled heart sounds
- Pulsus paradoxus >10 mmHg
- ECG: electrical alternans
- Treatment: urgent pericardiocentesis
Constrictive Pericarditis
- Dense fibrous scarring obliterates pericardial space
- Right-sided venous distension + low cardiac output (similar to restrictive cardiomyopathy)
- Kussmaul sign (JVP rises on inspiration)
- Treatment: pericardiectomy
Special Situations
Myopericarditis
- Up to 15% of pericarditis cases have concurrent myocarditis
- Elevated troponin, wall motion abnormalities on echo
- Cardiac MRI confirms myocardial involvement
- Strict activity restriction; avoid competitive sports for at least 3-6 months
Pericarditis in Autoimmune Disease
- SLE: typically complicates disease flare; polyserositis; clinically significant tamponade in only 1-2%
- RA: clinically significant pericarditis in only 1-2%; constrictive pericarditis can develop over months; aggressive DMARD/biologic therapy appears to reduce incidence
- SSc: small pericardial effusions common, rarely hemodynamically significant; large rapidly accumulating effusions occasionally occur with dSSc
Sources: Braunwald's Heart Disease (11e), Rosen's Emergency Medicine (10e), Robbins & Kumar Basic Pathology (10e), Goldman-Cecil Medicine
dry pericarditis and pericardial effusion
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich content from multiple authoritative sources. Let me compile the comprehensive answer.
Dry (Fibrinous) Pericarditis and Pericardial Effusion
PART 1 - DRY (FIBRINOUS) PERICARDITIS
What Is "Dry" Pericarditis?
"Dry pericarditis" is the clinical/historical term for fibrinous pericarditis - the form where the pericardial inflammation produces a fibrinous exudate without significant fluid accumulation. It is the most common morphological type and is classically seen in viral/idiopathic pericarditis and uremia.
The name reflects the absence of a significant effusion, with the pericardial surfaces essentially rubbing against each other - "dry."
Pathophysiology
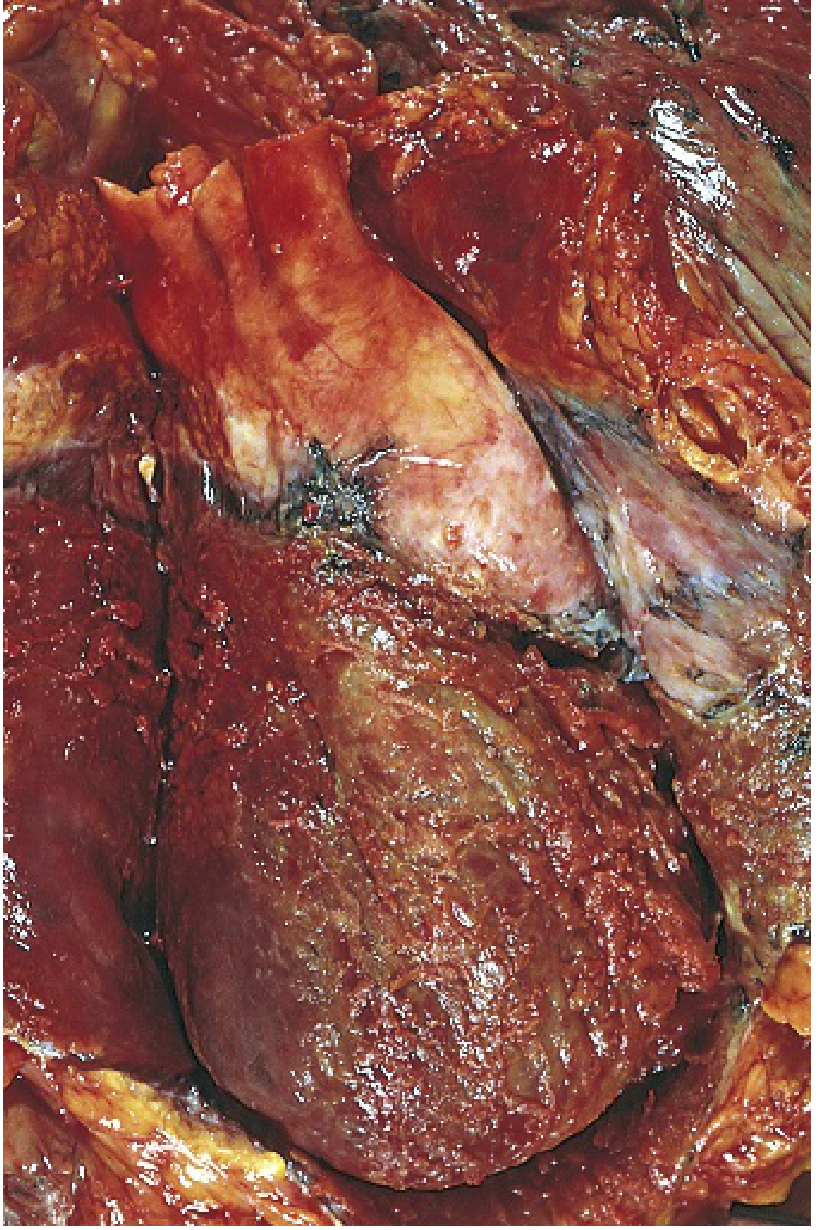
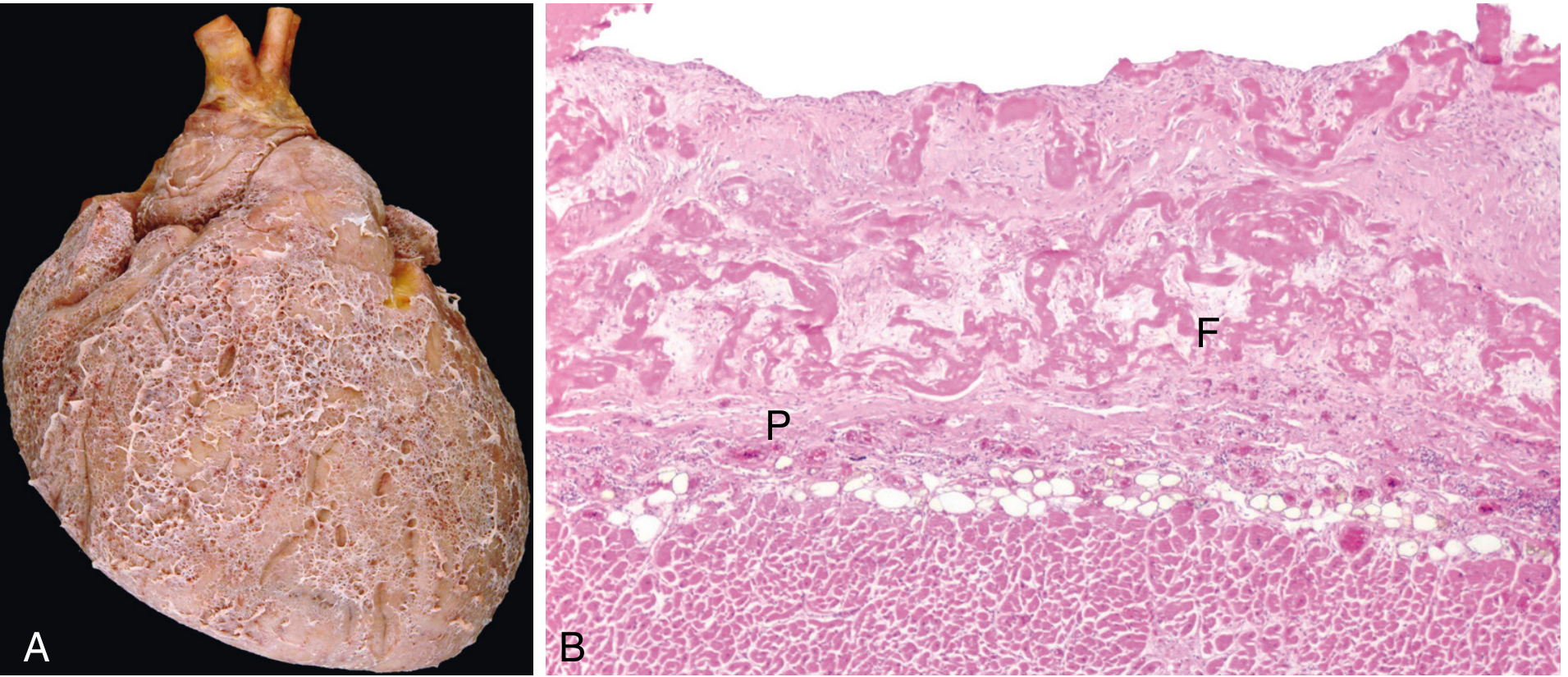
When vascular permeability increases significantly during inflammation, large molecules including fibrinogen escape the vasculature. Fibrinogen is then converted to fibrin and deposits on the pericardial surfaces. This fibrinous exudate forms between the parietal and visceral pericardial layers.
Grossly, this produces the classic "bread-and-butter" pericardium - described by Laennec in 1819 - where the shaggy fibrinous deposits on both surfaces resemble two buttered pieces of bread pulled apart.
Causes of Fibrinous/Dry Pericarditis
- Viral/idiopathic - most common; coxsackievirus B, echovirus, adenovirus, EBV, CMV, HIV
- Uremia - classic cause; fibrinous exudate is the hallmark
- Acute MI - early post-infarction (epistenocardiac) pericarditis, 2-4 days after transmural infarction
- Rheumatic fever - fibrinous pericarditis as part of pancarditis; resolves without residua
- Autoimmune - SLE, RA, scleroderma
Clinical Features of Dry Pericarditis
Chest pain is the dominant symptom:
- Sharp, pleuritic, retrosternal
- Worsened by lying flat (supine), deep inspiration, and swallowing
- Relieved by sitting forward/leaning forward
- May radiate to the trapezius ridge (phrenic nerve involvement) - highly specific for pericarditis
Pericardial friction rub - the hallmark sign:
- Results from friction between inflamed/fibrinous visceral and parietal pericardial surfaces (and sometimes parietal pericardium vs adjacent pleura)
- Classic rub = 3 components: ventricular systole + early diastole + atrial contraction ("crunchy snow" sound)
- Best heard at the lower left sternal border, patient leaning forward in full expiration
- Evanescent and intermittent - requires repeated auscultation
- Importantly: no correlation exists between the size of any effusion and the presence of a rub - a loud rub does not mean no effusion, and an absent rub does not rule out pericarditis
ECG changes (4 classic stages - diffuse, not territorial):
| Stage | Change |
|---|---|
| I (days 1-2) | Diffuse concave (saddle-shaped) ST elevation + PR depression (most specific sign) |
| II (days 3-7) | ST normalizes, T waves flatten |
| III | Diffuse T-wave inversions |
| IV | ECG normalizes |
- PR depression in multiple leads is the most specific ECG sign
- Distinction from STEMI: diffuse (not focal), concave ST elevation, PR depression, no reciprocal ST depression (except in aVR and V1)
Fate of Fibrinous Exudate
Two outcomes:
- Resolution - fibrinolysis dissolves the exudate; macrophages clear it - no sequelae (most common)
- Organization - fibroblasts and blood vessels grow into fibrin; leads to fibrous scarring - potentially constrictive pericarditis
PART 2 - PERICARDIAL EFFUSION
Definition and Normal Values
The pericardium normally contains 15-35 mL of serous fluid (ultrafiltrate of plasma). Any accumulation >50 mL is considered abnormal. Pericardial effusion refers to excess fluid accumulation in the pericardial space.
Classification
By fluid type:
| Type | Characteristics | Common Causes |
|---|---|---|
| Transudate | Clear, protein-poor, low LDH | Heart failure, hypoalbuminemia, hypothyroidism, uremia |
| Exudate | Protein-rich, high LDH, turbid | Infection, inflammation, malignancy |
| Hemorrhagic (hemopericardium) | Frank blood | Trauma, aortic dissection, post-MI wall rupture, malignancy, anticoagulants |
| Chylous | Milky (lymph) | Lymphatic obstruction, thoracic duct injury |
By size (echocardiographic):
| Size | Separation | Distribution |
|---|---|---|
| Small | <10 mm | Posterior only (gravitational) |
| Moderate | 10-20 mm (100-500 mL) | Circumferential; pericardial space anterior to RV >5 mm |
| Large | >20 mm | Circumferential; surrounds entire heart |
By onset:
- Acute vs subacute vs chronic (>3 months)
Causes
- Viral/idiopathic pericarditis - most common cause overall
- Malignancy - lung, breast, lymphoma; often bloody; large effusions; irregular/nodular pericardium on CT/MRI
- Uremia - large effusions possible; rarely hemodynamically significant unless on inadequate dialysis
- Trauma - hemopericardium
- Aortic dissection - hemopericardium; life-threatening (pericardiocentesis is CONTRAINDICATED - may worsen dissection)
- Post-MI wall rupture - sudden hemopericardium; surgical emergency
- Autoimmune diseases - SLE (1-2% develop tamponade), RA, SSc
- Radiation - post-mediastinal irradiation
- Hypothyroidism (myxedema) - large, slowly accumulating transudates; rarely cause tamponade
- Heart failure - transudative effusion
- Post-cardiac surgery / post-pericardiotomy syndrome
- Bacterial/TB - purulent; high risk of tamponade and constriction
Clinical Presentation
Small to moderate effusions - often asymptomatic. May have:
- Dull chest ache, pressure
- Dyspnea, cough (compression of adjacent structures)
- Hiccups (phrenic nerve compression)
- Hoarseness (recurrent laryngeal nerve compression)
Large effusions - may compress bronchi, esophagus, and phrenic nerve. Dullness to percussion at the left lung base posteriorly (Ewart's sign - dullness, bronchial breathing, and egophony at the left base).
Key principle: The rate of accumulation matters more than absolute volume. A rapidly developing 200 mL effusion can cause tamponade, while a slowly accumulating 2 L effusion may be clinically silent (pericardium has time to stretch).
Investigations
Chest X-ray:
- Normal until effusion >200-250 mL
- "Water-bottle" (flask) sign - enlarged, globular cardiac silhouette with acute cardiophrenic angles
- Bilateral hilar overlay sign
- Epicardial fat pad sign (lateral view): a band of higher density (fluid) sandwiched between two bands of lower density (epicardial fat posteriorly + mediastinal fat anteriorly) - the "sandwich sign"
- Rapid change in cardiac silhouette size on serial CXRs should raise strong suspicion
- Notably: no change in pulmonary vascular pattern (distinguishes from heart failure)
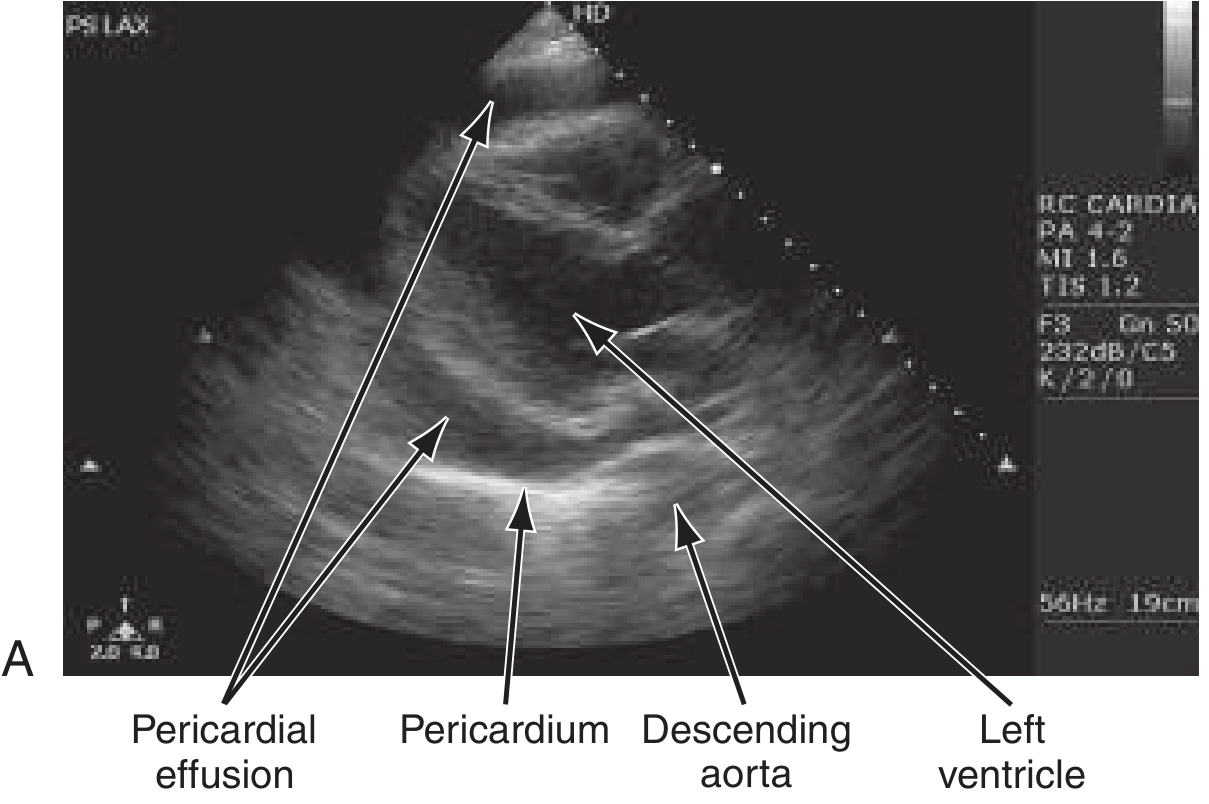
Echocardiography (first-line):
- Echolucent (echo-free) space surrounding the heart
- Small effusions: visible only posterior to the LV
- Moderate-large: circumferential
- Distribution is non-uniform due to gravity - most commonly along the posterolateral LV wall, inferolateral to the RV, and in the superior pericardial recess
- Pericardial thickening: increased echogenicity on 2D; multiple parallel posterior reflections on M-mode
- Limitation: cannot reliably characterize fluid type by echo appearance; anterior loculated effusions may be missed
CT:
- Better than echo for loculated or anterior effusions, overall sizing, and pericardial thickening
- Effusion appears as low-attenuation fluid surrounding the heart
- MRI:
- Transudates/exudates without debris: T1 hypointense, T2/SSFP hyperintense
- Proteinaceous or hemorrhagic effusions: T1 hyperintense
- Pericardial inflammation: gadolinium enhancement of pericardium
- Gold standard for characterizing effusion type, pericardial thickening, and inflammatory activity
Pericardial fluid analysis:
- Rarely diagnostic unless infection is suspected
- Exudate vs transudate (Light's criteria)
- Cell count/differential, culture, cytology (malignancy), ADA (TB)
- Immune complexes, ANA, anti-dsDNA in autoimmune disease
Cardiac Tamponade - When Effusion Becomes Life-Threatening
Tamponade occurs when intrapericardial pressure rises to equal and then exceed right heart filling pressures, impairing diastolic filling.
Pathophysiology:
- Rising pericardial pressure compresses all chambers
- RV compresses first (lower pressure) - RV diastolic collapse (earliest echocardiographic sign)
- Then RA compresses - RA systolic collapse
- Ventricular interdependence is exaggerated: inspiration fills RV more (shifts septum left, reducing LV filling) - produces pulsus paradoxus
Clinical features (Beck's triad):
- Hypotension
- Elevated JVP (distended neck veins)
- Muffled heart sounds
Plus:
- Tachycardia (compensatory)
- Pulsus paradoxus >10 mmHg (exaggerated fall in systolic BP on inspiration)
- Kussmaul sign is typically absent in tamponade (it is present in constriction)
ECG: Electrical alternans - alternating QRS amplitude due to the heart swinging within the effusion (pathognomonic when present)
Echocardiographic signs of tamponade:
- RA systolic collapse (most sensitive)
- RV diastolic collapse (most specific)
- IVC plethora (dilated IVC, <50% collapse with inspiration)
- Respiratory variation in mitral/tricuspid inflow >25-40% (Doppler)
Management: Urgent pericardiocentesis (echo-guided preferred)
- Subxiphoid approach most common
- If hemopericardium from aortic dissection: do NOT drain - surgical repair is required
- If purulent: pericardiectomy or catheter drainage with lavage + fibrinolytics + IV antibiotics
Treatment of Pericardial Effusion (Without Tamponade)
| Effusion Size | Management |
|---|---|
| Small | NSAIDs (ibuprofen 600 mg QID) + treat underlying cause + close follow-up |
| Moderate/asymptomatic | Treat underlying cause; monitor with serial echo |
| Large/symptomatic | Pericardiocentesis (diagnostic + therapeutic) |
| Uremic | Intensive dialysis ± NSAIDs; pericardiocentesis if no response |
| Malignant | Pericardiocentesis; consider pericardial window if recurrent |
| Purulent | Drainage (catheter/window/pericardiectomy) + IV antibiotics |
Patients requiring pericardiocentesis should be hospitalized for serial examination and etiological workup.
Relationship Between Dry Pericarditis and Pericardial Effusion
These represent a spectrum of the same inflammatory process:
Dry/Fibrinous Pericarditis
↓ (if inflammation persists or worsens)
Effusive Pericarditis (pericardial effusion develops)
↓ (if large/rapid accumulation)
Cardiac Tamponade
↓ (if extensive fibrosis)
Constrictive Pericarditis
Importantly:
- Most patients with pericarditis have at least a small effusion at some point, even if clinically "dry"
- A rub does NOT exclude an effusion, and an effusion does NOT exclude a rub
- The progression from dry to effusive to constrictive depends on the etiology - idiopathic/viral cases rarely progress to constriction (0.48%), while TB and bacterial cases have high risk
Sources: Braunwald's Heart Disease (11e), Rosen's Emergency Medicine (10e), Robbins & Cotran Pathologic Basis of Disease (10e), Grainger & Allison's Diagnostic Radiology, Textbook of Clinical Echocardiography, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.