Corneal ulcer
"corneal ulcer" OR "infectious keratitis"
corneal ulcer hypopyon slit lamp
Corneal Ulcer (Ulcerative Keratitis)
Definition & Pathophysiology
- Trauma or corneal abrasion becoming secondarily infected
- Contact lens wear (especially extended-wear/overnight)
- Desiccation from incomplete lid closure (e.g., Bell's palsy → exposure keratitis)
- Immunosuppression (topical/systemic steroids, systemic immunosuppressants)
Etiology / Causative Organisms
| Category | Organisms |
|---|---|
| Bacteria | Pseudomonas aeruginosa (contact lenses), S. pneumoniae, Staphylococcus spp., Moraxella spp. |
| Viruses | Herpes simplex virus (most common cause of central corneal ulcer), Varicella-zoster virus |
| Fungi | Candida, Aspergillus, Penicillium, Fusarium, Acremonium |
| Acanthamoeba | Contact lens wearers, contaminated water |
| Mycobacteria / Nocardia | Post-refractive surgery, trauma |
- Pseudomonas → contact lens wearers
- Fungal → corticosteroid drop users, agricultural workers (vegetation/soil inoculation)
- HSV → most common cause requiring corneal transplant in the USA
- Acanthamoeba → contact lens wearers swimming or using tap water
Clinical Features
- Ocular pain / foreign body sensation
- Photophobia (often consensual — ciliary spasm from associated iritis)
- Redness, tearing, mucopurulent discharge
- Blurred or decreased vision (if ulcer is in the visual axis, or if uveitis is present)
- Eyelid/conjunctival erythema, mucopurulent discharge
- Corneal ulcer: round or irregular white/hazy base with heaped-up edges and stromal infiltration due to WBC infiltration
- Associated iritis: miotic pupil, ciliary flush
- Slit-lamp: flare and cells in anterior chamber
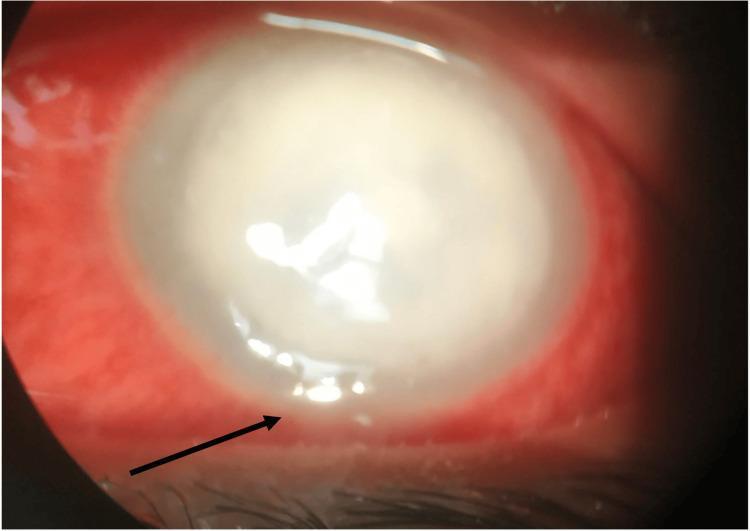
- Hypopyon (layering of inflammatory cells in the inferior anterior chamber) — indicates severe inflammation/infection
Clinical Images
Diagnosis
- Clinical — slit-lamp examination is the cornerstone
- Fluorescein staining — ulcer has "heaped-up" edges (vs. flat abrasion), with stromal edema/whitening
- Corneal scraping — should be performed in most cases; sent for:
- Gram stain (bacteria, fungi)
- Giemsa stain (bacteria, Acanthamoeba)
- Calcofluor white (Acanthamoeba, fungi — requires fluorescent microscope)
- Acid-fast stain (Mycobacteria, Nocardia)
- Culture & sensitivity
TIP: The causative organism cannot be reliably determined from the morphological appearance of the ulcer alone. Empirical broad-spectrum treatment is started before culture results return.
Management
General Measures
- Discontinue contact lens wear immediately (mandatory)
- Protective eye shield if significant corneal thinning or perforation risk
- Emergent ophthalmology consultation — corneal ulcers can rapidly progress to permanent vision loss
- Consider hospital admission for: aggressive disease, an only eye, poor compliance
Antibiotic Treatment
- Fluoroquinolone monotherapy — ciprofloxacin or ofloxacin 1 drop every hour day and night for 24–48 h, then tapered
- Alternatively: moxifloxacin or gatifloxacin (newer-generation; better Gram-positive coverage, superior penetration)
- Duotherapy (aggressive disease or suspected streptococci): fortified cephalosporin + fortified aminoglycoside (e.g., cefuroxime 5% + gentamicin 1.5%)
| Isolate | Agent |
|---|---|
| Gram-positive cocci | Cefuroxime 0.3%, vancomycin 5%, or teicoplanin 1% |
| Gram-negative rods | Fortified gentamicin 1.5% or fluoroquinolone |
| Gram-negative cocci | Ceftriaxone 5% or ceftazidime |
| Mycobacteria | Amikacin 2% or clarithromycin 1% |
| Nocardia | Amikacin 2% or TMP-SMX |
TIP: Fluoroquinolones have limited activity against Gram-positive organisms, particularly Streptococcus. Ciprofloxacin drops can cause white corneal precipitates that may delay re-epithelialization.
Antifungal Treatment
- Natamycin (first-line for filamentous fungi)
- Amphotericin B or fluconazole (Candida/yeasts)
- Topical steroids are contraindicated when fungal infection is suspected
Antiviral Treatment
- HSV keratitis: Topical ganciclovir 0.15% gel (3–5×/day) or trifluridine 1% (5–9×/day × 14 days); systemic acyclovir/valacyclovir for severe or refractory cases. Avoid topical steroids (worsen HSV infection)
- HZV keratitis: Systemic therapy is standard — acyclovir 800 mg 5×/day, or valacyclovir 1000 mg 3×/day × 7–10 days. Treat within 72 hours of rash onset to reduce acute pain and ocular complications
Adjunctive
- Cycloplegics (cyclopentolate 1%, homatropine 2%, atropine 1%) — prevent posterior synechiae, reduce ciliary spasm pain
- Systemic antibiotics indicated for: N. meningitidis (life-saving — IM benzylpenicillin/ceftriaxone), N. gonorrhoeae (ceftriaxone), H. influenzae (amoxicillin-clavulanate), threatened corneal perforation (ciprofloxacin + doxycycline for anti-collagenase effect)
- Steroids (topical): controversial; reduce scarring but promote fungal/mycobacterial/HSV replication; use only after infection is controlled under specialist supervision
Complications
- Corneal perforation — may require bandage contact lens, tissue glue, or penetrating keratoplasty/patch graft
- Endophthalmitis
- Corneal scarring → permanent visual impairment
- Treatment failure — if no improvement in 24–48 h, review cultures; if still failing after a further 48 h, suspend treatment and re-scrape on broader media; consider corneal biopsy
- Consider PACK-CXL (photoactivated chromophore-enhanced collagen cross-linking) if corneal melting or antibiotic resistance is suspected
Disposition
Recent Evidence
Gradual loss of visiion, Hyphema
hyphema management treatment
hyphema blood anterior chamber eye
Part 1: Gradual Loss of Vision
Differential Diagnosis by Pattern
| Diagnosis | Pain | RAPD | Fundus | Key Features |
|---|---|---|---|---|
| Cataract | No | ± | Unable to visualize | Lens opacity; gradual, painless bilateral |
| Chronic open-angle glaucoma | No | ± | Optic cup enlargement | Peripheral field loss first; bilateral; ↑IOP |
| Diabetic retinopathy | No | ± | Microaneurysms, hemorrhages, neovascularization | Bilateral; history of diabetes |
| Age-related macular degeneration | No | No | Drusen (dry); neovascular membrane (wet) | Central vision loss; elderly; bilateral |
| Optic neuritis | Yes (with EOM) | Yes | Papilledema or normal | Young female; associated with MS; gradual over days |
| Ischemic optic neuropathy | No | Yes | Swollen pale disc | GCA (>50 y/o), jaw claudication, ↑ESR |
| Giant cell arteritis | Retro-orbital ± | Yes | Normal or pale disc | Headache, myalgias, scalp tenderness |
| Uveitis | Yes | No | Normal | AC flare & cells, ciliary flush, photophobia |
| Toxic/nutritional optic neuropathy | No | Bilateral | Optic atrophy (late) | Cecocentral scotoma; dyschromatopsia; ethambutol, amiodarone, B12 deficiency |
| Chronic papilledema | No | Variable | Papilledema | Raised ICP; nasal field defects → constriction |
| Radiation retinopathy | No | Variable | Resembles diabetic retinopathy | History of periocular or cranial irradiation |
| Cortical blindness | No | ± | Possible papilledema | Bilateral; homonymous hemianopsia |
| Tumour / compressive optic neuropathy | Variable | Yes | Optic atrophy | Pituitary adenoma → bitemporal hemianopsia |
Causes of Progressive Visual Loss (Neurology perspective)
- Glaucoma: Arcuate visual field defects; central vision spared until late; bilateral/symmetric; ↑IOP and optic disc cupping
- Chronic papilledema: Nasal defects first → progressive constriction; central vision late
- Toxic optic neuropathy: Gradual onset over weeks–months; cecocentral scotomas; prominent dyschromatopsia; optic atrophy develops late. Common culprits: ethambutol, amiodarone, linezolid
- Retinal toxins: Vigabatrin, chloroquine/hydroxychloroquine, phenothiazines, digitalis → painless progressive binocular loss
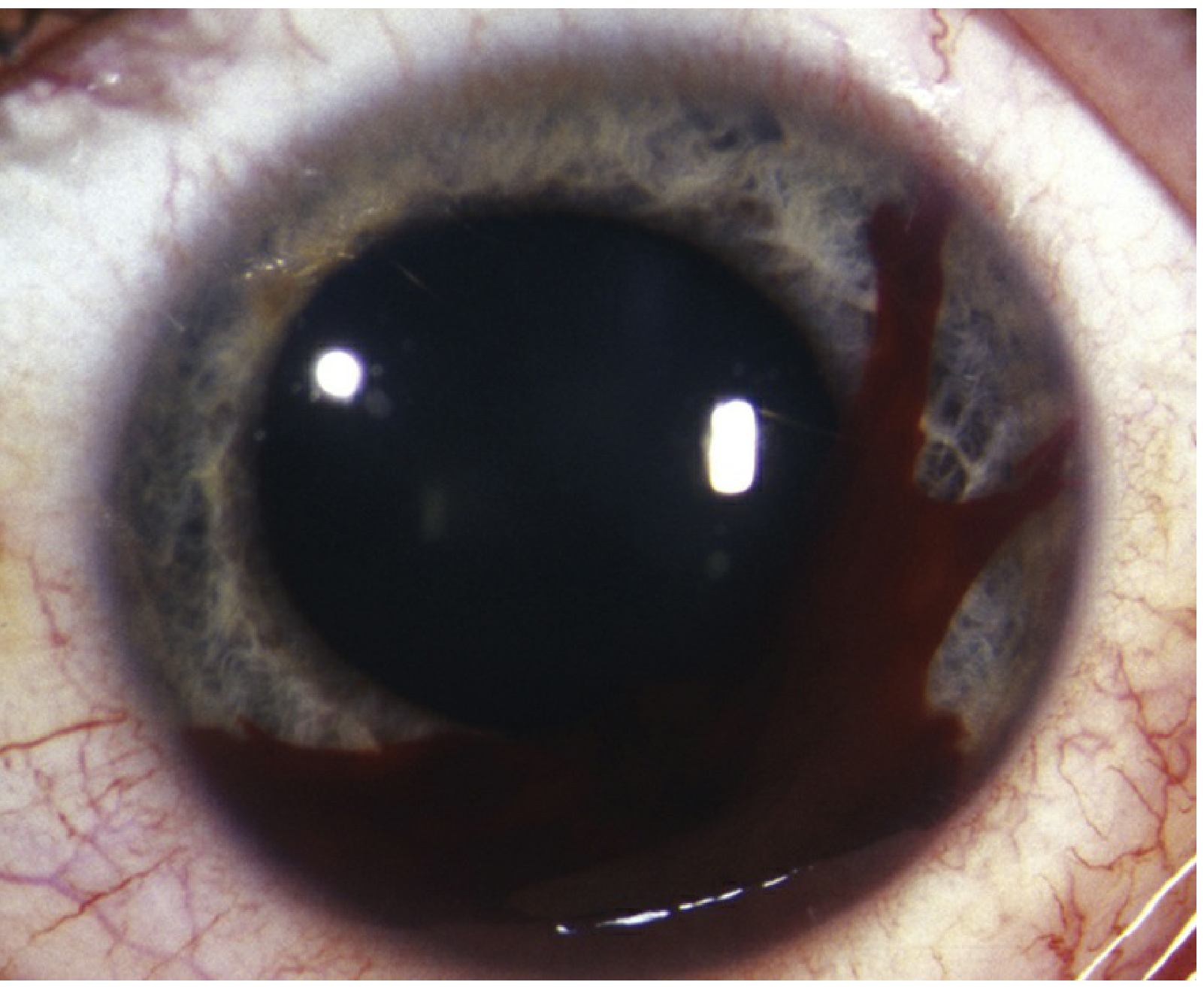
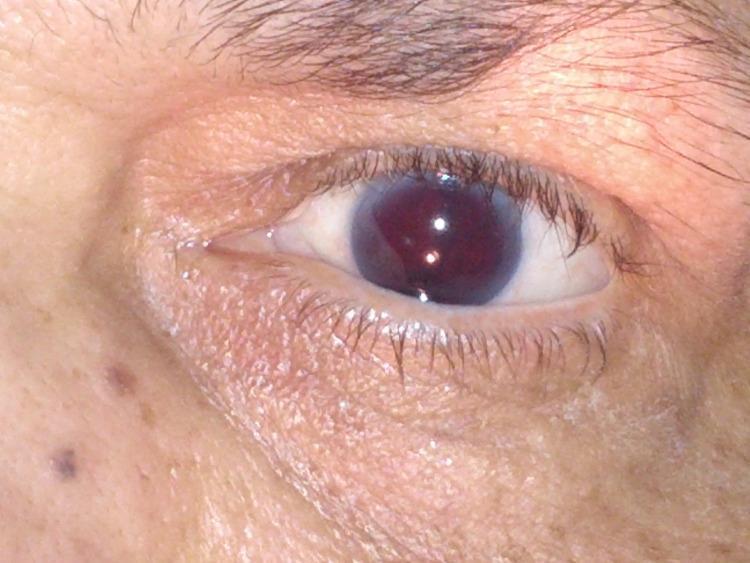
Part 2: Hyphema
Definition
Classification
| Grade | AC Fill |
|---|---|
| I | <1/3 |
| II | 1/3 – 1/2 |
| III | >1/2 |
| IV (Total) | 100% — may be red or "8-ball/blackball" (deoxygenated, dark) |
Clinical Images
Etiology
Traumatic (most common)
- Blunt or penetrating trauma → rupture of iris root vessel
- Maximal visual compromise is usually at the time of injury; decreasing vision over time suggests rebleed or continued bleeding (causing IOP rise)
Spontaneous / Non-traumatic
- Iris neovascularization (rubeosis iridis) from: diabetes, central retinal vein occlusion, ocular ischemic syndrome, chronic uveitis
- Blood dyscrasias / coagulopathies
- Anticoagulant use (aspirin, warfarin, clopidogrel, NSAIDs, ethanol)
- Iris–IOL chafing (post-cataract surgery)
- Herpetic keratouveitis
- Neoplasms: iris/ciliary body melanoma, retinoblastoma, leukemia, juvenile xanthogranuloma
- Fuchs heterochromic iridocyclitis
- Post-surgical (usually self-limited)
Symptoms
- Pain, blurred vision
- History of trauma (or spontaneous — as above)
- Transient vision clouding with microhyphema (intermittent bleeds)
Workup
- History: Mechanism/force/direction of injury; anticoagulant use; personal/family history of sickle cell disease or trait (critical — alters management); coagulopathy symptoms
- Ocular exam: First rule out ruptured globe. Measure IOP. Document extent of hyphema (height in mm). Dilated fundus exam (no scleral depression). B-scan ultrasound if fundus view poor
- CT orbits/brain (axial, coronal, parasagittal, 1-mm cuts) if: suspected orbital fracture, IOFB, or loss of consciousness
- Sickledex screen (hemoglobin electrophoresis if necessary) — screen all appropriate patients
- Spontaneous hyphema additional workup: PT/INR, PTT, CBC + platelets, bleeding time, proteins C and S; UBM (evaluate IOL haptic position, ciliary body masses); fluorescein angiogram of iris; gonioscopy (to evaluate angle neovascularization or masses)
Complications
| Complication | Mechanism |
|---|---|
| ↑ IOP | RBCs mechanically plug trabecular meshwork |
| Rebleeding | Occurs in 0.4–35%, typically 2–7 days post-injury (up to 5–10 days) |
| Corneal blood staining | Especially with total hyphema + elevated IOP |
| Peripheral anterior synechiae (PAS) | Prolonged hyphema → angle closure |
| Optic atrophy | Sustained high IOP |
| Accommodative impairment | Ciliary body injury |
Treatment
Activity & Environment
- Bed rest with bathroom privileges OR limited activity; elevate head of bed to 45° (blood settles inferiorly, clears trabecular meshwork, reduces IOP)
- Rigid eye shield at all times — do NOT patch (prevents recognition of sudden vision change from rebleed)
- Consider hospitalization for: noncompliant patients, bleeding diathesis, sickle cell disease/trait, severe associated ocular injuries, children at risk for amblyopia, suspected child abuse
Medications
| Agent | Indication/Notes |
|---|---|
| Cycloplegics | Cyclopentolate 1–2% or homatropine 5% b.i.d.–t.i.d., or atropine 1% q.d.–b.i.d.; prevents synechiae, reduces pain |
| Topical steroids (prednisolone acetate 1% q.i.d.–q1h) | Only if signs of iritis (photophobia, ciliary flush), fibrin/WBCs in AC, or lens capsule rupture; taper quickly — risk of steroid-induced glaucoma and cataract (especially in children) |
| Analgesics | Acetaminophen only; avoid aspirin, NSAIDs (antiplatelet effect promotes rebleeding) |
| Antifibrinolytics | Aminocaproic acid or tranexamic acid — decrease rebleeding rate; evidence inconclusive for topical forms; systemic aminocaproic acid rarely used now |
| Antiemetics | Ondansetron p.r.n. if hospitalized |
IOP Management
- Beta-blocker (timolol or levobunolol 0.5% b.i.d.)
- Add alpha-agonist (brimonidine 0.1–0.2% or apraclonidine 0.5% t.i.d.) or topical CAI (dorzolamide 2% or brinzolamide 1% t.i.d.) — avoid prostaglandin analogues and miotics (increase inflammation)
- If topical fails: acetazolamide up to 500 mg p.o. q12h (adults) or mannitol 1–2 g/kg IV over 45 min
- Beta-blocker first
- Extreme caution with all other agents: dorzolamide/brinzolamide may ↓ aqueous pH → increased sickling; alpha-agonists affect iris vasculature; avoid systemic diuretics (induce acidosis/dehydration → increased sickling)
- AC paracentesis as temporizing measure if medical management fails
Surgical Evacuation — Indications
- Corneal stromal blood staining (especially children)
- Significant visual deterioration
- Hyphema not decreasing to ≤50% by 8 days (prevents PAS)
- IOP ≥60 mmHg for ≥48 h despite maximal medical therapy (prevents optic atrophy)
- IOP ≥25 mmHg with total hyphema for ≥5 days (prevents corneal staining)
- Sickle cell: IOP ≥24 mmHg for ≥24 h, or any transient IOP ≥30 mmHg
- Children at risk for amblyopia
Follow-Up
- Daily after initial trauma: check VA, IOP, slit lamp (look for new bleeding, corneal staining, PAS, iridodialysis, lens subluxation, cataract as blood clears)
- Return immediately for sudden ↑ pain or ↓ vision (rebleed or IOP spike)
- After initial period: transition to long-acting cycloplegic (atropine 1%); taper steroids as blood/fibrin/WBCs resolve
- Protective glasses recommended after recovery
Key Clinical Points
A hyphema laying out posteriorly when the patient is supine may only become visible when sitting upright.
Rebleeding is the most feared early complication — occurs in up to 30% of cases, typically 3–5 days post-trauma, and can cause severe IOP elevation requiring surgical washout.
Sickle cell patients need a lower IOP threshold for intervention (≥24 mmHg vs. ≥30 mmHg) and require careful agent selection due to sickling risk.
An 8 year old girl with insidious onset of swelling of left knee and pain as seen by a pediatrician who noted an irregular pupil in the course of her examination and referred to an Ophthalmologist to rule out ocular involvement
"juvenile idiopathic arthritis" AND uveitis
Clinical Diagnosis: JIA-Associated Chronic Anterior Uveitis
The Clinical Picture
| Feature | Significance |
|---|---|
| 8-year-old girl | Female predominance (F:M = 5:1); oligoarticular JIA peaks at 2–4 years but extends well into middle childhood |
| Insidious knee swelling | Large lower-extremity joint = oligoarticular JIA pattern |
| Single joint involved | ≤4 joints = oligoarticular subtype (most common, 40–50% of JIA) |
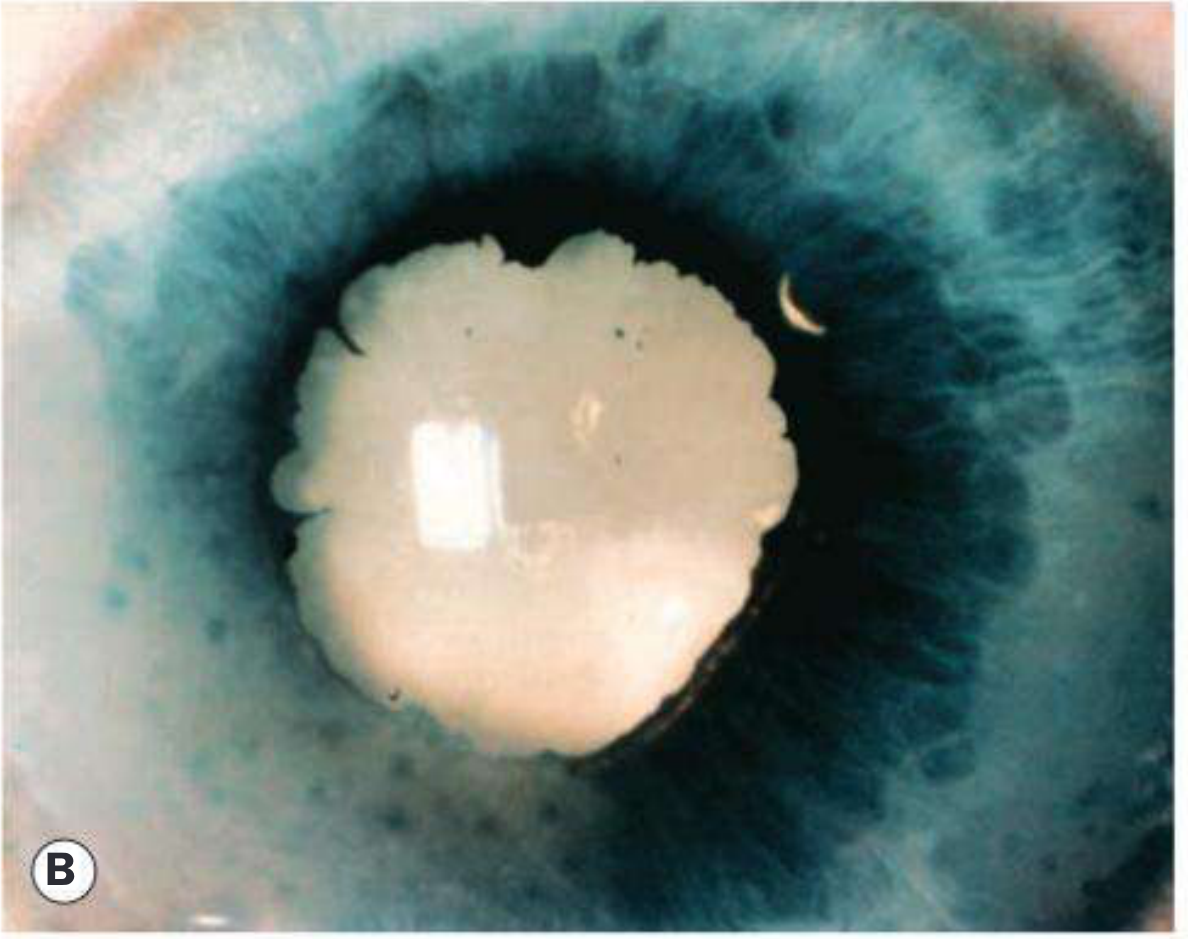
| Irregular pupil | Posterior synechiae (PS) — iris adhesions to the anterior lens capsule from chronic uveitis — distort the pupil shape |
| No eye symptoms | JIA uveitis is characteristically asymptomatic — the "white quiet eye" |
| Referred for ocular exam | Correct — this is a mandatory screening situation |
The uveitis of JIA is particularly dangerous because it is invariably asymptomatic and must generally be detected by screening with slit-lamp examination. Even during acute exacerbations with +4 aqueous cells, it is rare for patients to complain. — Kanski's Clinical Ophthalmology, p. 460
JIA: Classification (ILAR)
| Subtype | Prevalence | Demographics | Joints | Uveitis Risk |
|---|---|---|---|---|
| Oligoarticular (40–50%) | Most common | F >> M; peak 2–4 yr | ≤4 joints; knees & ankles | 20–30% (highest) |
| Polyarticular RF-neg (20–35%) | — | F > M; bimodal | ≥5 small + large joints | 4–10% |
| Polyarticular RF-pos (<10%) | — | F > M; 9–12 yr | Symmetric polyarthritis | 2% |
| Systemic / Still's (5–15%) | — | M = F | Oligo/poly; knees, wrists | 1% (rare) |
| Enthesitis-related (10–15%) | — | M > F; 9–12 yr | Lower limb + axial | 7% (acute, symptomatic) |
| Psoriatic (5–10%) | — | F > M | Wrists + small joints | 10% |
- Uveitis prevalence in persistent oligoarticular JIA: 16%; in extended oligoarticular: 25%
- ANA-positive in 60–70% of oligoarticular JIA → strong independent risk factor for uveitis
Ocular Findings in JIA-Associated Uveitis
Clinical Images

Slit-Lamp Findings (What the Ophthalmologist Should Look For)
| Sign | Description |
|---|---|
| Aqueous cells & flare | Chronic non-granulomatous inflammation; "dusting" of the entire endothelium with cells during exacerbations |
| Posterior synechiae (PS) | Iris adhesions to anterior lens capsule → irregular pupil (the sign that triggered this referral) |
| Keratic precipitates (KP) | Fine, non-granulomatous; NOT mutton-fat (those suggest sarcoid/TB) |
| Band keratopathy | Calcium deposits in Bowman's layer, interpalpebral zone — horizontal white band |
| Cataract | Posterior subcapsular; from chronic inflammation or steroid use |
| Hypopyon | Absent (distinguishes from HLA-B27 uveitis) |
| Conjunctival injection | Usually absent even with severe disease — the "white quiet eye" |
| Secondary glaucoma | Elevated IOP from trabecular inflammation/PAS |
| Cystoid macular oedema (CME) | Serious vision-threatening complication |
| Amblyopia | Risk in younger children, especially with media opacity or anisometropia |
Injection is usually absent even in the presence of severe uveitis. Both eyes are affected in 70% with symmetrical severity. — Kanski's Clinical Ophthalmology, p. 461
Why the Irregular Pupil?
Investigations
Ophthalmic
- Slit-lamp examination — mandatory; only way to detect and grade activity
- Measure IOP (glaucoma screening)
- Dilated fundus exam (CME, posterior involvement)
Systemic / Laboratory
| Test | Significance |
|---|---|
| ANA | Positive in 60–75% of oligoarticular JIA; marker of high uveitis risk |
| RF (rheumatoid factor) | Usually negative in oligoarticular; positive in RF+ polyarticular subtype |
| HLA-B27 | Positive in enthesitis-related JIA; also acute anterior uveitis |
| ESR, CRP | Markers of systemic inflammation |
| CBC | Baseline; anaemia of chronic disease |
| LFTs, renal function | Baseline before DMARDs/methotrexate |
Risk Stratification for Uveitis
- Oligoarticular subtype
- Female sex
- ANA-positive
- Age of onset < 7 years
- Duration of arthritis < 4 years (uveitis most commonly develops early)
Arthritis usually antedates the diagnosis of uveitis. The irregular pupil in this child means uveitis has already been silently active long enough to form synechiae.
Ophthalmology Screening Protocol
| JIA Subtype | Screening Interval |
|---|---|
| Oligoarticular (all), psoriatic, polyarticular RF-neg, enthesitis-related — new diagnosis | Initial exam within 6 weeks; then every 2 months × 6 months |
| Ongoing higher-risk patients | Every 3–4 months |
| Lower-risk / stable | Every 6 months |
| Systemic JIA, polyarticular RF-positive | At minimum an initial screening exam; annually |
| At discharge from screening | Weekly self-monitoring of monocular vision; annual optometrist review |
Visual symptoms or suspicion of ocular signs (synechiae, cataract, band keratopathy) should lead to urgent ophthalmological referral and slit-lamp examination within a week.
Treatment
Ocular Management (Step-Up)
| Step | Agent | Notes |
|---|---|---|
| 1st line | Topical corticosteroids (prednisolone acetate 1%) | Effective in ~80% initially; taper to avoid steroid-induced glaucoma and cataract |
| Adjunct | Cycloplegics (cyclopentolate — short-acting preferred) | Prevent synechiae formation; avoid prolonged use in young children (amblyopia risk in monocular treatment) |
| 2nd line | Periocular steroids (subtenon triamcinolone) | Unilateral cases or steroid-sparing |
| Systemic | Oral corticosteroids | For severe disease; short courses |
| DMARD | Methotrexate (MTX) | First-line systemic immunosuppressive; reduces uveitis frequency |
| Biologic | Adalimumab (anti-TNF) | Most evidence in JIA uveitis; often used with MTX — reduces recurrence |
| Biologic | Infliximab (anti-TNF) | Second biologic option |
| Biologic | Tocilizumab (anti-IL-6) | For refractory uveitis |
| ⚠️ AVOID | Etanercept | Anti-TNF but can worsen ocular inflammation — contraindicated |
Complication-Specific Management
- Secondary glaucoma: Topical IOP-lowering agents; if refractory → trabeculectomy with mitomycin C (better outcomes with systemic anti-TNF) or Baerveldt implant
- Cataract: Surgical extraction with IOL implantation (now favoured over aphakia); outcomes generally good with controlled inflammation
- Band keratopathy: EDTA chelation
- CME: Periocular steroid injection; systemic immunosuppression
- Amblyopia: Patching therapy; optical correction
Key Points for This Patient
- The irregular pupil = posterior synechiae — uveitis has been active and undetected
- Slit-lamp exam urgently to grade activity, document complications, measure IOP
- ANA test — if positive, confirms highest-risk profile
- Refer to paediatric rheumatologist for systemic JIA management
- Bilateral slit-lamp screening even though only one eye visibly affected — 70% of JIA uveitis is bilateral
- Start topical steroids + cycloplegic; escalate to MTX ± adalimumab early if needed
- Screen for amblyopia — she is still within the amblyogenic age window
Recent Evidence
- PMID 41314670 (2025 Systematic Review, RMD Open): Long-term outcomes of JIA-associated uveitis — confirms visual morbidity risk and importance of early immunomodulation
- PMID 41945858 (2026 Meta-analysis, Ocular Immunol Inflamm): Adalimumab + methotrexate combination is effective and safe for JIA-associated uveitis — supports early biologic use
- PMID 41728909 (2026 Practice Guideline, PANLAR): Recommendations for oligoarticular JIA treatment including uveitis screening

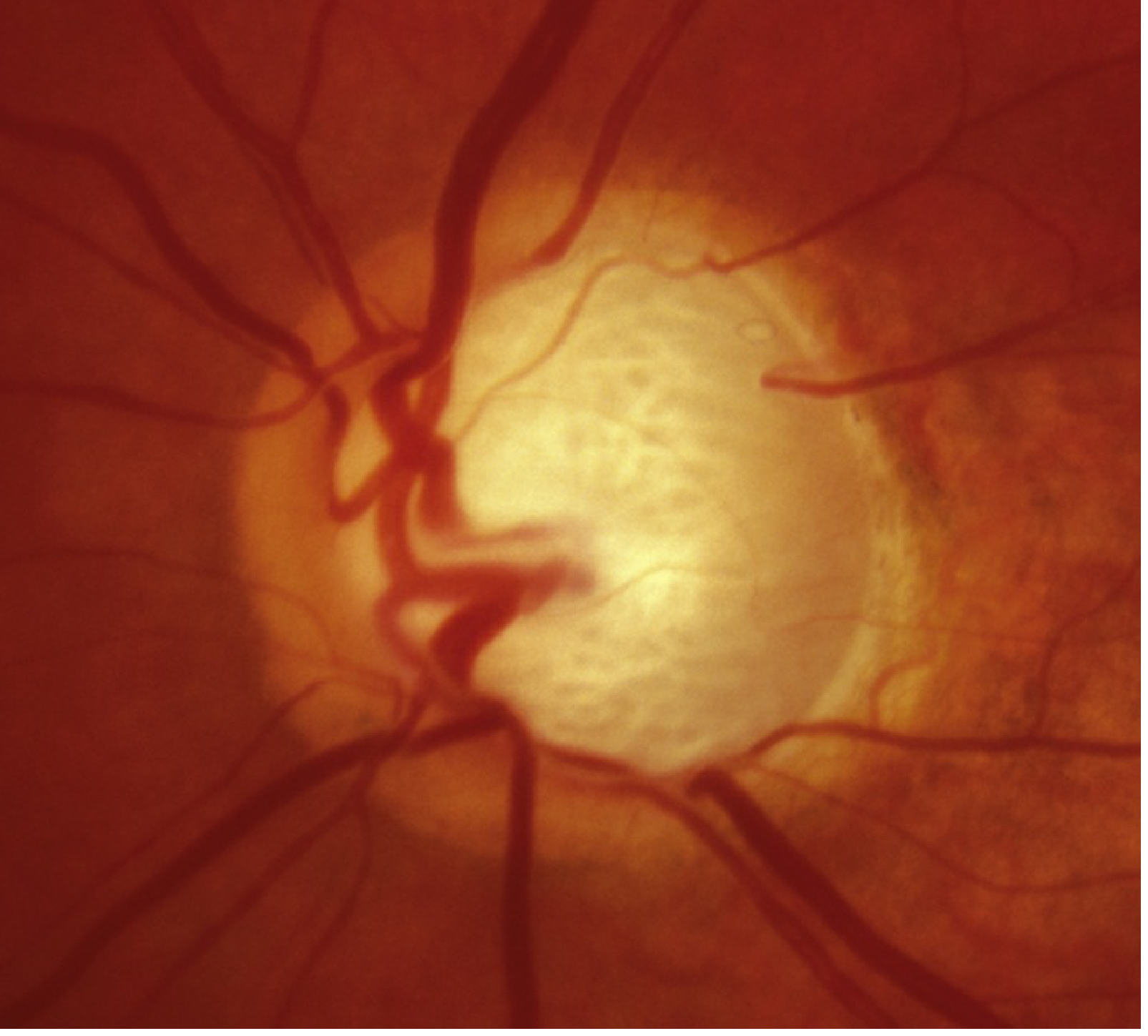
A 65 year old diabetic lady comes for her routine ophthalmic check up. On fundoscopy you detect asymmetrical enlargement of the cup: disc ratio (RE = 0.4; LE = 0.7). There are no changes suggestive of diabetic retinopathy. Picture below shows the optic disc of the left eye:
"open angle glaucoma" AND "cup disc ratio" AND diagnosis
Clinical Analysis: Asymmetric Cup-Disc Ratio in a Diabetic Patient
Interpretation of the Clinical Image
- A large, pale, deeply excavated optic cup occupying the majority of the disc
- Markedly thinned neuroretinal rim (NRR), particularly inferiorly and superiorly
- Bayoneting of vessels as they exit the disc
- The cup appears to fill approximately 0.7 of the disc diameter — consistent with the reported CDR of 0.7
- No haemorrhages or diabetic changes
Q1: Significance of the Optic Disc Findings
Cup-to-Disc Ratio (CDR)
- The CDR measures the diameter of the central pale cup relative to the total disc diameter (vertical ratio is standard)
- Normal CDR: generally ≤0.5; only 2% of the population have a CDR >0.7
- The vertical CDR is more sensitive — inferior and superior NRR are lost earliest in glaucoma
This Patient's Findings
| Finding | Value | Significance |
|---|---|---|
| RE CDR | 0.4 | Within normal range |
| LE CDR | 0.7 | Enlarged — suspicious for glaucoma |
| Asymmetry | 0.3 | Highly significant — asymmetry ≥0.2 is found in ~25% of glaucoma patients vs ~5% of normals |
A vertical cup/disc ratio asymmetry of 0.2 or more is found in about 5% of normal individuals and in about 25% of those with glaucoma. — Kanski's Clinical Ophthalmology, p. 367
ISNT Rule (Normal NRR)
- Violation of this rule (especially inferior notching) is a key indicator of glaucomatous damage
- In this patient's left eye, inferior > superior NRR loss is the likely pattern
Q2: Provisional Diagnosis
Primary Open-Angle Glaucoma (POAG)
- Retinal nerve fibre layer (RNFL) thinning
- Glaucomatous optic nerve damage (as seen)
- Characteristic visual field loss (as damage progresses)
- Open anterior chamber angle
- Absence of secondary glaucoma or non-glaucomatous cause
Why this patient fits POAG:
- Age 65 — prevalence of POAG is ~6% in White, ~16% in Black populations >70 years
- Diabetes — associated with glaucoma risk (though longitudinal studies are mixed, clinic-based studies show higher prevalence)
- Asymptomatic — POAG is typically silent until late
- Asymmetric CDR with LE > RE — unilateral/asymmetric progression is characteristic
- CDR 0.7 LE — enlarged cup with thinned rim
- No diabetic retinopathy — rules out diabetic optic disc change (rare) as confounding cause
POAG is the most prevalent type of glaucoma in people of European and African ethnic origin. It is a chronic, progressive optic neuropathy. IOP is a key modifiable risk factor. — Kanski's Clinical Ophthalmology, p. 363
Q3: Risk Factors in This Patient
| Risk Factor | Present? |
|---|---|
| Age (>60) | ✅ |
| Diabetes mellitus | ✅ |
| Asymmetric CDR | ✅ |
| Vascular disease risk | ✅ (diabetes → poor ocular perfusion) |
| Family history | Unknown |
| Myopia | Unknown |
| Race | Unknown |
Q4: Essential Investigations
1. Applanation Tonometry (IOP measurement)
- Goldmann applanation tonometry — gold standard
- Normal range: 10–21 mmHg; however, nearly half of POAG patients have IOP ≤21 mmHg at any screening
- Intraocular pressure >21 mmHg on more than one occasion, or a circadian variation of more than 5 mmHg is significant
- Inter-eye asymmetry >5 mmHg is suspicious even within normal range
- Must be measured at different times of day (diurnal variation)
2. Visual Field Testing (Perimetry)
- Humphrey automated visual field (24-2 or 30-2 strategy) — essential
- Characteristic patterns:
- Nasal step (earliest)
- Paracentral scotoma
- Arcuate scotoma (Bjerrum scotoma) — extends from blind spot superiorly or inferiorly
- Altitudinal defect
- Central vision spared until late in the disease
3. Gonioscopy
- To confirm open anterior chamber angle (excludes angle closure)
- Assess trabecular meshwork pigmentation
- Rule out secondary causes: peripheral anterior synechiae, pseudoexfoliation, pigment dispersion
4. Slit-Lamp Examination
- Exclude secondary glaucoma features: pseudoexfoliation material, pigment dispersion, rubeosis iridis, anterior uveitis
- Assess cornea for microcystic oedema (differentiates from PACG)
5. Central Corneal Thickness (CCT)
- Average CCT: 535–545 μm
- Thin cornea (<520 μm) → underestimates true IOP (applanation tonometry reads falsely low)
- Thin CCT is an independent risk factor for POAG development
- Essential for interpreting IOP values accurately
6. Optic Disc Documentation & Imaging
- OCT (Optical Coherence Tomography) — of the:
- RNFL (peripapillary) — detects thinning before visual field loss
- Ganglion cell complex (GCC) at macula — early detection
- Optic nerve head morphology
- Stereoscopic disc photographs (baseline documentation)
- Sensitivity and specificity up to 90% compared to normative database
7. Nerve Fibre Layer Analysis
- Detects RNFL defects (inferior > superior, corresponding to superior > inferior VF loss)
- Progression analysis: widening or deepening of established defects confirms active disease
All patients with suspected glaucoma should have: complete ocular exam including visual acuity, pupillary assessment for RAPD, confrontational visual fields, slit lamp, applanation tonometry, gonioscopy, and dilated fundus examination with special attention to the optic nerve. — Wills Eye Manual, p. 552
Q5: Management
Treatment Goal
Step-Up Medical Treatment
| Class | Agent | Dose | Notes |
|---|---|---|---|
| Prostaglandin analogues (1st line) | Latanoprost 0.005%, Bimatoprost 0.01/0.03%, Travoprost 0.004% | Once nightly | Most effective IOP reduction (~30%); once-daily convenient; side effects: iris pigmentation, hypertrichosis, periorbital fat atrophy |
| Beta-blockers | Timolol 0.25–0.5%, Levobunolol 0.5% | Once or b.i.d. | Avoid in asthma, COPD, heart block, bradyarrhythmia, congestive heart failure |
| Alpha-2 agonists | Brimonidine 0.1–0.2% | b.i.d.–t.i.d. | Contraindicated with MAOIs; caution in cardiovascular disease |
| Topical CAIs | Dorzolamide 2%, Brinzolamide 1% | b.i.d.–t.i.d. | Additive to prostaglandins; caution in sulfa allergy |
| Systemic CAIs | Acetazolamide 125–500 mg p.o. | b.i.d.–q.i.d. | For refractory cases; monitor electrolytes; contraindicated in renal failure |
| Miotics | Pilocarpine 1–4% | q.i.d. | Rarely used (side effects: accommodative spasm, retinal risk) |
Treatment is often started by using one type of drop in one eye (monocular therapeutic trial) with reexamination in 1–6 weeks to check for efficacy. — Wills Eye Manual, p. 555
Laser Treatment
- Selective Laser Trabeculoplasty (SLT) — first-line alternative or adjunct; IOP-lowering equivalent to argon laser; repeatable; particularly suitable for poor compliance or medication side effects
- Argon Laser Trabeculoplasty (ALT) — initial success 70–80%, declining to 50% at 2–5 years
Surgical Treatment
- Trabeculectomy (guarded filtration surgery) — with or without mitomycin C
- Tube-shunt surgery (e.g., Ahmed, Baerveldt)
- MIGS (minimally invasive glaucoma surgery) — for mild-to-moderate glaucoma: trabecular micro-bypass devices, canaloplasty, subconjunctival microstents, trabectome, endocyclophotocoagulation (ECP)
- Laser cyclophotocoagulation (diode laser) — for refractory or end-stage disease
- Cyclocryotherapy — for very advanced cases
Summary of This Case
| Finding | Interpretation |
|---|---|
| CDR LE = 0.7, RE = 0.4 | Asymmetric glaucomatous cupping |
| Asymmetry = 0.3 | Highly abnormal (normal <0.2) |
| Age 65, diabetic, female | Multiple POAG risk factors |
| No diabetic retinopathy | Rules out retinal confounders |
| No pain, likely asymptomatic | Consistent with POAG (silent disease) |
| Diagnosis | Primary Open-Angle Glaucoma (POAG) — Left Eye, suspect Right Eye |
| Next step | IOP (both eyes, diurnal), visual fields, gonioscopy, CCT, OCT-RNFL |
| Treatment | Prostaglandin analogue (LE first — monocular trial) with 4–6 week review |
A 76-year old man, not a known hypertensive and diabetic complains of gradual progressive loss of vision in both eyes; right eye more than the left eye for the last 6months; He was apparently normal till then. He says that some thing is obstructing his central vision. He sees all the images being distorted. A straight line appears wavy and also the images appear larger. Vn: RE - 6/36 LE – 6/12. The eye is quiet. Pupil shows normal reaction to light & accommodation. Early cataract change is seen in Lens. Fundus exam shows normal optic disc; retinal arteries are appear narrowed; there are yellowish glistening deposits in the macular area, with hyper pigmented spots scattered around. In the fovea there is some new vessel formation as well
"age-related macular degeneration" AND "anti-VEGF" treatment
Corneal ulcer bacteria vs virus f
Corneal ulcer bacteria vs virus
Corneal ulcer bacteria vs virus
Corneal ulcer bacteria vs virus
Corneal Ulcer: Bacterial vs. Viral (HSV)
At a Glance
| Feature | Bacterial | Viral (HSV) |
|---|---|---|
| Onset | Acute, rapid | Subacute/insidious; recurrent |
| Pain | Moderate–severe | Mild–moderate (reduced sensation) |
| Laterality | Usually unilateral | Unilateral (10% bilateral in primary) |
| History | Contact lens wear, trauma, surgery | Prior cold sores, recurrent eye disease, steroid use |
| Discharge | Mucopurulent, copious | Watery / minimal |
| Corneal sensation | Normal | Decreased (hypoesthesia) — key finding |
| Ulcer morphology | Round/oval, focal dense white/yellow-white stromal infiltrate with overlying epithelial defect | Dendritic (branching with terminal bulbs) or geographic (amoeba-shaped with dendritic edges) |
| Staining | Fluorescein stains the base of ulcer | Dendrite edges stain with rose bengal/lissamine green; central ulceration stains with fluorescein |
| Infiltrate | Opaque — slit beam cannot see through it | Stromal haze is more translucent (immune); epithelial lesion is superficial |
| Stromal involvement | Yes — stromal thinning, tissue loss, dense suppuration | Epithelial (dendrite), OR stromal (immune/necrotizing) — different mechanisms |
| Hypopyon | Common in moderate–severe bacterial keratitis | Absent in pure epithelial HSV; may appear in severe stromal keratitis |
| Conjunctival injection | Marked circumcorneal injection, lid oedema, chemosis | Present but often less dramatic |
| Eyelid/skin | No vesicles | May have vesicles on eyelids (unilateral, cross dermatomes) |
| Anterior chamber | Significant flare/cells, hypopyon, posterior synechiae | Mild–moderate; trabeculitis → elevated IOP is characteristic of herpetic uveitis |
| Neovascularization | Late complication | Ghost vessels (old stromal keratitis); chronic stromal vascularization indicates prior episodes |
| Perforation risk | High — especially Pseudomonas (rapid melting) | Lower for epithelial disease; necrotizing stromal keratitis can perforate |
| Bilaterality | Rare | 10% (primary); reactivation almost always unilateral |
Morphology — The Key Differentiator
Bacterial Ulcer
- Focal white/yellow-white stromal infiltrate with overlying epithelial defect
- Dense and opaque — the slit beam cannot pass through to the iris
- Heaped-up edges; round or irregular; mucopurulent base
- Surrounding stromal oedema, Descemet folds
HSV Ulcer — Three Forms
| HSV Form | Appearance | Significance |
|---|---|---|
| Dendritic keratitis | Thin, linear, branching epithelial ulceration with club-shaped terminal bulbs | Live, replicating virus — treat with antivirals |
| Geographic ulcer | Large, amoeba-shaped epithelial defect with dendritic edges | Advanced epithelial disease |
| Stromal keratitis (immune) | Unifocal/multifocal stromal haze/whitening WITHOUT epithelial defect; ± vascularization | Immune reaction (not active replication) → topical steroids + antivirals |
| Necrotizing (stromal with ulceration) | Suppurative stromal inflammation + thinning + epithelial defect; may look identical to bacterial ulcer | Must rule out bacterial superinfection |
| Disiform (endothelial) | Circular corneal stromal + epithelial oedema with keratic precipitates out of proportion to AC inflammation | Immune reaction at endothelium |
Pathogens
Bacterial
| Organism | Key Association |
|---|---|
| Pseudomonas aeruginosa | >60% of contact lens-related keratitis; aggressive, rapid melting |
| S. aureus | Focal, well-defined yellow-white infiltrate |
| S. pneumoniae | Aggressive; elderly, immunocompromised |
| Streptococcus spp. | Often aggressive |
| Moraxella | Debilitated patients (alcohol, diabetes) |
| N. gonorrhoeae | Can penetrate intact epithelium |
Viral
| Virus | Notes |
|---|---|
| HSV-1 | Most common; most common cause of central corneal ulcer and of corneal transplants in the USA |
| VZV | Pseudodendrites — slightly elevated, no true terminal bulbs, don't stain well with fluorescein; associated with dermatomal rash, Hutchinson's sign |
Diagnostics
| Test | Bacterial | Viral (HSV) |
|---|---|---|
| Corneal scraping | Mandatory — Gram stain, culture & sensitivity | Giemsa shows multinucleated giant cells (not HSV-specific); PCR preferred |
| Staining | Gram, Giemsa, Calcofluor white | Rose bengal/lissamine green (dendrite edges); fluorescein (central ulcer) |
| PCR | For atypical organisms (mycobacteria, Nocardia) | Viral PCR from corneal/conjunctival swab — high sensitivity |
| Corneal sensation | Normal | Reduced — test before instilling anaesthetic |
| Viral culture | N/A | Available but PCR preferred |
A "true" dendrite with branching epithelial ulceration and terminal end-bulbs is pathognomonic for HSV. VZV produces pseudodendrites (elevated, no bulbs, don't ulcerate centrally). — Wills Eye Manual
Treatment
| Bacterial | Viral (HSV Epithelial) | Viral (HSV Stromal — Immune) | |
|---|---|---|---|
| 1st line | Topical fluoroquinolone (ciprofloxacin/ofloxacin) 1 drop/hour day & night | Topical ganciclovir 0.15% gel 5×/day or trifluridine 1% 9×/day × 14 days | Topical corticosteroid (prednisolone 1%) + prophylactic antiviral |
| 2nd line / severe | Fortified cephalosporin + fortified aminoglycoside duotherapy | Oral acyclovir 400 mg 5×/day or valacyclovir 500 mg t.d.s. × 7–10 days | Oral acyclovir/valacyclovir |
| Adjunct | Cycloplegic; mydriatic | Cycloplegic if iritis; prophylactic topical antibiotic | Cycloplegic; monitor IOP |
| Steroids | Contraindicated until bacterial infection controlled | Avoid for epithelial disease (worsens replication) | Indicated (immune mechanism) — always cover with antiviral |
| Antifungal | Only if fungal suspected | N/A | N/A |
Key "Don't Miss" Points
- Decreased corneal sensation → think HSV (or VZV, Acanthamoeba, neurotrophic) — always test sensation before anaesthetic drops
- Dendritic ulcer = HSV until proven otherwise — do NOT give steroids alone
- Contact lens + severe pain + rapid progression = Pseudomonas — treat aggressively
- Topical steroids + a missed fungal or HSV ulcer = catastrophic worsening
- Necrotizing stromal HSV keratitis can look identical to bacterial keratitis → scrape and culture before committing to a diagnosis
- VZV pseudodendrites ≠ HSV dendrites: pseudodendrites are raised (not ulcerated), have no terminal bulbs, and don't stain well with fluorescein
i have exam viva tomorrow, can you cover opthal posting
i have pbl and prepare a slide on How will you manage a case of Acute congestive glaucoma?