Dm complications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to provide a detailed, well-structured answer on DM complications.
Complications of Diabetes Mellitus
DM complications are divided into microvascular (directly caused by hyperglycemia-driven small vessel damage) and macrovascular (accelerated atherosclerosis of large vessels). Four core biochemical mechanisms underlie all chronic complications: formation of advanced glycation end-products (AGEs), activation of protein kinase C (PKC), disturbances in the polyol pathway, and overload of the hexosamine pathway (Robbins, Cotran & Kumar Pathologic Basis of Disease).
I. MICROVASCULAR COMPLICATIONS
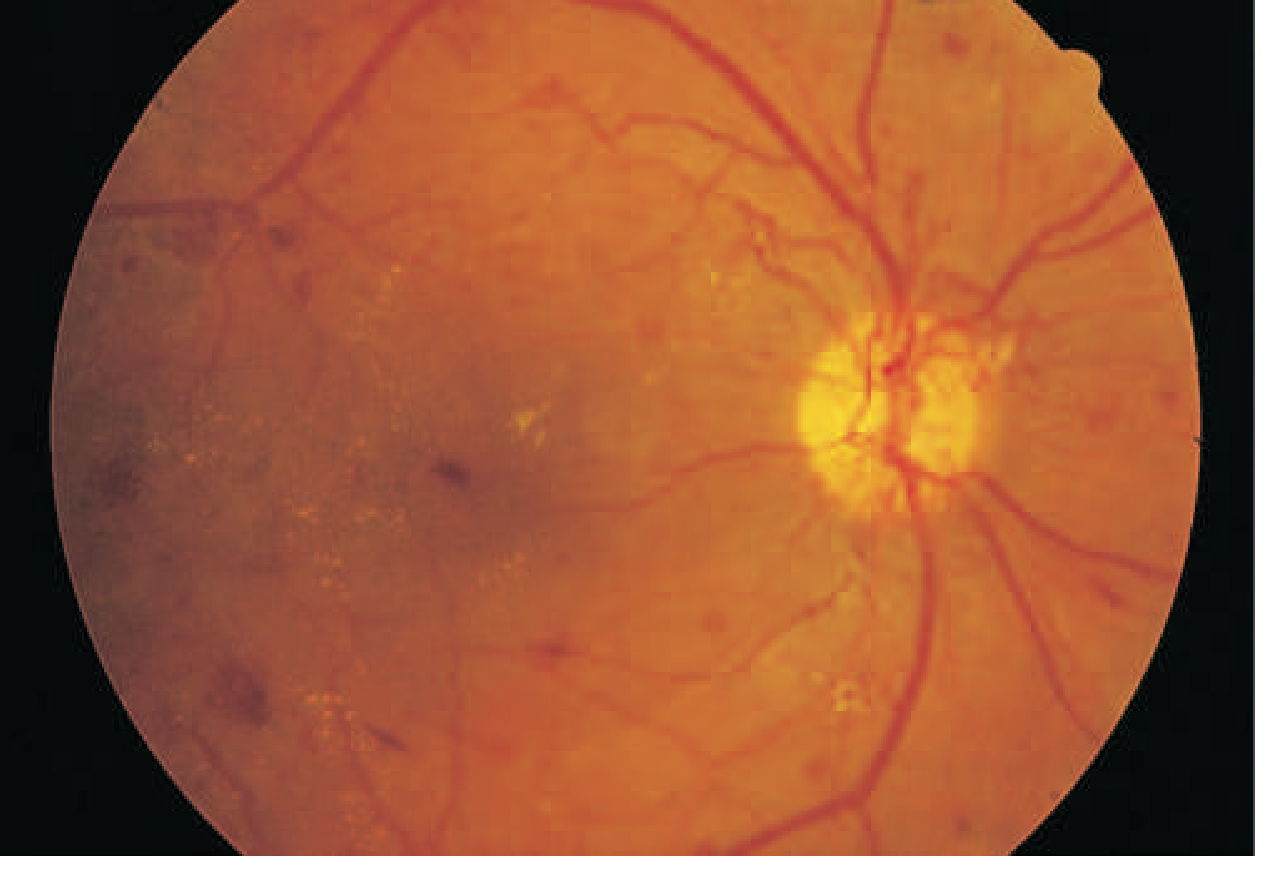
1. Diabetic Retinopathy (DR)
DR is the leading cause of new blindness in adults aged 20-74 in the US, and the 5th leading cause of severe vision loss worldwide.
Classification:
| Stage | Features |
|---|---|
| Nonproliferative (NPDR) | Retinal microaneurysms, blot hemorrhages, cotton-wool spots, venous caliber changes, intraretinal microvascular abnormalities |
| Proliferative (PDR) | Neovascularization near optic disc/macula - hallmark feature; leads to vitreous hemorrhage, fibrosis, retinal detachment |
Macular edema can occur in either stage and is associated with significant risk of moderate visual loss over 3 years.
Key risk factors: Duration of DM, degree of glycemic control, hypertension, nephropathy, dyslipidemia.
Other ocular complications: Cataracts (earlier onset), glaucoma, optic neuropathy, extraocular muscle paresis, dyskinetic pupils.
Screening:
- T1DM: begin 3-5 years after diagnosis (or at puberty onset), then annually
- T2DM: at time of diagnosis, then annually
- Dilated fundus exam by ophthalmologist/optometrist
Treatment:
- Tight glycemic control (primary prevention/slowing progression)
- BP control (ACE inhibitor or ARB)
- Fenofibrate for dyslipidemia (beneficial in DR)
- Anti-VEGF injections (bevacizumab, ranibizumab) - preferred over laser for macular edema; also effective for proliferative DR
- Panretinal laser photocoagulation - for proliferative DR
- Vitrectomy - for vitreous hemorrhage or retinal detachment
Note: GLP-1 receptor agonists (e.g., semaglutide) may transiently worsen established retinopathy with rapid glycemic normalization.
(Harrison's Principles of Internal Medicine, 22E; Washington Manual of Medical Therapeutics)
2. Diabetic Nephropathy
The leading cause of CKD and end-stage renal disease (ESRD) requiring dialysis. Affects ~20-40% of diabetic patients.
Pathogenesis: Chronic hyperglycemia causes glomerular hyperperfusion and hyperfiltration → basement membrane thickening, mesangial expansion, glomerulosclerosis → progressive albuminuria and declining GFR.
Natural history (initially described for T1DM):
- Early: glomerular hyperperfusion, raised eGFR
- Years 1-5: basement membrane thickening, glomerular hypertrophy, mesangial expansion - eGFR normalizes
- Later: albuminuria develops, then GFR declines - changes likely irreversible at this stage
Screening:
- Urine albumin-to-creatinine ratio (UACR) on spot specimen + eGFR annually
- T1DM: start 5 years after diagnosis; T2DM: at diagnosis
- Albuminuria confirmed on 2-3 occasions over 3-6 months
Definitions:
- Normal: UACR <30 mg/g
- Moderate (microalbuminuria): 30-299 mg/g
- Severe (macroalbuminuria): ≥300 mg/g
Other renal issues: Type IV RTA (hyporeninemic hypoaldosteronism) causing hyperkalemia and acidemia.
Treatment:
- Target BP <130/80 mmHg
- ACE inhibitor or ARB - first-line for all DM + HTN; also used even in normotensive patients with albuminuria
- SGLT2 inhibitors (empagliflozin, canagliflozin) - proven reduction in CKD progression; can be initiated down to eGFR 30 mL/min/1.73m²
- Finerenone (nonsteroidal mineralocorticoid receptor antagonist) - reduces CKD progression and CV events with less hyperkalemia than spironolactone
- Dietary protein: 0.8 g/kg/day
- Avoid nephrotoxins
(Harrison's Principles of Internal Medicine, 22E; Washington Manual)
3. Diabetic Neuropathy
Distal symmetric polyneuropathy (DPN) is the most common neuropathy in developed countries and accounts for more hospitalizations than all other diabetic complications combined. Responsible for 50-75% of nontraumatic lower limb amputations.
Classification:
| Type | Features |
|---|---|
| Subclinical | Abnormal electrodiagnostic/quantitative sensory testing only |
| Distal symmetric polyneuropathy (DPN) | Classic "stocking-glove" paresthesias, burning pain, numbness; major risk factor for foot ulceration and Charcot arthropathy |
| Autonomic neuropathy | Cardiovascular, GI, genitourinary, sudomotor |
| Focal/multifocal | Cranial nerve palsies, truncal radiculopathy, diabetic amyotrophy |
Autonomic neuropathy manifestations:
- Cardiovascular: Resting tachycardia, orthostatic hypotension, exercise intolerance, silent MI, sudden death
- GI (diabetic gastroparesis): Nausea, vomiting, bloating, intractable gastroparesis
- GU: Erectile dysfunction, neurogenic bladder, retrograde ejaculation
- Sudomotor: Anhidrosis, gustatory sweating
Screening: Annual foot exam with 10g monofilament, 128 Hz tuning fork or pinprick, temperature testing.
Treatment of painful DPN:
- Tricyclic antidepressants (amitriptyline 10-150 mg at bedtime)
- Gabapentin 900-3600 mg/day
- Pregabalin 150-300 mg/day
- Duloxetine (SNRIs)
- Topical capsaicin 0.075%
- α-Lipoic acid 600 mg TID (antioxidant; evidence in early DPN)
- Vitamin B12 supplementation if deficient
Treatment of autonomic complications:
- Orthostatic hypotension: Compressive stockings, fludrocortisone 0.1-0.3 mg/day, high-salt diet
- Gastroparesis: Small frequent meals, metoclopramide, erythromycin (short-term)
(Washington Manual; Harrison's; Goldman-Cecil Medicine)
II. MACROVASCULAR COMPLICATIONS
Coronary heart disease (CHD), stroke, and peripheral vascular disease (PVD) together account for 80% of deaths in persons with diabetes.
1. Coronary Heart Disease (CAD)
- Occurs at a younger age than in non-diabetics
- Often atypical presentations (silent ischemia due to autonomic neuropathy)
- MI carries worse prognosis; PCI gives less satisfactory results
- Increased risk of both ischemic and non-ischemic heart failure, and sudden death
2. Heart Failure
- Hazard ratio for HF is ~2.5 in diabetics vs non-diabetics
- Diabetes affects myocardial structure and function independently of CAD - causing left ventricular concentric remodeling, hypertrophy, and impaired myocardial energetics (diabetic cardiomyopathy)
- SGLT2 inhibitors and GLP-1 receptor agonists reduce HF hospitalizations and CV mortality in T2DM with established CVD
3. Stroke and Peripheral Arterial Disease (PAD)
- Increased risk of ischemic stroke
- PAD leads to claudication, rest pain, and critical limb ischemia contributing to amputations
Risk factors for macrovascular disease in DM: Insulin resistance, hyperglycemia, albuminuria, hypertension, hyperlipidemia, cigarette smoking, obesity.
Macrovascular prevention:
- A1C target <7% (especially in early years; avoid hypoglycemia)
- BP <140/90 mmHg (or <130/80 if tolerable)
- High-intensity statin for all patients with known CVD
- Aspirin 81-325 mg/day for secondary prevention; consider in primary prevention for age >40 with DM
- Smoking cessation; weight loss
(Washington Manual of Medical Therapeutics)
III. OTHER COMPLICATIONS
| Complication | Notes |
|---|---|
| Diabetic foot | Combination of neuropathy + PAD + infection; leading cause of nontraumatic amputation |
| Infections | Increased susceptibility (impaired neutrophil function); UTIs, soft tissue infections, mucormycosis, malignant otitis externa |
| Dermatologic | Necrobiosis lipoidica diabeticorum, acanthosis nigricans, diabetic dermopathy |
| Oral | Periodontal disease, xerostomia |
| Cognitive impairment | Increased risk of dementia, especially with recurrent hypoglycemia |
Summary Table
| Category | Complication | Key Mechanism | Screening/Prevention |
|---|---|---|---|
| Microvascular | Retinopathy | Pericyte loss, VEGF-driven neovascularization | Annual dilated eye exam |
| Nephropathy | Glomerular hyperfiltration, mesangial expansion | Annual UACR + eGFR | |
| Neuropathy | Metabolic/ischemic nerve damage | Annual foot exam | |
| Macrovascular | CAD, HF, Stroke, PAD | Accelerated atherosclerosis | Statin, aspirin, BP control |
Tight glycemic control remains the single most effective intervention to prevent and slow the progression of all microvascular complications, and SGLT2 inhibitors + GLP-1 agonists have transformed outcomes in both nephropathy and cardiovascular disease in T2DM.
This is a shared conversation. Sign in to Orris to start your own chat.