57 yr old female with atrial tachycardia Echo- mild left atrial dilatation rest normal started on Caesar one 100 BD and prominent XL 25 od not hypertensive
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atrial tachycardia" management rate control
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a structured clinical review of this case:
Clinical Analysis: Atrial Tachycardia in a 57-year-old Female
Patient Summary
- 57F, atrial tachycardia (AT), non-hypertensive
- Echo: Mild left atrial (LA) dilatation, rest normal (normal LV function, no structural disease)
- Medications started: Carvedilol 100 mg BD + Ivabradine XL 25 mg OD
Understanding the Diagnosis
Focal atrial tachycardia arises from discrete sites in the atria (pulmonary veins, crista terminalis, tricuspid/mitral annulus, coronary sinus, atrial septum). Mechanisms include enhanced automaticity, triggered activity, or micro-reentry. It is usually regular and rarely exceeds 200 bpm.
Mild LA dilatation in this context is likely a consequence of the sustained tachycardia — elevated atrial pressures over time cause atrial remodeling. This is an important clue that the arrhythmia may be incessant or recurrent enough to cause structural change.
⚠️ Tachycardia-induced cardiomyopathy risk: Incessant atrial tachycardia with a rapid ventricular response can cause a rate-related cardiomyopathy. This condition is reversible once the tachycardia is eliminated and rate normalizes. The mild LA dilatation here warrants vigilance for early LV dysfunction on follow-up. — Fuster and Hurst's The Heart, 15th Edition
Medication Review
1. Carvedilol (Caesar One) 100 mg BD — ⚠️ Dose Concern
Carvedilol is a non-selective β-blocker with α₁-blocking properties. It is appropriate for rate control in atrial tachycardia (β-blockers are first-line for chronic AT management).
However, 100 mg BD is an exceptionally high dose of carvedilol:
- Standard doses: 3.125–25 mg BD for heart failure; up to 25 mg BD for heart failure, 50 mg BD max for hypertension/ischaemic heart disease
- 100 mg BD (200 mg/day) is well above the recommended maximum and could cause:
- Significant bradycardia, especially when combined with ivabradine
- Hypotension (α-blockade), particularly risky as the patient is non-hypertensive
- Fatigue, dizziness, peripheral vasoconstriction
Please verify this dose — it may be a transcription error (e.g., 12.5 mg BD or 25 mg BD is more likely intended, or the drug brand "Caesar One" may contain a different concentration requiring clarification).
2. Ivabradine (Prominent XL) 25 mg OD — ⚠️ Indication Concern
Ivabradine selectively blocks the funny current (If) in the sinus node, reducing heart rate. Its key pharmacology:
- Approved indications: Inappropriate sinus tachycardia, HFrEF with sinus rhythm and HR ≥75 bpm
- Standard dose: 5–7.5 mg BD (not OD); 25 mg OD is non-standard — verify formulation
- Mechanism limitation: Ivabradine acts on the sinus node If channel. In focal atrial tachycardia (where the pacemaker is an ectopic focus, not the sinus node), ivabradine has limited or no direct effect on the tachycardia rate. It may have some indirect benefit if the AT is adenosine-sensitive or has triggered activity, but evidence is sparse.
In practice, ivabradine is used for inappropriate sinus tachycardia and not recommended as standard therapy for focal AT. Its use here may reflect an attempt to control residual elevated rates in conjunction with carvedilol, but this combination also carries a risk of excessive HR lowering and bradycardia.
Guideline-Based Treatment for Focal Atrial Tachycardia
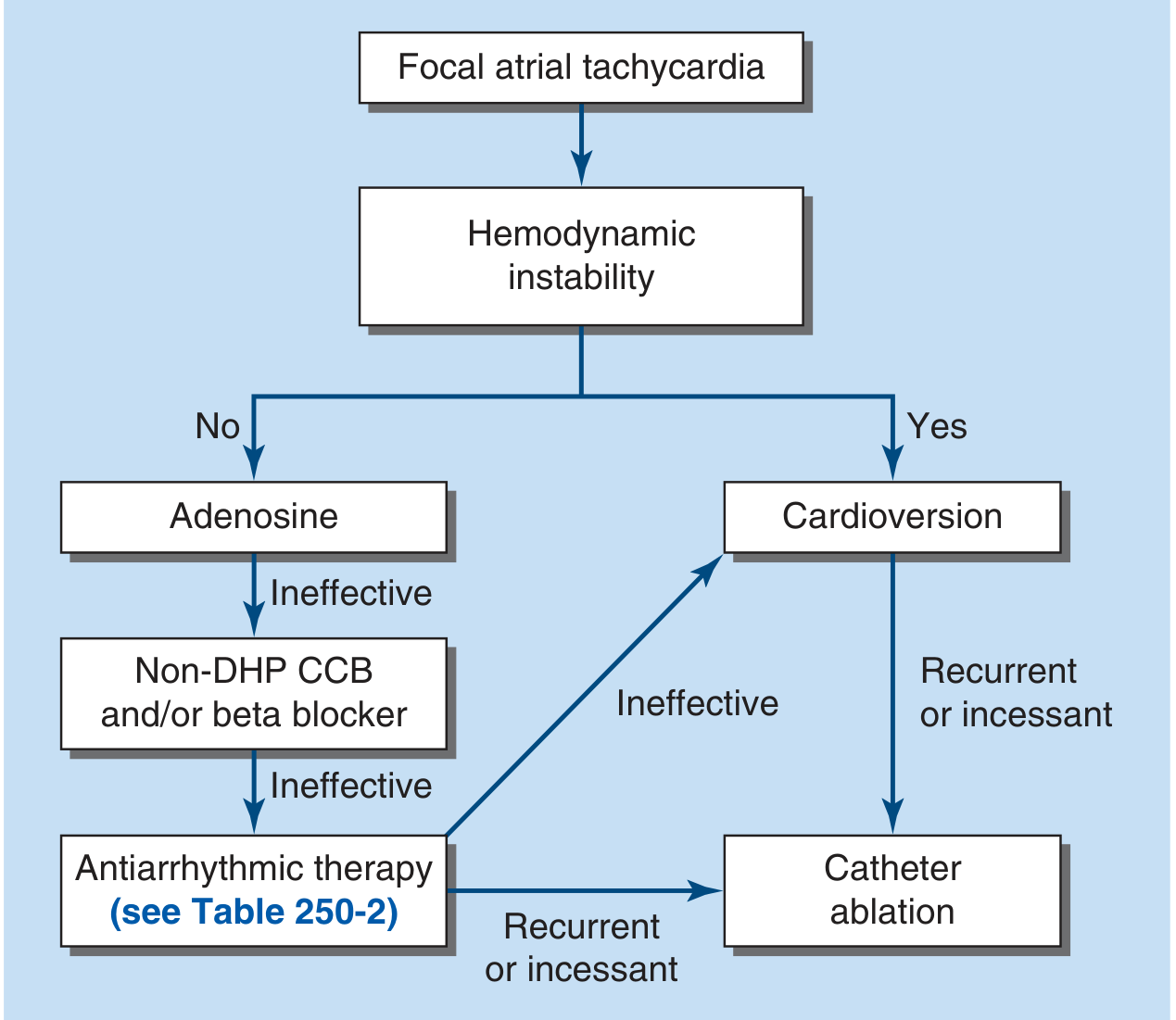
Harrison's Principles of Internal Medicine 22E — Treatment algorithm for focal atrial tachycardia
Hemodynamically stable (this patient):
| Step | Intervention |
|---|---|
| 1st line chronic | β-blockers (metoprolol 25–100 mg BD, bisoprolol 2.5–10 mg OD, carvedilol 6.25–25 mg BD) |
| Alternative 1st line | Non-DHP calcium channel blocker (diltiazem, verapamil) |
| If refractory | Membrane-active antiarrhythmics: flecainide, propafenone, sotalol, rarely amiodarone |
| Definitive therapy | Catheter ablation — highly effective, increasingly offered as first-line, especially if incessant AT |
"Electrical mapping and ablation of atrial tachycardia are highly effective and are increasingly offered as first-line therapy. Alternatively, atrial tachycardias can be managed with β-blockers (e.g., metoprolol starting at 25 mg twice daily), calcium channel blockers (e.g., diltiazem starting at 180 mg long-acting daily), or other antiarrhythmic drugs." — Goldman-Cecil Medicine
"Pharmacologic therapy with β-blockers or CCBs is effective in a proportion of patients. If these first-line medications fail, membrane active antiarrhythmic medications such as flecainide, propafenone, sotalol, or rarely amiodarone can be considered." — Fuster and Hurst's The Heart, 15th Edition
Key Clinical Concerns & Recommendations
| Issue | Action |
|---|---|
| Carvedilol 100 mg BD dose | Verify — likely a prescribing/transcription error; standard max is 25–50 mg BD |
| Ivabradine for AT | Limited evidence; ivabradine acts on sinus node, not ectopic foci — consider replacing with a non-DHP CCB if β-blocker alone insufficient |
| Combination bradycardia risk | High-dose carvedilol + ivabradine can cause dangerous bradycardia — monitor HR closely |
| Hypotension risk | Non-hypertensive patient on carvedilol (α-blocker) — monitor BP |
| LA dilatation | Repeat echo in 3–6 months; if LV dysfunction develops, this is tachycardia-induced cardiomyopathy — urgent rate control or ablation |
| Definitive therapy | Refer for electrophysiology study (EPS) + catheter ablation, especially given structural remodeling (LA dilatation) — ablation is increasingly first-line and curative |
| AF risk | LA dilatation increases risk of progression to atrial fibrillation — monitor with Holter |
Summary
This patient has focal atrial tachycardia with mild LA dilatation suggesting the arrhythmia is having hemodynamic consequences. The current regimen has dose/indication concerns that need verification. A β-blocker at appropriate dose is reasonable first-line pharmacotherapy, but given the LA remodeling and likelihood of incessant or recurrent AT, early referral for catheter ablation is strongly advised as it is curative in the majority of cases.
— Goldman-Cecil Medicine; Fuster and Hurst's The Heart, 15th Edition; Harrison's Principles of Internal Medicine 22E
Not carvedelol on Amiodarone 100bd next management should I continue the same
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Thank you for the correction. So the current regimen is:
- Amiodarone 100 mg BD (200 mg/day total)
- Ivabradine XL 25 mg OD
Revised Analysis: Amiodarone 100 mg BD + Ivabradine for Atrial Tachycardia
Is Amiodarone 100 mg BD Appropriate Here?
Yes, this is a reasonable maintenance dose. Amiodarone 200 mg/day (100 mg BD or 200 mg OD) is a well-recognised low maintenance dose for supraventricular arrhythmias:
"Many supraventricular arrhythmias can be managed successfully with daily dosages of 200 mg or less, whereas ventricular arrhythmias generally require higher doses. Adverse effects are less common at dosages of 200 mg/day or less but can still occur." — Braunwald's Heart Disease
Amiodarone is a Class III antiarrhythmic with Class I, II, and IV properties — it suppresses ectopic automaticity, triggered activity, and reentry, making it broadly effective for atrial tachycardia. It is generally used when β-blockers and CCBs have failed (which appears to be the case here), and is the most effective antiarrhythmic for maintaining sinus rhythm.
What About Ivabradine Here?
Ivabradine (If channel blocker, acts on sinus node) has limited direct evidence for focal atrial tachycardia. Its use is better established for inappropriate sinus tachycardia. That said:
- Some focal ATs (particularly those near the sinus node or with automaticity as the mechanism) may have partial If channel contribution
- At low amiodarone doses, ivabradine could supplement rate/rhythm control
- The main concern is additive bradycardia — both agents slow heart rate
Verify the ivabradine dose: Standard dosing is 5–7.5 mg BD. "Prominent XL 25 mg OD" — if this is a 25 mg modified-release tablet, confirm this is the intended formulation and dose, as it is non-standard.
Should You Continue the Same? — Clinical Decision Framework
| Question | Answer |
|---|---|
| Is the AT controlled (rate normal, symptoms resolved)? | If yes → Continue and monitor |
| Is the patient in sinus rhythm or still in AT? | If still in AT with normal rate, rhythm control (amiodarone) is working partially |
| Is there any bradycardia (HR <50)? | Combination risk — check resting ECG + Holter |
| LA dilatation improving on echo? | Repeat in 3–6 months; should regress if rate is controlled |
| Symptoms persisting? | Consider escalating or referring for ablation |
Recommendations Going Forward
Continue current regimen IF:
- Resting HR is controlled (60–80 bpm)
- Patient is asymptomatic or significantly improved
- No adverse effects (thyroid, pulmonary, liver)
Add/Change IF:
- AT is still incessant or frequently recurrent → refer for electrophysiology study + catheter ablation (>90% cure rate, increasingly first-line)
- Bradycardia developing → reduce or stop ivabradine first (lower evidence base for AT)
- Consider dropping ivabradine and replacing with a beta-blocker (metoprolol/bisoprolol) if rhythm control is not yet achieved, as the β-blocker + amiodarone combination has stronger evidence
Mandatory Monitoring on Long-Term Amiodarone
Even at 200 mg/day, amiodarone monitoring is non-negotiable:
| Parameter | Frequency |
|---|---|
| TFTs (TSH, T3, T4) | Every 3 months for first year, then 6-monthly |
| LFTs (AST, ALT) | 6-monthly |
| Chest X-ray | Baseline + annually (pulmonary toxicity) |
| PFTs with DLCO | Baseline; repeat if respiratory symptoms develop |
| ECG | Regularly — watch for QT prolongation, bradycardia |
| Eye review | If visual symptoms (corneal microdeposits in ~100% at 6 months, usually asymptomatic) |
| Serum electrolytes | Periodically (hypokalaemia raises TdP risk) |
| Echo | 3–6 months — assess LA size regression |
"Adverse effects are reported by about 75% of patients treated with amiodarone for 5 years, and these effects compel stopping the drug in 18–37%... Thyroid function tests should be performed approximately every 3 months for the first year." — Braunwald's Heart Disease
Bottom Line
Continue amiodarone 100 mg BD — appropriate maintenance dose for SVT/AT in a non-hypertensive patient with normal LV function. Re-evaluate ivabradine (ensure correct dose; consider stopping it if AT is well controlled on amiodarone alone, to avoid bradycardia).
The most important next step: assess whether the AT is truly suppressed (12-lead ECG + 24-hour Holter). If the arrhythmia persists or is incessant, the mild LA dilatation puts this patient at risk of tachycardia-induced cardiomyopathy, and early referral for catheter ablation (curative, >90% success) should be discussed with the patient.
— Braunwald's Heart Disease; Fuster and Hurst's The Heart, 15th Edition; Goldman-Cecil Medicine
Not ivabradine on Prolomet XL 25
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Thank you for the clarification. So the correct regimen is:
Amiodarone (Caesar One) 100 mg BD + Metoprolol succinate (Prolomet XL) 25 mg OD
Revised Analysis: Amiodarone 100 mg BD + Metoprolol Succinate 25 mg OD for Atrial Tachycardia
Is This a Rational Combination?
Yes — this is a clinically rational and commonly used combination, but requires careful monitoring.
| Drug | Role | Dose Assessment |
|---|---|---|
| Amiodarone 100 mg BD (200 mg/day) | Rhythm control — suppresses ectopic focus, prevents recurrence | ✅ Appropriate low maintenance dose for supraventricular arrhythmia |
| Metoprolol succinate XL 25 mg OD | Rate control + anti-adrenergic suppression of triggering | ✅ Appropriate low starting dose; can titrate to 50–100 mg OD |
Amiodarone has Class II (β-blocking) properties itself. Adding a β-blocker gives complementary rate control, particularly during breakthrough tachycardia or adrenergic surges. This combination is used in practice, especially when amiodarone alone has not fully controlled the rate.
Key Concern: Additive Bradycardia
Both amiodarone (intrinsic β-blockade + AV nodal slowing) and metoprolol slow heart rate and AV conduction. This combination can cause:
- Symptomatic bradycardia (HR <50 bpm)
- AV block (especially 1st or 2nd degree)
- Fatigue, dizziness, presyncope
Amiodarone interactions: "bradycardia and heart block in diseased heart" — Morgan & Mikhail's Clinical Anesthesiology
At metoprolol 25 mg OD, the risk is low but present. This is actually a conservative, well-chosen starting dose given the combination.
Should You Continue the Same Regimen?
Continue IF all of the following apply:
- Resting HR is 55–80 bpm (not bradycardic)
- ECG shows no AV block or PR prolongation >200 ms beyond baseline
- Patient is asymptomatic or significantly improved (fewer/no palpitations)
- Echo at follow-up shows LA dilatation stable or regressing
- No amiodarone side effects have emerged
Reassess/Modify IF:
| Scenario | Action |
|---|---|
| AT still incessant on Holter | Escalate metoprolol to 50 mg OD, or refer for catheter ablation |
| HR <55 or AV block on ECG | Reduce/stop metoprolol first (less critical than amiodarone for rhythm) |
| Symptoms persist despite both drugs | Electrophysiology referral for ablation — >90% cure rate |
| Amiodarone toxicity signs | Dose reduction or discontinuation |
| LA dilatation worsening on echo | Urgent rhythm control — reconsider ablation |
Next Steps — Practical Plan
- 12-lead ECG — check PR interval, QTc, baseline HR
- 24-hour Holter — assess AT burden, minimum HR, AV block
- Echocardiogram in 3 months — LA size regression confirms AT is controlled
- Amiodarone monitoring bloods (if not already done):
- TSH, T3, T4
- LFTs
- Chest X-ray + DLCO baseline
- Discuss catheter ablation — given that the patient needed a Class III antiarrhythmic (amiodarone) plus a β-blocker, this suggests the AT is not trivially controlled. Ablation offers definitive cure with >90% success and would allow stopping both drugs.
Bottom Line
Continue the current regimen — Amiodarone 100 mg BD + Metoprolol XL 25 mg OD is appropriate and well-dosed for this non-hypertensive patient with AT and mild LA dilatation. The most important next action is to confirm rhythm control with a Holter monitor and begin amiodarone toxicity surveillance. If the AT persists or is incessant, refer early for catheter ablation rather than escalating drug doses further.
— Braunwald's Heart Disease; Goldman-Cecil Medicine; Fuster and Hurst's The Heart, 15th Edition
How long to continue the same medication
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
There is no fixed duration — it is guided entirely by the clinical response, the nature of the arrhythmia, and amiodarone's cumulative toxicity profile. Here is the practical framework:
Duration of Amiodarone + Metoprolol in Atrial Tachycardia
The Core Principle
There is no predetermined stop date. Duration depends on three factors:
- Whether the AT is paroxysmal or persistent/incessant
- Whether the arrhythmia remits spontaneously or requires indefinite suppression
- The accumulating risk of amiodarone toxicity over time
"Some forms of atrial tachycardia are paroxysmal and may remit spontaneously without treatment." — Goldman-Cecil Medicine
Scenario-Based Duration Guide
| Clinical Scenario | Duration Strategy |
|---|---|
| AT controlled, paroxysmal pattern, no recurrence on Holter | Trial of dose reduction/weaning after 6–12 months of stable rhythm |
| AT incessant or recurrent, LA dilatation present | Continue until ablation is performed — do not attempt to stop prematurely |
| AT remits completely, LA size normalises on echo | Consider stopping metoprolol first, then slowly wean amiodarone (takes months to clear due to long half-life) |
| Patient declines ablation, AT recurring | Long-term indefinite therapy — but amiodarone toxicity risk accumulates significantly after 2–3 years |
The Amiodarone Toxicity Time Problem
This is the most important reason not to continue amiodarone indefinitely without reassessment:
- 75% of patients on amiodarone for 5 years develop adverse effects
- 18–37% require discontinuation due to toxicity
- Toxicity is dose- and duration-dependent — the longer and higher the dose, the greater the risk
- At 200 mg/day (this patient's dose), risk is lower but not absent
"In general, the lowest possible maintenance dose of amiodarone should be used to minimise the likelihood of adverse events." — Braunwald's Heart Disease
Practical Timeline for This Patient
NOW → 3 months
✓ 24-hr Holter — confirm AT burden
✓ Baseline amiodarone bloods (TFT, LFT, CXR, DLCO)
✓ Titrate metoprolol if HR still high (up to 50–100 mg OD)
3–6 months
✓ Repeat echo — is LA dilatation regressing?
✓ If AT controlled and asymptomatic → consider EPS + ablation discussion
✓ Amiodarone monitoring bloods
6–12 months (if stable, no ablation)
✓ Reassess whether AT is truly suppressed
✓ If sustained sinus rhythm for 6+ months → cautious trial of stepping down metoprolol
✓ Continue amiodarone monitoring every 4–6 months
Beyond 1–2 years
⚠️ Strongly favour definitive ablation over continuing amiodarone long-term
⚠️ Cumulative toxicity risk rises significantly
⚠️ If patient is a good candidate, ablation allows stopping BOTH drugs
When to Stop Each Drug
| Drug | Stop When |
|---|---|
| Metoprolol XL 25 mg | AT well controlled for 6–12 months, HR stable, no tachycardia recurrence; taper gradually |
| Amiodarone 100 mg BD | After ablation (confirmed success), or after sustained remission — must taper slowly (half-life 40–55 days; tissue clearance takes months) |
Bottom Line
Continue both medications for at least 6–12 months, reassessing rhythm control with Holter at 3 months and echo at 3–6 months. Given that this patient already has LA dilatation (structural consequence of the arrhythmia) and required amiodarone (a last-resort antiarrhythmic), catheter ablation should be the target end-point — it would allow stopping both drugs permanently and eliminates the long-term amiodarone toxicity risk.
Do not continue amiodarone beyond 2 years without a formal review of whether ablation can replace it.
— Braunwald's Heart Disease; Goldman-Cecil Medicine; Fuster and Hurst's The Heart, 15th Edition
This is a shared conversation. Sign in to Orris to start your own chat.