Sacral agenesis
Reading File
Finding Sources
Finding Sources
Searching PubMed
sacral agenesis caudal regression syndrome
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of sacral agenesis drawn from multiple authoritative textbooks.
Sacral Agenesis (Caudal Regression Syndrome)
Definition
Sacral agenesis is the absence of part or all of two or more lower vertebral bodies, representing failure of embryonic development of the sacrum and lower spine. It is a form of closed spinal dysraphism, also termed caudal regression syndrome when more extensive caudal structures are involved.
- Comprehensive Clinical Nephrology, 7th Ed.: "a rare anomaly in which part or all of two or more vertebral bodies is absent... occurs early in fetal development when there is failure of ossification of the lowest vertebral segments."
Incidence
- 1–5 per 100,000 live births overall
- ~3 per 1,000 diabetic pregnancies (classically reported)
- Strongly associated with maternal type 1 diabetes; 16% or more of affected children have an insulin-dependent diabetic mother
- Insulin-dependent diabetic mothers have a ~1% risk of delivering an affected child
- Campbell-Walsh-Wein Urology
Etiology & Pathogenesis
The precise cause remains uncertain, but several factors are implicated:
- Maternal hyperglycemia — the leading extrinsic teratogen; disrupts growth of pluripotential somatic stem cells at the caudal eminence, impairing distal neural tube, caudal mesenchyme, and hindgut formation.
- Chromosomal/genetic factors — deletion of chromosome 7q36 leading to absence of a transcription factor; may affect SHH (Sonic Hedgehog) signaling.
- Currarino syndrome (triad: presacral mass + sacral agenesis + anorectal malformation) — caused by mutations in HLXB9, a homeodomain gene on 7q; found in 20/21 familial and 2/7 sporadic cases.
- Maternal drug exposure — e.g., minoxidil has been reported as a cause.
- Insulin-antibody complexes crossing the placenta have been proposed as a mechanism.
Clinical Presentation
Presentation is bimodal:
- >75% detected in early infancy
- Remainder discovered between 4–5 years of age (often during failed toilet training)
Physical examination clues:
- Flattened buttocks
- Short, low gluteal cleft (pathognomonic appearance)
- Palpable absence of the coccyx
Urological symptoms (in children ≥4 years):
- Urinary incontinence or constant dribbling: ~85%
- Recurrent UTI: ~74%
- Vesicoureteral reflux (VUR): up to 65%
Distinguishing feature: Sensation (including perianal dermatomes) is typically intact, and lower extremity function is often normal, unlike myelomeningocele. High-arched feet, claw toes, or hammer toes may be present.
Neurourological Dysfunction
Urodynamic patterns:
- Upper motor neuron (detrusor overactivity): ~35%
- Lower motor neuron (areflexic/acontractile bladder): ~40%
- No denervation signs: 20–25%
Importantly, the number of absent vertebrae does not correlate with the type or severity of bladder dysfunction.
Diagnosis
Radiological confirmation:
- Lateral plain film of the lower spine is the most straightforward (AP view is often obscured by bowel gas)
- MRI reveals a characteristic sharp cutoff of the conus at T12 — a consistent finding
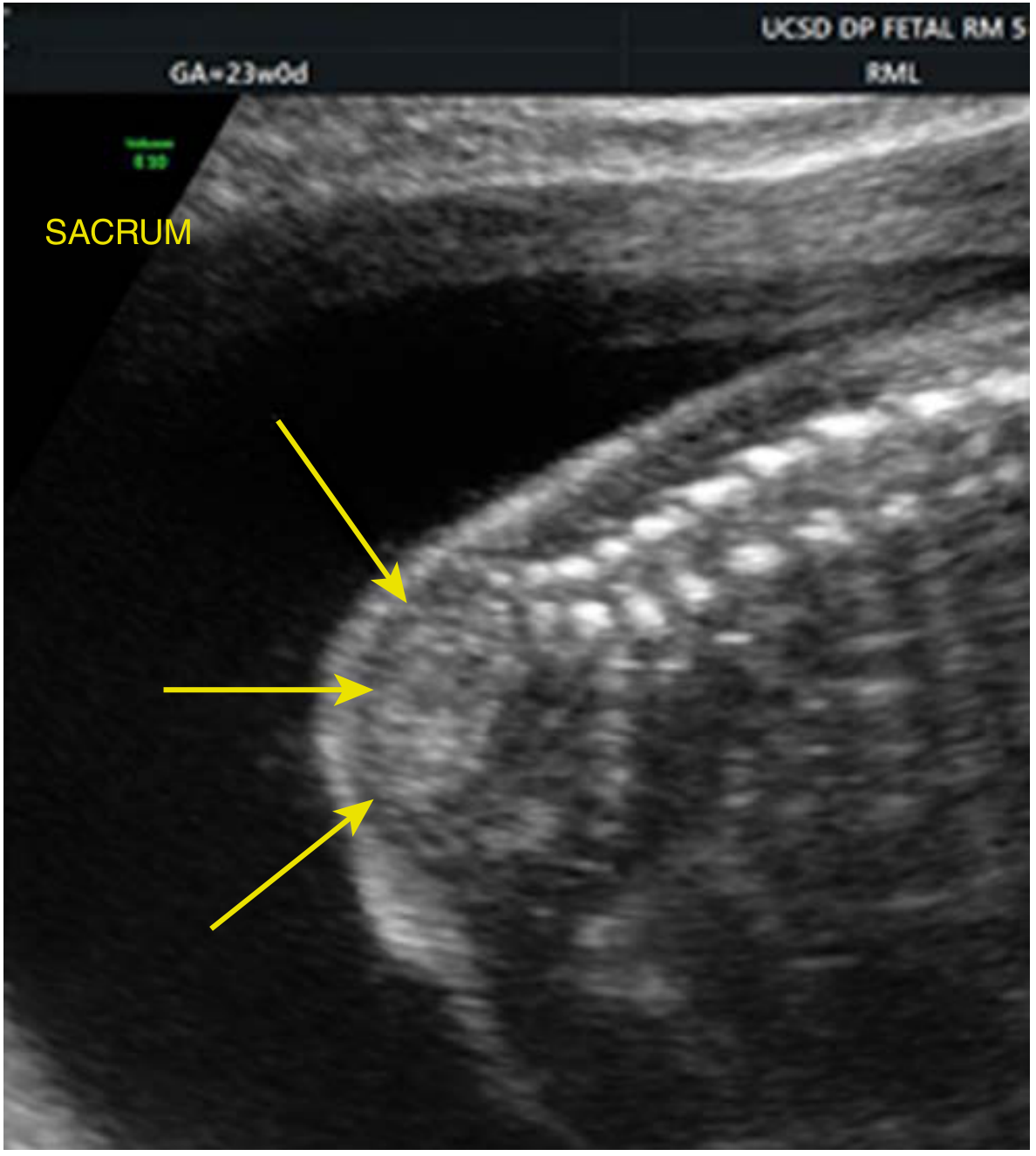
- Sacral ossification begins at 15 weeks gestation; detectable by prenatal ultrasound after 18 weeks
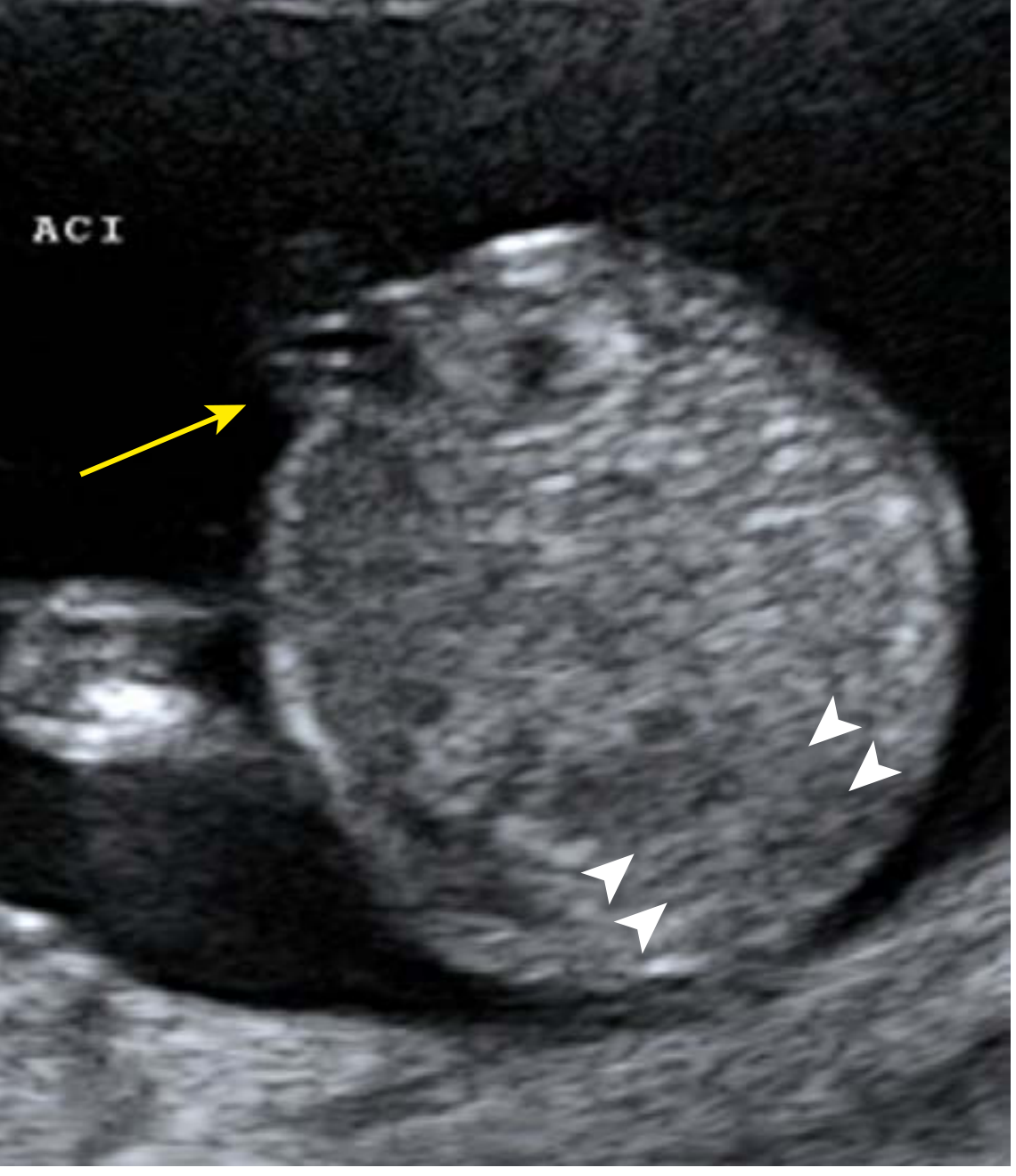
Prenatal ultrasound appearance:
- Abrupt termination of the lower spine on sagittal imaging
- Confirmed on axial view: cord insertion visible anteriorly but spine absent posteriorly
Prenatal workup:
- Amniocentesis/microarray or NIPT for karyotype
- Fetal 3D skeletal imaging and/or fetal MRI
- Fetal echocardiogram (associated cardiac anomalies)
Associated Anomalies
- Currarino triad: sacral agenesis + presacral mass + anorectal malformation (HLXB9 mutation)
- Anterior sacral meningocele
- Anorectal malformations
- VUR, renal anomalies
- Other: imperforate anus, cryptorchidism, radial hypoplasia, tracheoesophageal fistula (in complex cases)
Management
Urological (Campbell-Walsh-Wein Urology)
- Urodynamics (UDS) — mandatory at diagnosis
- Renal ultrasound + nuclear or conventional cystography (especially with UTI history or upper motor neuron pattern)
Based on UDS findings:
| Pattern | Treatment |
|---|---|
| Upper motor neuron (detrusor overactivity) | Antimuscarinic agents |
| Lower motor neuron (retention/dribbling) | Clean intermittent catheterization (CIC) + α-sympathomimetics |
| Refractory overactive bladder | Augmentation cystoplasty |
| Refractory outlet insufficiency | Endoscopic bulking agents, artificial urinary sphincter (AUS), bladder neck sling, or reconstruction |
Bowel dysfunction also requires characterization — anorectal manometry often reveals internal anal sphincter abnormalities → fecal incontinence management is equally important.
Neonatal/Perinatal Management
- Flat plate radiograph to confirm extent of sacral agenesis
- CT or MRI for full anatomical delineation
- Pediatric surgery and pediatric orthopedics consultation
- Long-term multidisciplinary follow-up required
Prognosis
- Significant orthopedic disability (comparable to paraplegia in severe cases), but mental function is preserved
- Sensation preserved at up to three dermatome levels lower than functional motor control
- Stool and urinary incontinence with recurrent UTIs are the principal long-term morbidities
- Early detection and management prevents social stigma and upper tract damage
Key Points
- High index of suspicion in children with incontinence/UTIs + short gluteal cleft + flattened buttocks
- Children of diabetic mothers are at increased risk
- MRI hallmark: sharp conus cutoff at T12
- Urodynamic pattern does NOT correlate with the number of absent vertebrae
- Currarino syndrome (sacral agenesis + presacral mass + anorectal malformation) → test for HLXB9 mutation
- Preconception poorly controlled diabetes is a modifiable risk factor
Sources: Campbell-Walsh-Wein Urology, pp. 815–818 | Creasy & Resnik's Maternal-Fetal Medicine, pp. 579–584 | Comprehensive Clinical Nephrology, 7th Ed., p. 746
This is a shared conversation. Sign in to Orris to start your own chat.