Epidural analgesia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"epidural analgesia"[MeSH Terms] AND "anesthesia, obstetrical"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough response.
Epidural Analgesia
Definition and Overview
Epidural analgesia refers to the administration of analgesic drugs into the epidural space to produce segmental pain relief. It is not a single generic technique but encompasses a wide range of options - including the choice and dose of analgesic agents, location of catheter placement, and onset/duration of perioperative use. It is used for labor pain, postoperative pain (especially thoracic and abdominal surgery), and chronic pain management.
- Miller's Anesthesia, 10e, p. 11723
Anatomy and Needle Approaches
The epidural space is entered most commonly with a loss-of-resistance technique using a Tuohy needle. Two main approaches exist:
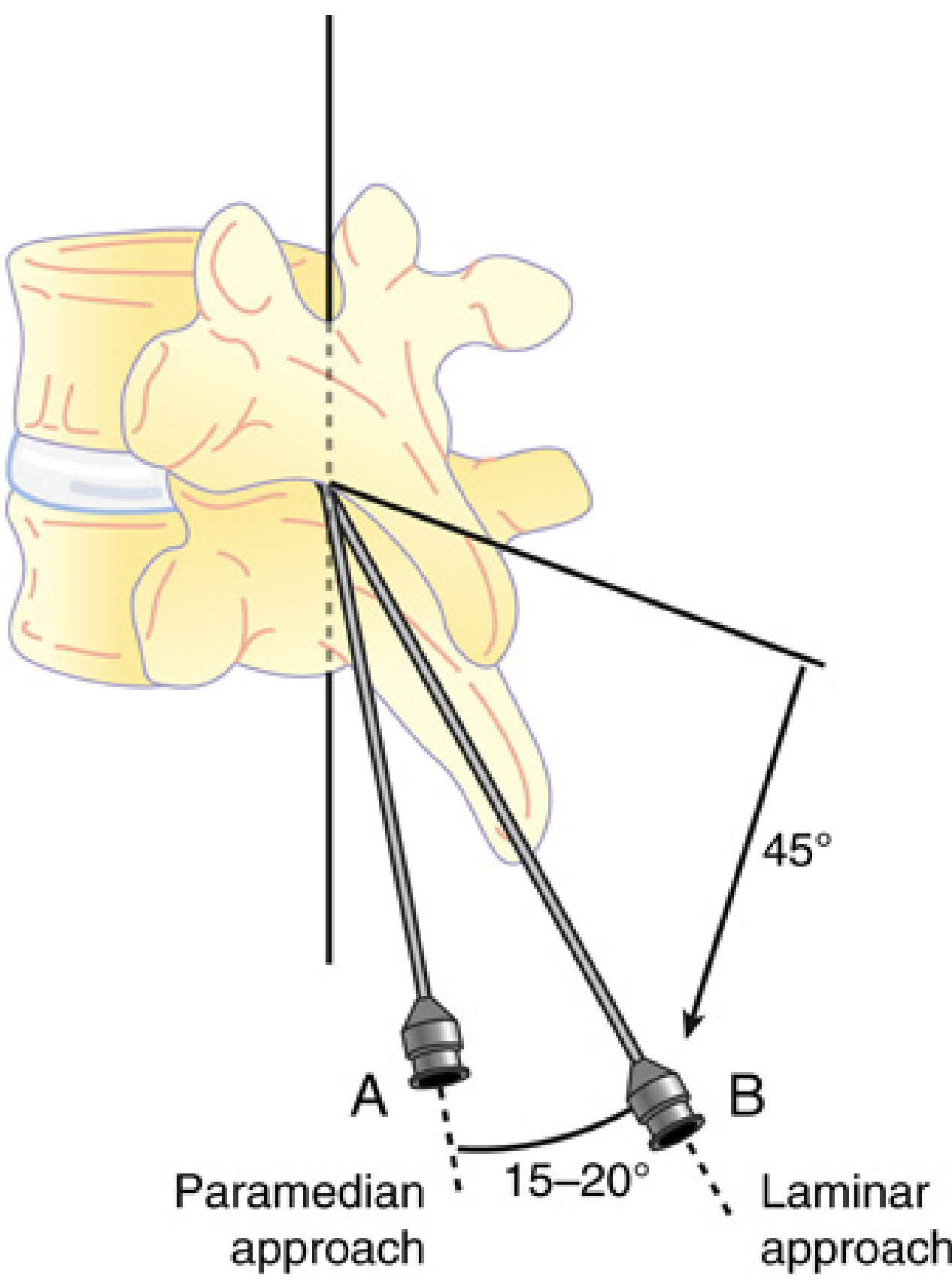
- Paramedian approach (A): Needle inserted 1 cm lateral to the superior tip of the spinous process, advanced perpendicular to contact the lamina below, then "walked" rostrally at 45° and medially at 20° over the rostral edge of the lamina until loss of resistance is felt through the ligamentum flavum. Favored by most anesthesiologists at midthoracic levels.
- Laminar approach (B): Needle inserted next to the rostral edge of the spinous process, advanced straight without angulation.
After needle placement, epidural pressure can be transduced to yield a characteristic waveform that confirms epidural space entry with high sensitivity and specificity.
- Miller's Anesthesia, 10e, p. 7340-7341
Analgesic Drugs Used
Local Anesthetics
- Epidural local anesthetic alone is less effective than local anesthetic-opioid combinations, and carries a higher failure rate with risk of motor block and hypotension.
- Bupivacaine and ropivacaine (long-acting amides) are most commonly used; they produce excellent sensory analgesia while sparing motor function at low concentrations (<0.1%).
- Epidural infusion of local anesthetic alone may be warranted to avoid opioid side effects, but the sole use is less common due to significant failure rates.
- Miller's Anesthesia, 10e, p. 11724
Opioids
Epidural opioids work by segmental spinal cord mechanisms. The combination of opioid + local anesthetic provides synergistic analgesia:
- Lipophilic opioids (fentanyl, sufentanil): rapid onset, shorter duration, less rostral CSF spread, fewer systemic side effects. Preferred in continuous infusions and PCEA.
- Hydrophilic opioids (morphine): longer duration (~24 hours), useful as single-dose for postoperative analgesia even when catheter placement is non-congruent with the incision.
- Single-dose epidural fentanyl 50-100 mcg diluted in ≥10 mL saline prolongs duration due to spread and diffusion.
- Miller's Anesthesia, 10e, p. 11723-11724
Synergy Mechanism
Local anesthetics facilitate entry of opioids from the epidural space into the CSF, increasing lumbar CSF opioid levels. Thoracic sufentanil + bupivacaine provides significantly better analgesia on movement and less sedation than opioid infusion alone.
Delivery Methods
1. Single-Dose Epidural
A one-time bolus (e.g., epidural morphine for post-cesarean analgesia). Effective but duration-limited.
2. Continuous Epidural Infusion (CEI)
Fixed-rate continuous infusion via indwelling catheter. Safe and effective; >90% of patients achieve adequate analgesia.
3. Patient-Controlled Epidural Analgesia (PCEA)
- Allows individualization of analgesic requirements via a patient-controlled pump.
- Provides analgesia superior to IV PCA in many settings.
- Lower drug use and better patient satisfaction than CEI.
- Side effect profile with PCEA: pruritus 1.8-16.7%, nausea 3.8-14.8%, sedation 13.2%, hypotension 4.3-6.8%, motor block 0.1-2%, respiratory depression 0.2-0.3%.
- Typical PCEA: low-concentration local anesthetic-lipophilic opioid combination; lipophilic opioid preferred for its rapid effect.
- Miller's Anesthesia, 10e, p. 11737
4. Programmed Intermittent Epidural Bolus (PIEB)
- Newer technique: pump delivers pre-set boluses at regular intervals.
- Bolus delivery achieves better distribution in epidural space than continuous infusion.
- Compared with CEI or PCEA: lower anesthetic dose, greater patient satisfaction, lower incidence of motor block and instrumental delivery.
- Typical settings: bolus 5-10 mL every 30-60 min, often combined with PCEA.
- Barash Clinical Anesthesia, 9e, p. 3491
Epidural Analgesia in Labor
Indications and Technique
- Used for pain relief during all stages of labor and delivery; can be converted to surgical anesthesia for cesarean delivery if needed.
- First stage of labor: ~10 mL of bupivacaine (0.125%) or ropivacaine (0.0625-0.1%) + fentanyl 50-100 µg (or sufentanil 5-10 µg) injected into mid/low lumbar epidural space.
- Maintenance: bupivacaine 0.0625-0.1% or ropivacaine 0.08-0.15%, with fentanyl 1-2 µg/mL or sufentanil 0.3-0.5 µg/mL at 10-12 mL/h.
- Operative vaginal delivery: 10 mL of bupivacaine 0.25-0.5%, lidocaine 1%, or 2-chloroprocaine 2-3% for dense sacral analgesia.
- Barash Clinical Anesthesia, 9e, p. 3490
Effect on Labor Duration
- Epidural analgesia does not increase the risk of cesarean delivery - this has been confirmed by multiple controlled trials and natural experiments.
- The only consistent effect is prolongation of the second stage of labor by approximately 25 minutes.
- Early studies suggesting increased cesarean risk were confounded; controlled trials by Chestnut et al. showed that timing of epidural placement did not affect the method of delivery.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 968
Fetal Considerations
- Late decelerations suggesting decreased uteroplacental perfusion may occur in up to 20% of cases with continuous lumbar epidural, more common with bupivacaine than chloroprocaine/lidocaine.
- Prehydration and avoidance of supine position reduce uteroplacental insufficiency.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 968
Combined Spinal-Epidural (CSE) Analgesia
CSE combines rapid, profound onset from the spinal component with the flexibility and duration of continuous epidural analgesia.
Technique: Epidural space identified with a 9-cm Tuohy needle, a 127-mm pencil-point spinal needle is advanced through it into the subarachnoid space, intrathecal drug injected, spinal needle removed, then epidural catheter inserted.
Intrathecal dose:
- Fentanyl 10-25 µg alone, or sufentanil 2-5 µg ± bupivacaine 1.25-2.5 mg
- Produces profound analgesia for 90-120 minutes with minimal motor block
- Spinal opioid alone adequate for latent phase; local anesthetic needed for active phase
Advantages over conventional epidural:
- Faster, more reliable onset
- Faster sacral spread
- Less asymmetric block
- Epidural catheters placed with CSE fail less frequently than with traditional epidural technique
Special applications:
- Early labor or pre-load-dependent conditions (e.g., aortic stenosis): opioid-only CSE avoids the preload reduction from local anesthetics and allows ambulation.
- Morbidly obese / anticipated difficult airway: CSE favored because a functional neuraxial block is already established.
- Barash Clinical Anesthesia, 9e, p. 3491-3492
Dural-Puncture Epidural (DPE) Analgesia
A CSE procedure without subarachnoid drug injection. The dural puncture itself allows enhanced transfer of epidurally administered drugs into the intrathecal space.
- Advantages over conventional epidural: confirms midline placement (CSF return), faster onset, better sacral spread, fewer asymmetric blocks.
- Advantage over CSE: avoids fetal bradycardia associated with the intrathecal injection.
- Current evidence comparing DPE vs. epidural is conflicting.
- Barash Clinical Anesthesia, 9e, p. 3492
Catheter Placement: Incision-Congruent vs. Non-Congruent
Placing the epidural catheter at a dermatome level congruent with the surgical incision (vs. non-congruent, e.g., lumbar catheter for thoracic surgery) provides:
-
Earlier return of gastrointestinal function
-
Lower incidence of myocardial infarction
-
Superior analgesia
-
Decreased motor block
-
Miller's Anesthesia, 10e, p. 11733
Benefits of Epidural Analgesia
| Organ System | Benefit |
|---|---|
| Gastrointestinal | Earlier return of motility after abdominal surgery; reduced ileus via sympathetic block + reduced opioid use |
| Pulmonary | Fewer pulmonary infections and complications (especially thoracic epidural with local anesthetic); preserves pulmonary function by reducing "splinting" |
| Cardiac | Thoracic epidural (NOT lumbar) reduces postoperative MI risk; attenuation of coronary vasoconstriction; reduced supraventricular arrhythmias in cardiac surgery |
| Neurological | Less postoperative delirium in combined epidural-general anesthetic vs. general anesthesia alone |
| Mortality | Meta-analysis of 141 trials (9,559 subjects): neuraxial anesthesia/analgesia reduces overall mortality ~30% vs. systemic opioids (primarily in orthopedic patients) |
- Miller's Anesthesia, 10e, p. 11738-11740
Complications and Risks
Hypotension
- Sympathetic fiber blockade from local anesthetics; mean incidence ~5.6% (95% CI: 3-10.2%).
- Management: reduce local anesthetic dose/rate, switch to opioid-only infusion, treat underlying cause (hypovolemia).
Motor Block
- Incidence ~2-3% with epidural local anesthetics; ~3.2% with PCEA.
- Resolves in most cases 2 hours after stopping infusion.
- Persistent or increasing motor block warrants urgent evaluation for spinal hematoma, spinal abscess, or intrathecal catheter migration.
Nausea and Vomiting
- Neuraxial opioids: up to 50% single-dose; up to 80% with continuous infusions.
- Related to cephalad CSF migration of opioid to the area postrema (medulla).
- Treatment: naloxone, droperidol, metoclopramide, dexamethasone, ondansetron, transdermal scopolamine.
Pruritus
- Most common side effect of neuraxial opioids: ~60% incidence.
- Epidural local anesthetic only: ~15-18% (similar to systemic opioids).
- Overall incidence with epidural analgesia: ~16.1%.
Urinary Retention
- Incidence: ~23% with epidural analgesia; due to spinal opioid receptor-mediated decrease in detrusor contraction.
- Treatable with low-dose naloxone (at risk of reversing analgesia).
Neurological Complications
-
Rate of neurologic complications after central neuraxial blockade: <4 in 10,000 (0.04%).
-
Epidural hematoma: increased risk with anticoagulants. ASRA guidelines govern timing of needle/catheter insertion and removal relative to anticoagulant pharmacokinetics.
-
Epidural abscess: rare (<1 in 10,000 for short-term use); higher risk with immunocompromised patients or prolonged catheterization.
-
Superficial cellulitis at catheter site: 4-14%.
-
Miller's Anesthesia, 10e, p. 11725-11744
Thoracic Epidural Analgesia (TEA) - Special Considerations
TEA is the "gold standard" for post-thoracotomy analgesia.
- Opioid + local anesthetic combinations provide better analgesia at lower doses than either drug alone.
- Paramedian approach is preferred at midthoracic levels.
- Reduces respiratory complications after thoracic and major surgery.
- TEA with local anesthetic-based regimen specifically (not opioid-only) provides the pulmonary, GI, and cardiac benefits described above.
- Miller's Anesthesia, 10e, p. 7339
Key Drug Doses Summary
| Drug | Route | Dose |
|---|---|---|
| Bupivacaine (labor, induction) | Lumbar epidural | 0.125% x 10 mL + opioid |
| Bupivacaine (maintenance) | Epidural infusion | 0.0625-0.1% at 10-12 mL/h |
| Ropivacaine (maintenance) | Epidural infusion | 0.08-0.15% at 10-12 mL/h |
| Fentanyl (labor additive) | Epidural | 1-2 µg/mL continuous, or 50-100 µg induction |
| Sufentanil (labor additive) | Epidural | 0.3-0.5 µg/mL continuous, 5-10 µg induction |
| Fentanyl (CSE, intrathecal) | Intrathecal | 10-25 µg |
| Sufentanil (CSE, intrathecal) | Intrathecal | 2-5 µg |
| Bupivacaine (CSE, intrathecal) | Intrathecal | 1.25-2.5 mg |
| Morphine (single-dose postop) | Epidural | Dose-dependent on age and catheter site |
Sources:
- Miller's Anesthesia, 2-Volume Set, 10e, Chapters 49 & 77
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, Chapter 14
- Creasy & Resnik's Maternal-Fetal Medicine, Chapter 9
Strps of epodual analgesia with diagrams and complications
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I have all the information needed for a thorough response. Let me compile it now.
Steps of Epidural Analgesia - With Diagrams and Complications
Step 1 - Understand the Relevant Anatomy
Before needle insertion, the clinician must understand the layers the needle will traverse and the boundaries of the target space.
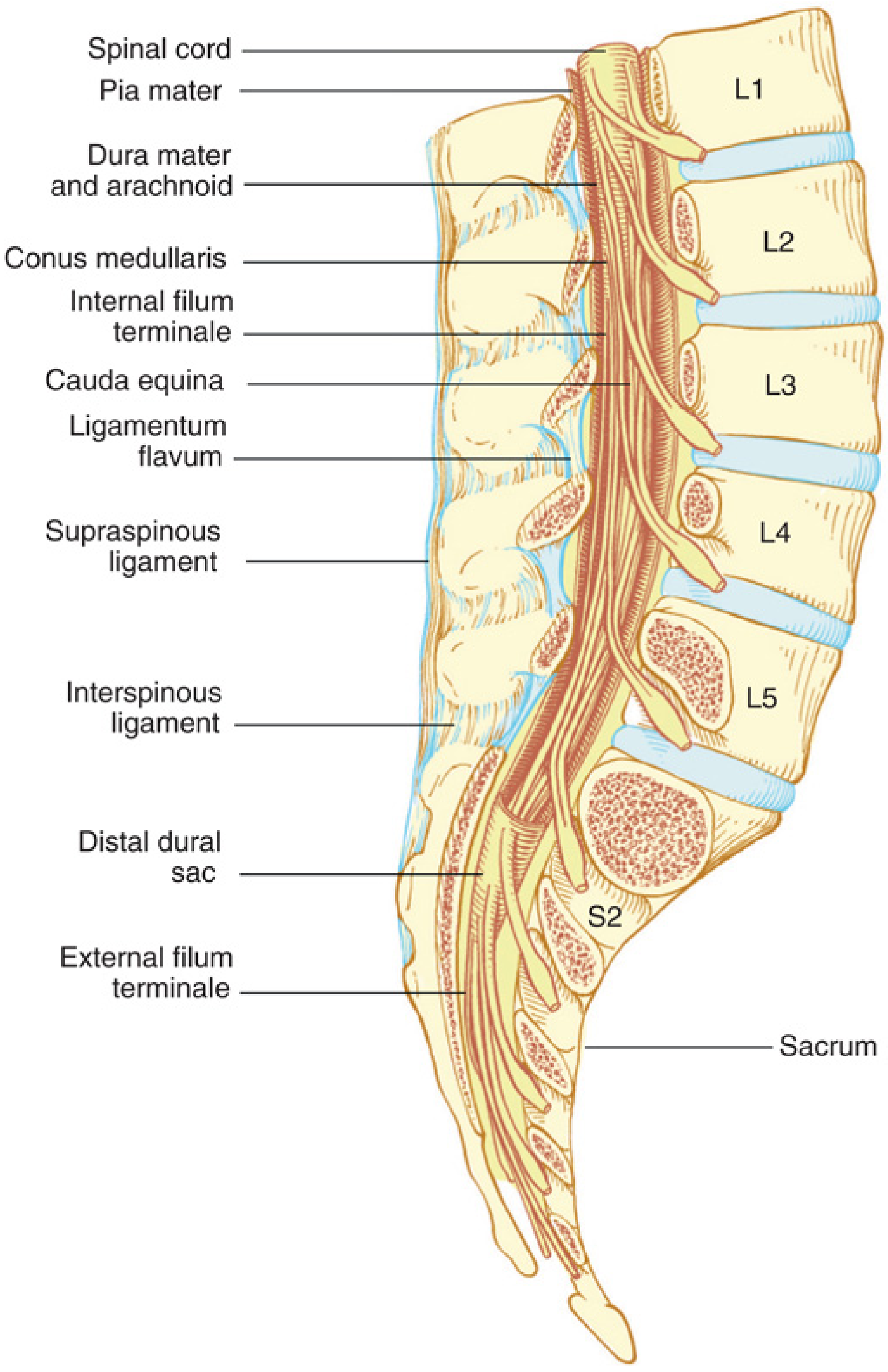
Epidural space boundaries:
- Anteriorly: Posterior longitudinal ligament
- Laterally: Pedicles and intervertebral foramina
- Posteriorly: Ligamentum flavum
- Extends: From foramen magnum to sacral hiatus
- Contents: Nerve roots, epidural fat, areolar tissue, lymphatics, and the Batson venous plexus
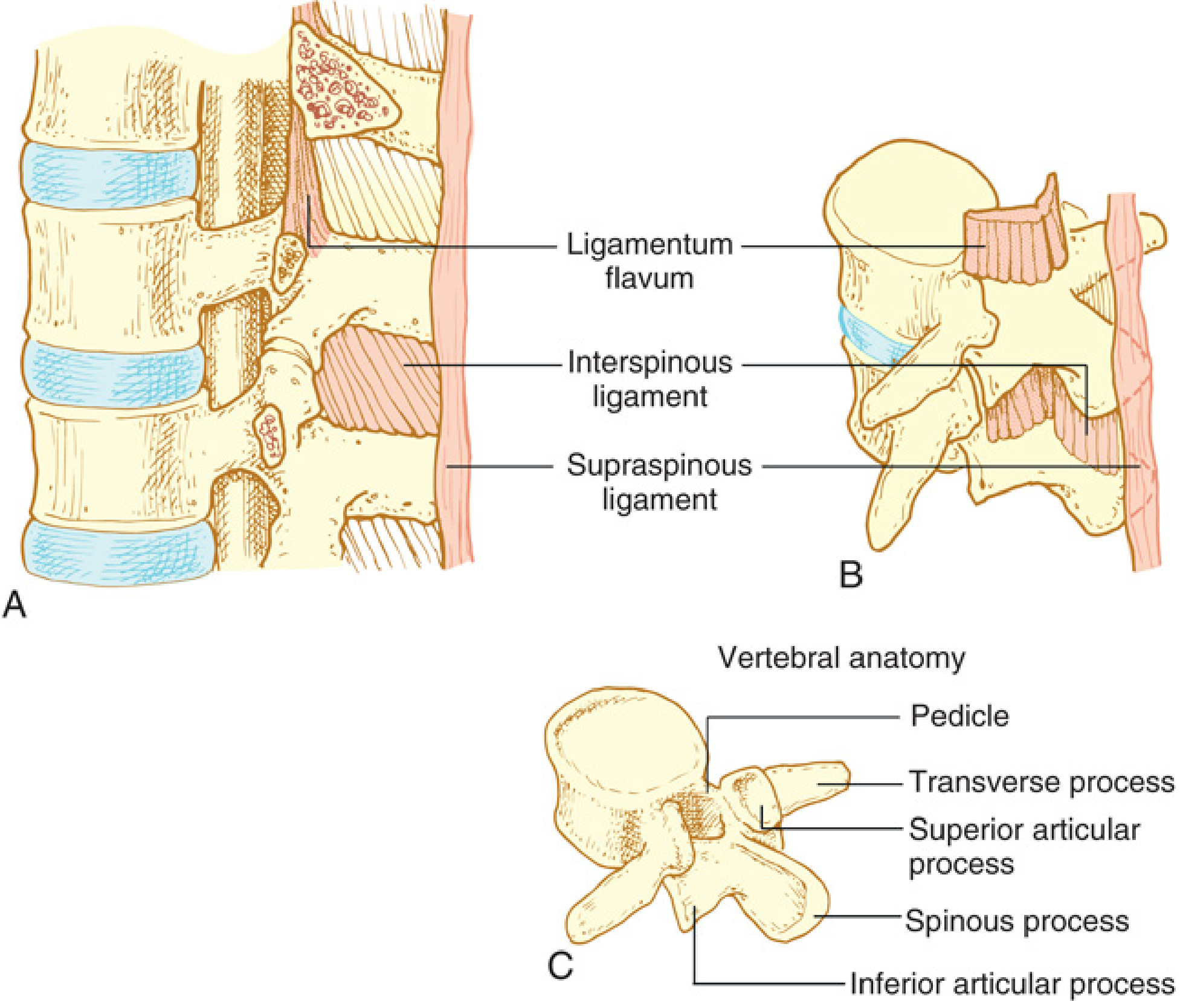
Layers the needle traverses (midline approach, superficial to deep):
- Skin
- Subcutaneous tissue
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum → epidural space entered here
- (Beyond this: dura mater, subdural space, arachnoid, subarachnoid space)
The ligamentum flavum is the key structure. It is NOT uniform - it is thicker at lumbar levels, and the two halves (right and left) may be incompletely fused in the midline at various levels.
- Miller's Anesthesia, 10e, p. 6017-6019
Step 2 - Pre-Procedure Preparation
History and examination:
- Focused history: anesthesia problems, drug allergies, current medications, coagulation status, NPO status
- Physical exam: airway, BP, heart, lungs, and back (for anatomic deformities, skin infections, scoliosis)
- Laboratory: coagulation profile if clinically indicated
Patient information and consent:
- Inform the patient of available options, benefits, and specific risks
- Obtain signed informed consent
- For obstetric patients: stress that the procedure is optional
IV access and preloading:
- Establish IV access with ≥20-gauge catheter
- Administer IV fluid bolus of 500-1000 mL before the procedure to minimize hypotension risk
- (Note: administer slowly in pregnancy-induced hypertension)
Monitoring setup:
- Continuous BP (cycled every 2.5 min during the procedure), ECG, pulse oximetry
- Record vital signs at minimum every 5 minutes
- Fetal monitoring for obstetric patients
Emergency readiness:
- Suction, oxygen, Ambu-bag, defibrillator, anesthesia machine must be available
- Vasopressors ready: ephedrine 5 mg IV or phenylephrine (for hypotension), atropine (for bradycardia)
Pfenninger & Fowler's Procedures for Primary Care, 3e
Step 3 - Equipment Preparation
From the sterile epidural tray:
| Equipment | Purpose |
|---|---|
| Tuohy needle (18-gauge, most common) | Main epidural needle; Huber tip deflects catheter forward |
| Glass LOR syringe (5 mL with saline) | For loss-of-resistance technique |
| Epidural catheter (multi-orifice, 20-gauge) | For continuous infusion |
| 25 or 27-gauge skin wheal needle | For local anesthetic skin infiltration |
| 18-gauge skin puncture needle | To nick skin before Tuohy needle insertion |
| 0.2-µm filter | On proximal catheter end (all epidural drugs must be preservative-free) |
| Syringes (3 mL, 20 mL, 5 mL glass) | For lidocaine 1%, epidural drug, LOR |
| Test dose: lidocaine 1.5% + epinephrine 1:200,000 | To detect intravascular or intrathecal placement |
Step 4 - Patient Positioning
Two options:
A. Sitting Position (preferred for obese patients)
- Patient sits at edge of bed/table, feet on a stool
- Neck and back maximally flexed ("chin to chest, hunch the back like an angry cat")
- Opens interspinous spaces to maximum width
- Assistant stands in front of patient to assist and reassure
B. Lateral Decubitus Position
- Patient lies on their side, knees drawn up to chest, chin tucked to neck
- Spine must be straight (not rotated)
- Useful when patient cannot sit (pain, labor, sedation)
The flexed position widens the interspinous gap and opens the ligamentum flavum, facilitating needle entry.
Step 5 - Level Selection and Surface Landmarks
Lumbar epidural (most common):
- L3-L4 interspace is most commonly used (identified by the Tuffier's line - a line connecting the two posterior iliac crests crosses the L3-L4 or L4 spinous process)
- Also used: L2-L3, L4-L5
- Insertion angle at L4-L5: nearly 90° (perpendicular); decreases to ~70° at L2-L3
Thoracic epidural:
- For post-thoracotomy or major abdominal surgery
- Thoracic spinous processes are steeply angulated caudad (unlike the nearly horizontal lumbar spinous processes)
- Paramedian approach preferred at midthoracic levels (see diagram below)
Identify the interspace: Palpate spinous processes; mark the interspace with a fingernail indentation or skin marker.
Step 6 - Sterile Preparation and Skin Infiltration
- Open sterile epidural tray; wear sterile gloves
- Prep the back with antiseptic solution (chlorhexidine-based); allow to dry
- Apply sterile drapes
- Raise a skin wheal with lidocaine 1% at the chosen interspace using a 25-27g needle
- Inject deeper along the intended needle track (at the same angle) to anaesthetize deeper tissues (interspinous ligament)
- Make a small skin nick with an 18g needle to ease passage of the Tuohy needle
Step 7 - Tuohy Needle Insertion and Epidural Space Identification
Midline Approach
- Insert the Tuohy needle below the inferior border of the spinous process at the chosen interspace
- Advance slowly through skin → subcutaneous tissue → supraspinous ligament → interspinous ligament; resistance increases progressively
- Once firmly in the interspinous ligament, remove the stylet
- Attach the glass LOR syringe filled with saline (2-3 mL)
Loss-of-Resistance (LOR) Technique
- Apply constant gentle pressure to the syringe plunger while slowly advancing the needle
- While the needle tip is in the ligamentum flavum, the syringe plunger resists compression
- When the needle tip enters the epidural space, there is a sudden loss of resistance - the plunger falls forward freely and saline injects easily
- Alternatively: the hanging drop method - a drop of saline at the needle hub is drawn inward by the negative epidural pressure as the needle enters the space
Confirming Correct Placement
- Aspirate: no blood (vascular) and no CSF (intrathecal) should return
- If epidural pressure is transduced, a characteristic waveform confirms the epidural space
- Inject 5 mL saline - should flow freely without resistance
Paramedian approach (thoracic): Insert needle 1 cm lateral to the superior tip of the spinous process → advance perpendicular to contact the lamina below → "walk" rostrally at 45° and medially at 20° over the rostral laminar edge → LOR as the needle traverses the ligamentum flavum
- Miller's Anesthesia, 10e, p. 7340; Pfenninger & Fowler's, p. 44
Step 8 - Epidural Catheter Insertion
- Rotate the Tuohy needle bevel in the desired direction (cephalad for most cases) - the curved bevel deflects the catheter in that direction
- Insert the catheter tip through the needle hub; advance slowly
- A slight resistance is felt as the tip exits the needle bevel into the epidural space
- Advance the catheter 5 cm into the epidural space beyond the needle tip (this is the optimal threading depth - too little risks displacement; too much risks coiling, knotting, or intravascular placement)
- Hold the catheter firmly and withdraw the Tuohy needle over the catheter - never withdraw the catheter through the needle (the bevel can shear off the catheter tip)
- Never re-advance the needle once the catheter is in place
Securing the Catheter
- Note the cm marking at the skin entry point
- Tape the catheter along the back after the patient sits upright (the catheter moves as the patient straightens from the flexed position)
- Attach a 0.2-µm filter to the proximal end
- Secure tubing to the patient's gown to prevent accidental dislodgement
Step 9 - Test Dose Administration
Purpose: To detect intravascular or intrathecal placement of the catheter
Method:
- Aspirate first - check for blood or CSF
- Administer 3 mL of lidocaine 1.5% + epinephrine 1:200,000 (= 45 mg lidocaine + 15 µg epinephrine)
- Wait 3-5 minutes and monitor:
| Positive Test Dose | Indicates | Interpretation |
|---|---|---|
| HR increase ≥20 bpm within 30-60 s | Intravascular placement (epinephrine marker) | False-positive possible in active labor |
| Sensory/motor block of lower limbs within 5 min | Intrathecal placement | Spinal doses injected → high/total spinal risk |
| Tinnitus, metallic taste, perioral numbness | Intravascular (lidocaine CNS toxicity) | Systemic injection |
If intravascular: Remove catheter; re-site at different interspace
If intrathecal: Option 1 - remove and re-site; Option 2 - use as continuous spinal catheter (with extreme caution - label clearly to avoid large "epidural" doses intrathecally)
Note: The epinephrine test dose can be unreliable in patients on β-blockers and in obstetric patients where contractions may produce a false-positive tachycardia. Incremental injection (5 mL fractions) remains the safest strategy.
- Miller's Anesthesia, 10e, p. 6128-6129
Step 10 - Drug Injection and Maintenance
- Inject the epidural drug incrementally in 5 mL fractions while monitoring vital signs
- Assess the level and quality of block after each increment
- Establish the maintenance regimen (CEI, PCEA, or PIEB)
- Document: drug, dose, route, time, vital signs, level of block
Factors affecting block level:
- Level of injection (primary determinant)
- Volume and concentration of solution
- Rate of injection
- Patient age, height, body habitus
- Addition of vasoconstrictor (epinephrine prolongs/intensifies block)
- Patient position during injection
Summary Flow Diagram
Consent + IV access + preloading
↓
Monitor: BP, ECG, SpO₂
↓
Position patient (sitting or lateral decubitus)
↓
Identify interspace (L3-L4 most common)
↓
Sterile prep + skin/deep infiltration with lidocaine
↓
Skin nick with 18g needle
↓
Tuohy needle insertion → interspinous ligament
↓
Attach LOR syringe → advance with constant pressure
↓
Loss of resistance → epidural space confirmed
↓
Aspirate (no blood, no CSF)
↓
Thread catheter 5 cm → withdraw needle
↓
Secure catheter → attach filter
↓
Test dose → wait 3-5 min
↓
Incremental drug injection → assess block
↓
Maintenance infusion (CEI / PCEA / PIEB)
Complications
A. Procedure-Related (Immediate)
| Complication | Incidence | Mechanism | Recognition | Management |
|---|---|---|---|---|
| Dural puncture / "wet tap" | ~1% | Needle passes through dura | CSF freely returns through needle | Resite at different level OR advance catheter intrathecally as continuous spinal |
| Intravascular injection | Rare | Catheter enters epidural vein (Batson plexus) | Blood on aspiration; positive test dose (tachycardia, CNS symptoms) | Withdraw catheter; resite; LAST protocol if toxicity develops |
| Total/high spinal | Rare | Large volume injected intrathecally | Rapid ascending block, hypotension, apnoea, loss of consciousness | Airway support, intubation, vasopressors |
| Subdural injection | <1% | Catheter enters subdural extra-arachnoid space | Higher-than-expected block after 15-30 min delay; exaggerated sympathetic block; modest motor block | Symptomatic; remove catheter |
| Catheter shearing | Rare | Withdrawing catheter through needle bevel | Catheter segment left in epidural space | Usually managed conservatively if asymptomatic |
B. Drug-Related Complications
| Complication | Incidence | Notes |
|---|---|---|
| Hypotension | ~5.6% (mean) | Sympathetic block from local anesthetic; treat with IV fluids, decrease LA rate, vasopressors (ephedrine/phenylephrine) |
| Motor block | 2-3% | Lower concentration LA reduces risk; persistent/worsening motor block = emergency (rule out hematoma or abscess) |
| Pruritus | ~60% (opioid-related) | Most common opioid side effect; treat with low-dose naloxone, ondansetron, diphenhydramine |
| Nausea/vomiting | Up to 80% (continuous opioid) | CSF rostral spread to area postrema; treat with metoclopramide, ondansetron, dexamethasone |
| Urinary retention | ~23% | Opioid receptor-mediated detrusor inhibition; low-dose naloxone; catheterization |
| Respiratory depression | 0.2-0.3% (PCEA) | Hydrophilic opioids (morphine) > lipophilic; delayed onset (up to 12-24h for morphine) |
| Local anesthetic systemic toxicity (LAST) | Rare | CNS symptoms first (tinnitus, perioral numbness, convulsions) → cardiovascular collapse; treat with lipid emulsion 20% |
C. Post-Procedure Complications
| Complication | Incidence | Notes |
|---|---|---|
| Post-dural puncture headache (PDPH) | High (after accidental wet tap with Tuohy needle) | Positional, frontal/occipital; worse upright, relieved supine. Conservative: supine position, hydration, caffeine, analgesics. Definitive: epidural blood patch (15-20 mL autologous blood injected at or below the puncture level; 90% initial improvement, persistent resolution in 61-75%) |
| Epidural hematoma | <4 in 10,000 | Risk increased with anticoagulants; presents as back pain + progressive neurological deficit; surgical emergency - needs MRI + urgent decompression within 6-8 hours |
| Epidural abscess | <1 in 10,000 (short-term use) | Higher risk with immunocompromise or prolonged catheterization; presents with fever, back pain, neurological deficit; MRI + antibiotics ± surgical drainage |
| Superficial cellulitis | 4-14% | At catheter insertion site; clean technique + regular site inspection |
| Neurological damage | Rare (permanent <0.04%) | Trauma, anterior spinal artery syndrome, or compression from hematoma/abscess |
| Transient neurologic symptoms | Uncommon | Bilateral buttock/leg pain within 24h of block resolution; self-limiting within 1 week; treat with NSAIDs |
D. Obstetric-Specific
| Complication | Notes |
|---|---|
| Fetal bradycardia | More common with CSE; due to rapid decrease in maternal epinephrine or uteroplacental hypoperfusion from hypotension |
| Prolonged second stage | ~25 min prolongation; does NOT increase cesarean delivery rate |
| Increased instrumental delivery | Modest increase; reduced with dilute LA concentrations and PIEB |
| Back pain | No causative relationship proven in prospective studies |
Key safety rule: Any new or worsening neurological deficit in a patient with an epidural catheter in situ must be urgently evaluated. Never delay assessment - epidural hematoma and abscess require emergency decompression to prevent permanent paralysis.
Sources:
- Miller's Anesthesia, 2-Volume Set, 10e, Chapters 41 & 77
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, Chapter 14
- Pfenninger & Fowler's Procedures for Primary Care, 3e, Chapter 3
- Creasy & Resnik's Maternal-Fetal Medicine, Chapter 9
This is a shared conversation. Sign in to Orris to start your own chat.