Blood bank and transfer pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have excellent, comprehensive material from multiple authoritative textbooks. Here is the full, organized reference on Blood Bank and Transfusion Pathology.
Blood Bank and Transfusion Pathology
1. Historical Milestones
Blood transfusion has a rich history. Key dates from - Bailey and Love's Short Practice of Surgery, 28th Ed.:
| Year | Event |
|---|---|
| 1818 | James Blundell performs the first successful human transfusion (postpartum haemorrhage, patient survived) |
| 1901 | Karl Landsteiner discovers the ABO system |
| 1914 | Albert Hustin performs first non-direct transfusion using sodium citrate anticoagulant |
| 1926 | British Red Cross institutes the world's first blood transfusion service |
| 1939 | Rhesus system identified as a major cause of transfusion reactions |
2. Blood Donation and Screening
In standard practice, up to 450 mL of blood is drawn per donation, a maximum of three times per year. Each unit is tested for:
- Hepatitis B and C
- HIV-1 and HIV-2
- Syphilis
Units are leukodepleted as a precaution against variant Creutzfeldt-Jakob disease (vCJD) - this also reduces immunogenicity. The ABO and Rh(D) blood groups are determined, along with a screen for irregular red cell antibodies.
3. Blood Groups
ABO System
Controlled by three allelic genes (A, B, O) that produce enzymes adding carbohydrate residues to cell surface glycoproteins. The O gene is an amorph (adds nothing).
| Phenotype | Genotype | Antigens | Antibodies | UK Frequency |
|---|---|---|---|---|
| O | OO | O | Anti-A, anti-B | 46% |
| A | AA or AO | A | Anti-B | 42% |
| B | BB or BO | B | Anti-A | 9% |
| AB | AB | A and B | None | 3% |
- Group O = Universal donor (no antigens to provoke a reaction)
- Group AB = Universal recipient (no circulating antibodies)
Rhesus (Rh) System
- The Rh(D) antigen is strongly antigenic; present in ~85% of the UK population
- Anti-D antibodies are not naturally occurring - they are stimulated by transfusion of Rh+ blood or delivery of an Rh(D)+ baby
- Anti-D crossing the placenta in an Rh(D)-negative mother can cause haemolytic disease of the newborn (HDN) - severe haemolytic anaemia or hydrops fetalis
4. Blood Products
Whole Blood
- Rarely available in civilian practice; replaced by component therapy
- Advantages: coagulation factor-rich, metabolically active if fresh
- Indications: acute blood loss replacement, volume expansion in septicaemia with coagulopathy
Packed Red Blood Cells (pRBCs)
- Each unit ~330 mL, haematocrit 50-70%
- Stored in SAG-M (saline-adenine-glucose-mannitol) solution at 2-6°C
- Shelf life: 5 weeks (older CPD storage: 2-3 weeks)
Fresh Frozen Plasma (FFP)
- Rich in all coagulation factors
- Stored at -40 to -50°C; shelf life 2 years
- First-line therapy for coagulopathic haemorrhage
- Note: Rh(D)-positive FFP can be given to Rh(D)-negative women, but seroconversion is possible with large volumes due to red cell fragments - consider Rh-D immunisation prophylaxis
Cryoprecipitate
- Supernatant precipitate of FFP
- Rich in: fibrinogen, Factor VIII, Factor XIII
- Stored at -30°C; shelf life 2 years
- Indications: low-fibrinogen states, Factor VIII deficiency
Platelets
- Pooled concentrate: ~250 × 10⁹/L
- Stored on a special agitator at 20-24°C; shelf life only 5 days
- Given for thrombocytopenia or platelet dysfunction in bleeding/surgery
- Patients on clopidogrel who are actively bleeding may need near-continuous infusion; DDAVP has limited success
Prothrombin Complex Concentrates (PCC)
- Highly purified; contains Factors II, IX, X (±VII)
- Indicated for emergency reversal of warfarin in uncontrolled haemorrhage
- Dose: 25-50 units/kg based on INR; preferred over FFP for warfarin reversal (BCSH 2012 guidelines)
Autologous Blood
- Pre-donation up to 3 weeks before elective surgery for re-transfusion
- Cell salvage: intraoperative collection, washing, and reinfusion of red cells
5. Indications and Transfusion Trigger
Indications for transfusion:
- Acute blood loss (restore circulating volume and O₂ delivery)
- Perioperative anaemia
- Symptomatic chronic anaemia
Modern transfusion thresholds (abandoning the old "10 g/dL rule"):
| Hb (g/dL) | Action |
|---|---|
| <6 | Probably will benefit from transfusion |
| 6-8 | Unlikely to benefit without active bleeding or impending surgery |
| >8 | No indication in absence of other risk factors |
6. Cross-Matching
- Full cross-match (ABO + Rh typing + recipient serum vs donor cells): takes up to 45 minutes
- "Type-specific" blood (ABO/Rh matched only): available within 10-15 minutes
- Emergency: Group O blood (O- for females of childbearing age; O+ for males)
7. Transfusion Reactions
Acute Reactions
Immediate Haemolytic Transfusion Reaction (IHTR)
- Caused by ABO incompatibility - usually clerical/human error (~1 in 180,000 red cells transfused)
- Mechanism: IgM complement-fixing anti-A/anti-B antibodies cause intravascular haemolysis
- Consequences: cytokine release, activation of coagulation, renal failure, DIC
- Features: pain at infusion site, chest and back pain, hypotension, haemoglobinuria
- Mortality: up to 10%
Febrile Non-Haemolytic Transfusion Reaction (FNHTR)
- Caused by recipient's anti-leucocyte antibodies reacting with leukocytes in transfused components
- Features: fever, chills/rigors, nausea, muscle pain
- Temperature rise >38°C but <2°C above baseline: slow transfusion + antipyretics (paracetamol)
- Temperature >39°C or rise >2°C: stop transfusion
- Now rare with leukodepleted blood
Allergic Reaction / Anaphylaxis
- Mild (urticaria, flushing): slow infusion, antihistamines
- Severe anaphylaxis (wheeze, stridor, angioedema): IM adrenaline + IV chlorpheniramine + IV hydrocortisone
TRALI - Transfusion-Related Acute Lung Injury
- Typically after platelets or FFP (multi-parous female donors are higher risk)
- Mechanism: Two-hit model
- Donor anti-leukocyte antibodies (HLA class I/II or neutrophil-specific antigen antibodies) react with recipient neutrophils - "first hit"
- Bioactive lipids/cytokines stored in blood products activate primed pulmonary neutrophils - "second hit"
- Features: severe hypoxia, hypotension, bilateral lung infiltrates within 6 hours of transfusion
- Distinguishing from ARDS or TACO is important
- Treatment: supportive - high-flow oxygen, ventilator support if needed
TACO - Transfusion-Associated Circulatory Overload
- Common in elderly and cardiac patients; frequently underdiagnosed
- Defined as: acute/worsening pulmonary oedema within 6 hours of transfusion
- Features: dyspnoea, tachycardia, hypertension (key distinction from TRALI), positive fluid balance
- Treatment: stop transfusion, oxygen, diuretics
- Prevention: co-administration of diuretics, single unit transfusions in frail adults
Approach to Acute Transfusion Reaction (BOX - Scott-Brown's)
- Stop the transfusion
- Assess: Airway, Breathing, Circulation
- Maintain IV access with physiological saline
- Check patient ID and blood component compatibility
- Inspect component for clumps/discolouration
- Assess for evidence of blood loss
- (Unless mild allergic/febrile): FBC, renal/liver screen, blood culture, direct Coombs test, repeat group & screen, urine for haemoglobinuria
- Inform the transfusion laboratory
- Return blood component to the transfusion laboratory
- Report to SHOT (Serious Hazards of Transfusion)
SHOT Report Data (Cumulative 1996-2012)
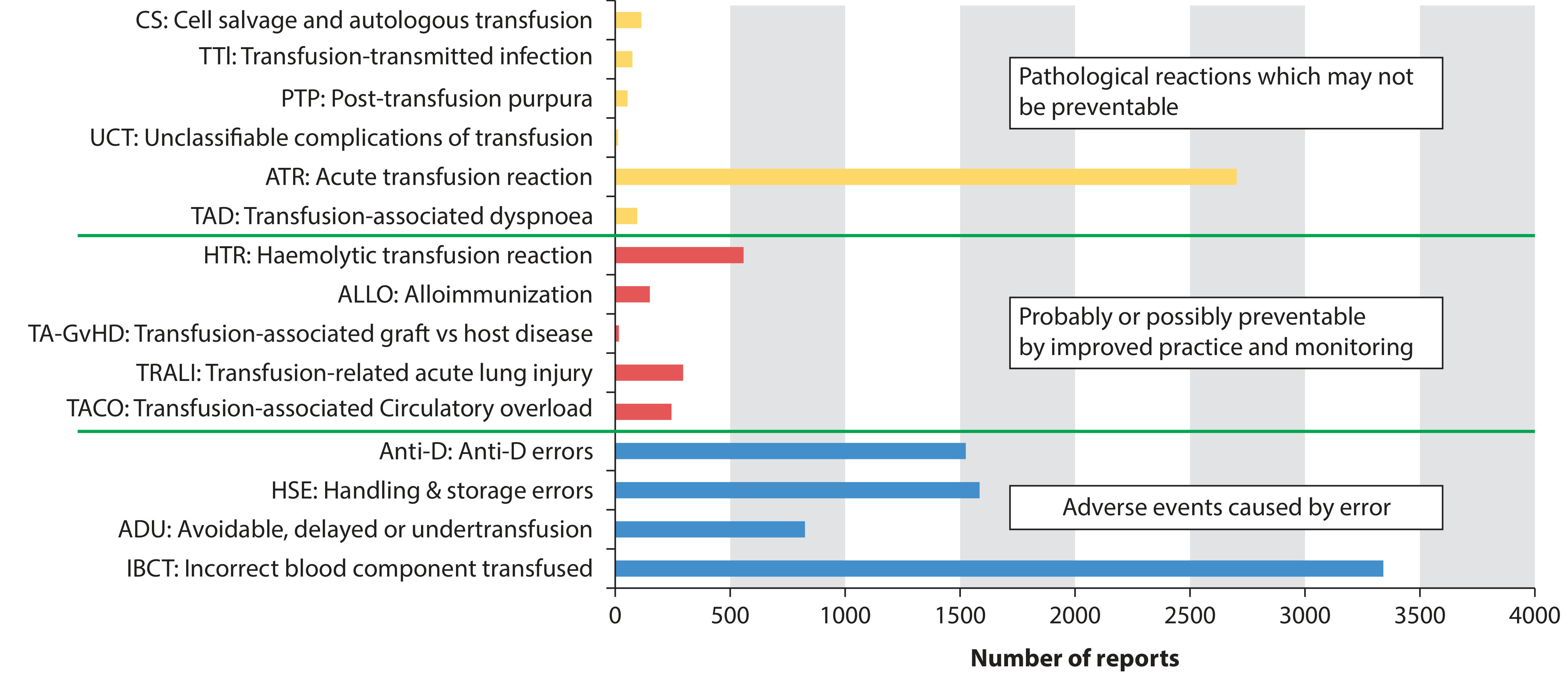
Key takeaway: Incorrect blood component transfused (IBCT) and handling/storage errors dominate - emphasizing that most serious adverse events are preventable errors, not unavoidable pathological reactions. - Scott-Brown's Otorhinolaryngology, Vol 1
Delayed Reactions
Delayed Haemolytic Transfusion Reaction (DHTR)
- Occurs days after transfusion in previously sensitized individuals (prior transfusions or pregnancy)
- Mechanism: alloantibodies (Rh, Kell, Duffy) had fallen below detectable levels; re-exposure triggers a secondary IgG immune response and extravascular haemolysis
- Features: jaundice, haemoglobinuria, fever, fatigue, anaemia; rarely renal failure
- Investigations: drop in Hb, positive direct Coombs test, raised bilirubin
Post-Transfusion Purpura (PTP)
- Severe thrombocytopenia (platelets <10 × 10⁹/L) 7-12 days post-transfusion
- Occurs in previously pregnant/transfused females who are HPA-1a antigen negative
- Develops high anti-HPA-1a levels after transfusion
- Treatment: high-dose IV immunoglobulin; now rare since leukodepletion
Transfusion-Associated Graft Versus Host Disease (TA-GVHD)
- Rare but usually fatal
- Cause: donor lymphocytes engraft in recipient and mount immune attack
- Features: fever, rash, diarrhoea, jaundice, bone marrow failure (appearing up to 30 days post-transfusion)
- At-risk: immunocompromised patients (congenital immunodeficiency, HIV, post-BMT, fludarabine therapy)
- Prevention: gamma-irradiated blood components
8. Complications of Massive Transfusion
Massive transfusion is defined as replacement of one blood volume within 24 hours (roughly 10+ units).
| Complication | Mechanism / Notes |
|---|---|
| Coagulopathy | Dilution of clotting factors; hypothermia worsens enzyme function; acidosis compounds effect - the "lethal triad" |
| Hypocalcaemia | Citrate (anticoagulant in stored blood) chelates Ca²⁺; leads to muscle weakness, arrhythmias, myocardial dysfunction |
| Hyperkalaemia | K⁺ leaks from stored red cells; dangerous with rapid transfusion |
| Hypokalaemia | Paradoxically can follow if citrate is metabolised to bicarbonate, driving K⁺ intracellularly |
| Hypothermia | From infusion of cold blood products; directly worsens coagulopathy and can double mortality |
| Iron overload | In patients requiring repeated long-term transfusions (e.g. thalassaemia) |
Management of Coagulopathy in Massive Haemorrhage
- Damage control resuscitation: deliver matched RBC : FFP : platelets in 1:1:1 ratio (approximates whole blood)
- Tranexamic acid: empirically, as early as possible - most bleeding patients are hyperfibrinolytic
- Cryoprecipitate: for low fibrinogen (guided by TEG/ROTEM or empirically)
- Avoid crystalloids and colloids if at all possible (dilute clotting factors)
- Frequent point-of-care coagulation testing (thromboelastometry)
9. Infection Transmission Risk
| Pathogen | Notes |
|---|---|
| HIV | Screened; risk very low |
| Hepatitis B & C | Screened; tested on every unit |
| Malaria | Donor exclusion (travel history) |
| Bacterial contamination | Most often platelets (stored at room temperature); patient develops acute septic shock; broad-spectrum antibiotics immediately; return component to lab |
| vCJD | Leukodepletion used as precaution |
10. Blood Substitutes
Under investigation as alternatives to allogeneic transfusion:
- Biomimetic (haemoglobin-based): engineered molecules from human, bovine or recombinant sources; one free Hb solution commercially available in some countries
- Abiotic (perfluorocarbon-based): synthetic oxygen carriers; second-generation emulsions in clinical trials
- No widely approved substitute available yet in most countries
Summary of Key Safety Points
- Always confirm patient identity and blood compatibility with two healthcare personnel before transfusion
- The commonest cause of fatal reactions is ABO incompatibility due to clerical error - not inherent product failure
- Universal leukodepletion has significantly reduced FNHTR and TA-GVHD
- In active haemorrhage, a 1:1:1 ratio of RBC:FFP:platelets plus tranexamic acid is standard damage control resuscitation
- For warfarin reversal: PCC + vitamin K preferred over FFP
- High-risk patients (immunocompromised) must receive gamma-irradiated components to prevent TA-GVHD
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 | Goldman-Cecil Medicine | Sabiston Textbook of Surgery | 22nd Edition Pye's Surgical Handicraft
This is a shared conversation. Sign in to Orris to start your own chat.