Compartment syndrome
Reading File
Finding Sources
Searching PubMed
"compartment syndrome" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Compartment Syndrome
Definition
Compartment syndrome is raised pressure within a closed fascial (osseofascial) space sufficient to compromise tissue perfusion, leading to ischemia and irreversible damage to the muscles and nerves within that compartment. - Bailey and Love's Short Practice of Surgery 28th Ed.
Pathophysiology
The core mechanism is a self-reinforcing cycle:
- Increased pressure within a rigid fascial space (from bleeding, edema, or external constriction)
- Reduced microcirculatory perfusion - capillary pressure is exceeded
- Tissue ischemia triggers cellular anoxia and cell death
- Reperfusion (when it occurs) adds further injury via oxygen free radicals, lipid peroxidation, and intracellular calcium influx, causing more edema and perpetuating the cycle
The result is progressive muscle and nerve necrosis. - ROSEN's Emergency Medicine, Current Surgical Therapy 14e
Causes
Increased Compartment Content
| Mechanism | Examples |
|---|---|
| Fracture / trauma | Closed long bone fracture (most common - 70%), crush injury, contusion (23%) |
| Vascular injury / reperfusion | Arterial repair, embolectomy, bypass grafting |
| Hemorrhage | Coagulation disorder, anticoagulation therapy |
| Burns | Circumferential third-degree burns, electrical burns |
| Intense muscle use | Exercise, seizures, eclampsia, tetany |
| Infiltration | IV contrast under pressure, intraosseous fluid leakage |
| Surgical positions | Lithotomy position, tuck position for lumbar surgery |
Decreased Compartment Volume
- Tight casts, dressings, or air splints
- Excessive traction on fractures
- Closure of fascial defects
Key pitfall: Compartment syndrome can occur with open fractures and with low-energy injuries. It is not exclusively a high-energy trauma complication.
Anatomy - Compartments
The most commonly affected regions are the leg (4 compartments) and forearm (3-4 compartments):
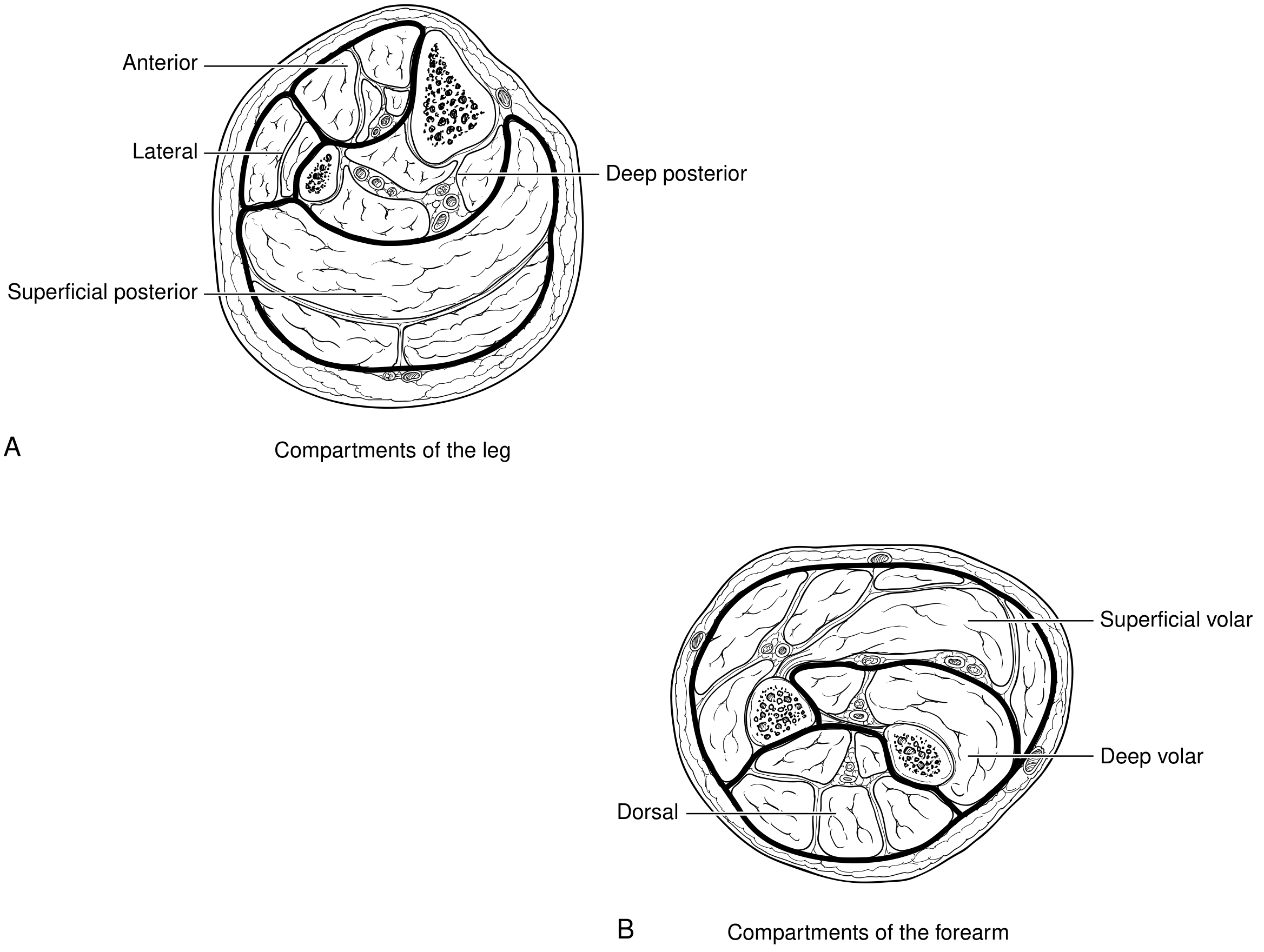
Leg (4 compartments):
- Anterior
- Lateral
- Deep posterior
- Superficial posterior
Forearm (3 compartments):
- Superficial volar
- Deep volar
- Dorsal
Other sites include the thigh, arm, hand, and foot. - Current Surgical Therapy 14e
Clinical Features - The "6 Ps"
Compartment syndrome is primarily a clinical diagnosis:
| Finding | Notes |
|---|---|
| Pain out of proportion | Most important early sign - severe, disproportionate to apparent injury |
| Pain on passive stretch | Passive stretching of muscles in the affected compartment reproduces pain |
| Pressure/tense compartment | Woody firmness on palpation |
| Paresthesia | Early neurological sign (nerve ischemia) |
| Paralysis | Late sign - indicates advanced muscle/nerve ischemia |
| Pallor / Pulselessness | Very late signs - do NOT wait for these |
Critical teaching point: Pulselessness is an extremely late and ominous sign. Absence of pulse deficit does NOT exclude compartment syndrome. Diagnosis must be made before paralysis and pulselessness appear. - Bailey and Love's
Elevated CPK and myoglobinuria are late markers of destruction and should not be used to establish the diagnosis. - Current Surgical Therapy 14e
Diagnosis
Clinical
Diagnosis is clinical in most cases. A patient with severe pain, tense compartment, and pain on passive stretch after relevant trauma requires urgent action.
Compartment Pressure Monitoring
Indicated when clinical assessment is unreliable - altered consciousness, head injury, intubated patients, uncooperative patients.
Measurement thresholds that mandate fasciotomy:
| Threshold | Value |
|---|---|
| Absolute compartment pressure | ≥ 30 mmHg |
| Delta pressure (ΔP = diastolic BP - compartment pressure) | ≤ 30 mmHg (Bailey and Love) |
| More conservative ΔP threshold (some sources) | < 10 mmHg |
Measure all compartments of the affected limb at multiple sites near (not in) the fracture. - Bailey and Love's, Current Surgical Therapy 14e
Treatment
Immediate (Emergency)
- Split and bivalve any cast/dressing down to the skin - removes external pressure
- Limb positioning - at the level of the heart (do NOT elevate above heart level, as this reduces perfusion pressure)
- Remove all circumferential wrapping
Definitive - Fasciotomy
Emergent fasciotomy is the only definitive treatment. All compartments of the affected limb must be released.
Lower leg: Four-compartment fasciotomy via medial and lateral incisions
Forearm: Release of volar and dorsal forearm compartments; if hand is involved, carpal tunnel release and hand fasciotomies may be added (consult hand surgery)
Post-fasciotomy:
- Wounds are left open
- Vacuum-assisted closure (VAC) devices reduce muscle edema
- Early closure or incomplete skin release must be avoided - can cause muscle necrosis
Prophylactic Fasciotomy
Recommended when:
- Ischemia time > 6 hours prior to revascularization
- Limb edema observed after reperfusion
- Combined arterial and venous injury
- Significant associated soft tissue injury
Post-fasciotomy Monitoring
- Serial neurovascular exams
- Monitor for rhabdomyolysis - aggressive IV fluid resuscitation targeting urine output > 100 mL/hr until CPK < 5,000 U/L
- Urine alkalization with bicarbonate in significant tissue damage
- Monitor for renal failure (acute tubular necrosis from myoglobinuria)
- Correct acidosis and electrolyte imbalances (intracellular K⁺ leak)
Key Complications if Untreated
- Irreversible muscle necrosis - Volkmann's ischemic contracture
- Peripheral nerve injury - permanent sensory/motor deficit
- Infection and gangrene
- Myoglobinuria - acute tubular necrosis - renal failure
- Limb loss
- Death (from systemic complications)
Special Situations
| Scenario | Notes |
|---|---|
| Open fractures | Do NOT assume the open wound decompresses the compartment - still monitor closely |
| Altered consciousness / sedated patients | Cannot perform clinical exam - measure pressures directly |
| Pediatric patients | High index of suspicion; pain out of proportion is the key early finding |
| Reperfusion after vascular repair | Prophylactic fasciotomy often warranted after ischemia > 6 hours |
| Intraosseous access | Fluid extravasation can cause lower leg compartment syndrome - inspect insertion site frequently |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., ROSEN's Emergency Medicine (Concepts and Clinical Practice), Current Surgical Therapy 14e, Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.