Detailed discussion on aph and placenta previa and PAS in pg level from standard text books like williams and others recent Update from international journals and articles
Reading File
Finding Sources
Finding Sources
Searching PubMed
placenta previa placenta accreta spectrum management
Finding Sources
Finding Sources
Searching PubMed
"placenta accreta spectrum" diagnosis treatment outcomes
Reading File
Reading File
Reading Article
PMID: 38969992
Reading File
Reading File
Reading Article
PMID: 39884567
Reading File
Reading File
Reading Article
PMID: 40472373
Reading File
Finding Sources
Reading Article
PMID: 40552443
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading Article
PMID: 37401769
Loading Image
Antepartum Hemorrhage (APH), Placenta Previa, and Placenta Accreta Spectrum (PAS): A Comprehensive PG-Level Discussion
Sources: Creasy & Resnik's Maternal-Fetal Medicine (8e), Morgan & Mikhail's Clinical Anesthesiology (7e), Barash Clinical Anesthesia (9e), Rosen's Emergency Medicine, Miller's Anesthesia (10e), Grainger & Allison's Diagnostic Radiology; supplemented with recent systematic reviews and meta-analyses (2023-2026).
PART I: ANTEPARTUM HEMORRHAGE (APH)
Definition and Epidemiology
Antepartum hemorrhage is defined as bleeding from the genital tract after 20 weeks of gestation and before delivery of the baby. It complicates 3-5% of all pregnancies and remains a leading contributor to both maternal and perinatal mortality worldwide. - Barash Clinical Anesthesia, 9e
The causes can be broadly categorized as:
| Category | Conditions |
|---|---|
| Placental causes | Placenta previa, placental abruption, vasa previa |
| Local (non-placental) causes | Cervicitis, cervical ectropion, polyps, carcinoma, trauma |
| Indeterminate | ~50% of APH cases |
The most clinically significant causes are placenta previa and placental abruption (abruptio placentae).
Differential Diagnosis of APH
The foremost task when a pregnant woman presents with second/third trimester bleeding is exclusion of placenta previa by ultrasound. No digital vaginal examination should ever be performed in any woman after 20 weeks until placenta previa is excluded - this rule is absolute, as it can precipitate catastrophic hemorrhage. - Creasy & Resnik, Rosen's Emergency Medicine
PART II: PLACENTA PREVIA
Definition and Classification
Placenta previa occurs when the placental implantation covers the internal cervical os. - Creasy & Resnik
Low-lying placenta is defined when the placental edge lies within 2 cm of the internal os but does not cover it.
Important terminology update: The previous categories of complete, partial, and marginal placenta previa are no longer recommended. Current NICHD/SMFM consensus terminology uses:
- "Placenta previa" = placenta covering the internal os
- "Low-lying placenta" = placental edge within 2 cm but not covering the os
- "Normal" = placental edge >20 mm from the internal os
- Creasy & Resnik; Key Points section
Incidence
- Placenta previa affects approximately 0.5% of all third-trimester pregnancies (1 in 200-250 pregnancies)
- It is diagnosed in 10% of mid-trimester sonograms, but the vast majority resolve due to placental migration (trophotropism)
- At least 90% of placentas identified as low-lying or previa in early pregnancy ultimately resolve by the third trimester
- Creasy & Resnik; Textbook of Family Medicine 9e
Pathogenesis - "Placental Migration"
The underlying cause is unknown. There is a clear association with endometrial damage and uterine scarring. The apparent "migration" of the placenta away from the cervix occurs because:
- The placenta grows toward better blood supply at the uterine fundus (trophotropism)
- The distal portions closer to the lower segment with poor blood supply undergo regression and atrophy
- Differential growth of the lower uterine segment with advancing gestation further increases the distance between the placental edge and the cervix
Bleeding occurs because development of the lower uterine segment and cervical effacement force placental separation from the underlying decidua. - Creasy & Resnik
Risk Factors
| Risk Factor | Relative Risk Increase |
|---|---|
| Previous placenta previa | 8x |
| Previous cesarean section | 1.5-15x (dose-dependent with number of CS) |
| Previous suction curettage | 1.33x |
| Age >35 years | 4.73x |
| Age >40 years | 9x |
| Multiparity | 1.1-1.73x |
| Asian race | 1.93x |
| Cigarette smoking | 1.4-3.3x |
From Creasy & Resnik's MFM, Table
Other risk factors include prior myomectomy, endometrial ablation, uterine radiation, IVF conception, and short interpregnancy interval.
Clinical Features
- Classic presentation: Painless, bright-red vaginal bleeding, usually after the 28th week (7th month). The painless nature distinguishes it from abruption.
- Several small "herald bleeds" may precede a major hemorrhage
- In up to 10% of cases, there is no bleeding until onset of labor
- Abnormal fetal lie (transverse, oblique) is common because the previa occupies the lower pole of the uterus, preventing head engagement
Diagnosis
Transvaginal ultrasound (TVUS) is the gold standard. It is safe (confirmed in multiple studies), accurate, and superior to transabdominal scanning for localizing the placental edge relative to the internal os.
- If placental edge is >20 mm from the internal os → report as "normal"
- If placental edge is within 20 mm but not covering the os → report as "low-lying"
- Placenta covering the internal os → "placenta previa"
- TVUS has high sensitivity and specificity; transabdominal scanning frequently overestimates proximity due to bladder distension and posterior placentas
Associated Conditions
- Placenta accreta spectrum (critically important - see Part III)
- Vasa previa
- Fetal malpresentation
- Preterm birth
- Intrauterine growth restriction (IUGR)
Management of Placenta Previa
Antepartum (Expectant) Management
In women without active bleeding and with an immature fetus:
- Inpatient vs outpatient: Evidence suggests outpatient management is reasonable in selected stable patients without active bleeding. Inpatient admission is indicated for active bleeding, contractions, or remote location.
- Pelvic rest (no intercourse, no vaginal examinations)
- Avoidance of strenuous activity
- IV access and crossmatched blood should be available
- Tocolysis may be used with caution for preterm uterine contractions to prolong gestation (tocolysis is generally considered safe in the context of placenta previa, though evidence is limited)
- Antenatal corticosteroids if preterm delivery anticipated before 34 weeks
- Serial ultrasound surveillance
Timing of Delivery
- Uncomplicated placenta previa: deliver at 36-37 weeks (planned cesarean section)
- With placenta accreta: earlier delivery, typically 34-37 weeks (see below)
- Amniocentesis for fetal lung maturity imposes unnecessary delay and is NOT recommended in current practice - Creasy & Resnik
Mode of Delivery
Cesarean section is mandatory for placenta previa. Vaginal delivery is absolutely contraindicated. - Barash Clinical Anesthesia
Anesthetic considerations:
- Neuraxial anesthesia is preferred (lower blood loss, less need for transfusion compared to general anesthesia)
- General anesthesia is reserved for hemodynamic instability or patient refusal
- Both uterine atony and placenta accreta can cause massive postpartum hemorrhage in these cases
Management of Acute Hemorrhage from Placenta Previa
- Stabilize the patient: IV access x2, full blood count, coagulation screen, crossmatch
- Ultrasound to confirm diagnosis and fetal wellbeing
- If hemorrhage is life-threatening or fetus is mature: emergency cesarean section
- Blood transfusion and massive hemorrhage protocol if needed
- Uterotonic agents, balloon tamponade, B-Lynch suture, uterine artery ligation, or hysterectomy for refractory bleeding
Recent Update (2025 Meta-analysis, PMID 40472373 - Bonanni et al., Obstet Gynecol): Even a diagnosis of low-lying placenta carries a twofold increased risk of postpartum hemorrhage (PPH) compared to normal placentation (RR 2.10, 95% CI 1.02-4.35). The incidence of PPH was 16% in low-lying placenta 1-20 mm from the os vs. 5.8% in non-low-lying cases. Critically, PAS disorders affected 9% of all low-lying placenta cases - emphasizing the need for vigilant assessment even in "low-lying" placentas.
PART III: PLACENTA ACCRETA SPECTRUM (PAS)
Terminology and Classification
The term Placenta Accreta Spectrum (PAS) has replaced older terms like "morbidly adherent placenta." It encompasses a spectrum of abnormal placental invasion:
| Type | Definition | Frequency |
|---|---|---|
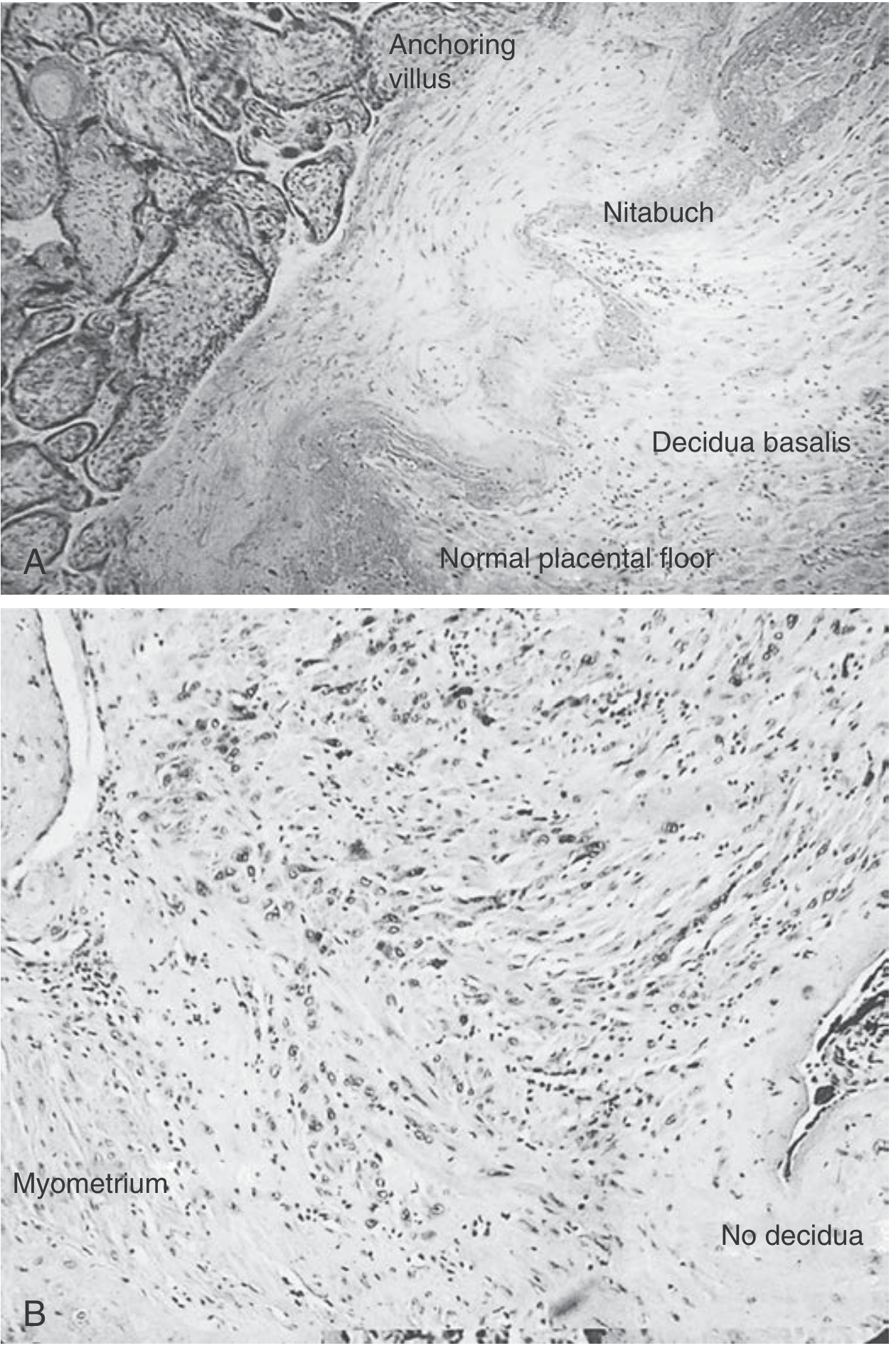
| Placenta accreta | Trophoblast attached to myometrium without intervening decidua (invasion into muscle but not full thickness) | 82% |
| Placenta increta | Invasion into full thickness of myometrium but not beyond serosa | 12% |
| Placenta percreta | Invasion beyond uterine serosa, may involve bladder or other pelvic organs | 6% |
Creasy & Resnik's MFM, Histologic types
Pathophysiology
The pathologic hallmark is absence of the Nitabuch fibrinoid layer - the normal boundary of placental implantation. In normal implantation, trophoblastic villi encroach on but do not penetrate through this membrane. In PAS, absence of decidua basalis allows trophoblasts to invade directly into the myometrium.
Incidence and Trends
- Incidence is rising sharply due to the global rise in cesarean section rates
- Current estimates: 1 in 300-500 pregnancies in recent cohorts
- Historical incidence (1970s): 1 in 30,000
- Current incidence (population-based): approximately 3 per 1,000 deliveries
- Creasy & Resnik; Rosen's Emergency Medicine
Risk Factors - The Critical Synergy of Previa + Prior CS
The most important risk factors are placenta previa + prior cesarean delivery. These two together create exponentially increasing risk:
| Prior Cesareans | Risk of PAS with Previa |
|---|---|
| 1 (primary CS) | ~3% |
| 2 prior CS | ~11% |
| 3 prior CS | ~40% |
| 3+ prior CS with previa | >60% |
Creasy & Resnik; Barash Clinical Anesthesia: "The risk of placenta accreta in women with previa increases from 3% in primary cesarean deliveries to 61% in patients with three prior cesareans."
Other risk factors: prior curettage, myomectomy, endometrial ablation, IVF, pelvic radiation, short interpregnancy interval, advanced maternal age, smoking, and high parity.
Ultrasound Diagnosis of PAS
TVUS is the primary modality. Sensitivity approximately 80-90% in referral centers, though one blinded expert study showed sensitivity of only 55%, highlighting operator-dependence. Characteristic features include:
| Ultrasound Marker | Definition |
|---|---|
| Placental lacunae | Irregular hypoechoic spaces within placenta ("Swiss cheese" or "moth-eaten" appearance); high velocity (>15 cm/s) turbulent flow on Doppler |
| Loss of retroplacental hypoechoic zone | Loss of the normal "clear zone" representing the decidua; myometrial thickness <1 mm |
| Abnormal uterine contour (placental bulge) | Placental tissue distorting the uterine serosa outward |
| Exophytic mass | Placental tissue extruding beyond the uterine serosa |
| Bridging vessels | Vessels extending from placenta across the myometrium beyond the uterine serosa |
- Color flow Doppler shows turbulent flow in lacunar spaces and increased vascularity at the placenta-uterus interface
- First-trimester diagnosis is possible and is particularly accurate in cases of cesarean scar ectopic pregnancy
- All women with clinical risk factors should be referred to a unit with appropriate expertise in PAS diagnosis
Creasy & Resnik, Table of Markers of Placenta Accreta Sequence
Role of MRI in PAS
MRI is used to confirm diagnosis or delineate the extent of invasion, particularly for posterior placentas or suspected percreta. It has reported high accuracy but studies are more prone to ascertainment bias than ultrasound studies. MRI has not been shown to reliably improve accuracy beyond well-performed TVUS, but it provides useful additional anatomical information for surgical planning, especially in suspected bladder or parametrial involvement.
- No adverse outcome has been found from MRI without gadolinium during pregnancy
- Creasy & Resnik
Antenatal Surveillance and Multidisciplinary Care
Pre-delivery diagnosis combined with planned delivery at a center of excellence by a multidisciplinary team (MFM, gynecologic oncology, urology, interventional radiology, anesthesiology, neonatology, blood bank) is the single most important intervention to reduce maternal morbidity and intraoperative blood loss. Studies consistently show markedly reduced morbidity when accretas are managed at regional referral centers.
Timing of Delivery in PAS
- Planned delivery at 34-35 weeks (Creasy & Resnik recommendation) after antenatal corticosteroids for fetal lung maturity
- Decision analysis supports 34-37 weeks without amniocentesis for lung maturity
- Earlier delivery in cases with cervical involvement or suspected percreta
- Emergency delivery if life-threatening hemorrhage
Surgical Management of PAS
Standard Approach: Cesarean Hysterectomy
The preferred and generally recommended treatment is cesarean delivery followed by total abdominal hysterectomy (cesarean hysterectomy). Key surgical principles:
- Fundal uterine incision - to avoid cutting through placenta and triggering hemorrhage before clamping the cord
- Cord is clamped after delivery of the baby
- Placenta is left in situ (do not attempt manual removal, which will precipitate massive hemorrhage)
- Proceed to total abdominal hysterectomy with the placenta still in place
- Complex dissection of lower uterine segment and parametrial areas may be required
- Pelvic surgeon capable of wide resection should be part of the team
Conservative Management (Uterus-Sparing Approaches)
For women who wish to preserve fertility, conservative approaches have been developed:
a) Placenta left in situ (expectant conservative management): The placenta is entirely left in situ and allowed to resorb over weeks to months. Uterine artery embolization (UAE) is commonly used adjunctively.
b) Local/myometrial resection: Surgical resection of the area of abnormal placentation with repair of the uterine defect.
Recent Meta-analysis Evidence on Conservative vs Hysterectomy:
Pan et al. 2024 (BMC Pregnancy Childbirth, PMID 38969992) - 8 studies, meta-analysis comparing conservative management vs. cesarean hysterectomy:
- Conservative management: less estimated blood loss (WMD -1624 mL), fewer units of packed RBCs (WMD -2.37 units), shorter operating time (WMD -74 min)
- Lower risks of bladder injury (RR 0.24), ICU admission (RR 0.24), coagulopathy (RR 0.20)
- BUT increased risk of endometritis (RR 10.91) and readmission (RR 8.99)
- 25% ultimately required hysterectomy (primary or delayed)
- UAE was used in 78% of conservatively managed cases
- Conclusion: Conservative management is an effective alternative when fertility preservation is desired, with informed consent about limitations
Hessami et al. 2025 (AJOG, PMID 39884567) - 16 studies, 2,300 women - the largest meta-analysis:
- Cesarean hysterectomy associated with significantly higher blood loss vs. placenta in situ (mean difference +974 mL) and vs. local resection (+740 mL)
- Higher risk of genitourinary injury with hysterectomy (OR 3.79 vs. placenta in situ; OR 4.11 vs. local resection)
- Higher ICU admission with hysterectomy vs. placenta in situ (OR 7.98)
- No difference in GI injury or thromboembolic events
- Conclusion: Conservative management associated with reduced surgical morbidity
Pinto et al. 2026 (IJGO, PMID 40552443) - 49 studies, 2,666 patients:
- Majority (69.4%) treated with myometrial resection and repair
- Overall hysterectomy rate when conservative surgery was attempted: 11.2%
- Urologic complication rate: 8.8%
- Mean blood loss: ~1,800 mL in both myometrial resection and other conservative approaches
- Conclusion: Uterine-sparing surgery feasible in high percentage of PAS patients with outcomes comparable to hysterectomy
Adjunctive Hemostatic Techniques
- Balloon occlusion of internal iliac or aortic vessels: Preoperative placement of balloon-tipped catheters via femoral artery approach under fluoroscopy. Benefit remains controversial - published studies show no proven benefit and reports of embolic complications. The utility is unclear due to variable timing of deployment. A comprehensive literature review concluded larger studies are needed.
- Cell salvage (intraoperative autologous blood collection)
- Uterine artery embolization (UAE): Used extensively as an adjunct in conservative management
- Massive transfusion protocol activation: Should be planned preoperatively
Urological Complications - Updated Evidence
Lucidi et al. 2023 (Ultrasound Obstet Gynecol, PMID 37401769) - 62 studies, meta-analysis:
- Overall urological complications in PAS surgery: 15.2%
- Cystotomy (total): 13.5% (intentional 7.7%, unintentional 7.2%)
- By severity: accreta/increta: 9.4%; percreta: 38.5%
- By approach: hysterectomy 19.4%; conservative surgery 12.2%
- Emergency vs. planned: 24.6% vs. 15.4%
- Key message: Urological morbidity is high, especially for percreta and emergency cases. Standardized PAS diagnosis protocols are needed.
PART IV: ABRUPTIO PLACENTAE (for completeness in APH discussion)
Definition
Abruptio placentae (placental abruption) is the premature separation of a normally sited placenta after 20 weeks of gestation. It is distinct from placenta previa in that the placenta is normally implanted.
Epidemiology
- Clinically recognized abruption: approximately 1% of all pregnancies
- Abruption causing fetal death: 1 in every 420 deliveries
- If placentas are routinely examined postdelivery, pathological evidence of abruption may be found in up to 4% of cases (most subclinical)
- Incidence has increased by approximately 25% in the USA over recent decades, with a disproportionate increase in Black women
- Incidence peaks at 24-26 weeks' gestation
- Approximately 10% of all preterm births are secondary to abruption
- Perinatal mortality ranges from 9-12% in developed countries; maternal mortality <1%
- Creasy & Resnik
Pathogenesis
The fundamental event is hemorrhage between the decidua basalis and placenta. The hematoma dissects the decidua, progressively separating the placenta from its implantation site, reducing the area available for fetal gas exchange and nutrition.
The underlying mechanism in many cases is vasospasm of abnormal maternal arterioles, often as a manifestation of defective placentation. Evidence of a preexisting placental pathology is inferred from:
- Low PAPP-A levels (placenta with impaired function)
- Poor trophoblastic invasion
- Abnormal uterine artery Doppler (inadequate remodeling of maternal arterioles)
- Strong association with preeclampsia, IUGR, and abruption (all sharing a common placental pathology pathway)
Acute shearing forces also cause abruption (trauma, rapid deceleration, sudden decompression of polyhydramnios).
As abruption progresses:
- Fetal hypoxia → fetal death (>50% separation → likely fetal death)
- Activation of coagulation cascade → DIC
- Hemorrhagic shock → worsening DIC → downward spiral
- Bleeding into myometrium → Couvelaire uterus (atonic, woody-hard) → increases risk of postpartum hemorrhage
Types
| Type | Description |
|---|---|
| Revealed | Blood tracks down between membranes and exits via cervix - external bleeding |
| Concealed | Blood accumulates behind placenta, no external bleeding; more dangerous |
| Mixed | Elements of both (most common) |
- 10% of abruptions are concealed - external bleeding is an unreliable guide to severity
Risk Factors for Abruption
- Chronic hypertension and preeclampsia (most important)
- Previous abruption (recurrence risk up to 20-fold increased)
- Cigarette smoking
- Cocaine and other vasoactive drug use
- Trauma (motor vehicle accidents, domestic violence)
- Multiple gestation
- Preterm premature rupture of membranes (pPROM)
- Thrombophilias and hyperhomocysteinemia
- Low PAPP-A (<5th percentile) on first-trimester screening
- Elevated second-trimester AFP (>2 MoM)
- Elevated second-trimester hCG (>3 MoM)
- Creasy & Resnik
Clinical Features
The classic triad is:
- Vaginal bleeding (dark, clotted blood - contrast with the bright-red painless bleeding of previa)
- Abdominal/uterine pain and tenderness (the key differentiator from previa)
- Uterine hypertonicity
Additional features:
- Uterine contractions (may precipitate preterm labor)
- Fetal compromise/distress on CTG
- With posterior abruption: severe back pain as the only symptom
- Massive concealed abruption: severe pain, hard "board-like" tonically contracting uterus, fetal death - classically associated with severe preeclampsia or cocaine use
- Coagulopathy (DIC) in severe cases
Diagnosis
Abruption remains a clinical diagnosis - imaging is useful primarily to exclude placenta previa. Ultrasound sensitivity for detecting abruption is limited:
- Fresh clot may be isoechoic to placenta
- Retroplacental hematoma is visible in only about 25% of cases on ultrasound
- A negative ultrasound does NOT rule out abruption
- Creasy & Resnik; Key Points: "Abruption remains a clinical diagnosis - imaging is useful only to exclude placenta previa"
Investigations:
- Full blood count, coagulation profile (PT, APTT, fibrinogen - fibrinogen <200 mg/dL suggests severe abruption, <150 mg/dL indicates DIC)
- Kleihauer-Betke test in Rh-negative women to quantify fetomaternal hemorrhage
- Continuous CTG
- Renal function (acute tubular necrosis from prolonged hypoperfusion)
Management of Abruption
The approach depends on gestational age, degree of compromise, and whether the fetus is viable:
Mild abruption, remote from term, stable fetus:
- Expectant management with close inpatient observation
- Serial ultrasound and fetal monitoring
- Antenatal corticosteroids if <34 weeks
Moderate abruption:
- Artificial rupture of membranes (stabilizes fetal presenting part against placenta, reduces pressure)
- Oxytocin augmentation if in labor
- Continuous fetal monitoring
- Urgent CS if non-reassuring fetal status
Severe abruption:
- Emergency cesarean section if fetus is alive
- If fetal death has occurred and mother is stable: vaginal delivery may be attempted (avoids CS in setting of DIC)
- Aggressive resuscitation, massive transfusion protocol
- Coagulation replacement (FFP, cryoprecipitate, platelets)
- Manage Couvelaire uterus: uterotonics, B-Lynch, hysterectomy if necessary
Prevention of recurrence:
- Modify risk factors: treat hypertension, smoking cessation, substance abuse cessation
- Folate supplementation for proven hyperhomocysteinemia
- Creasy & Resnik
PART V: CLINICALLY IMPORTANT INTERRELATIONSHIPS
The APH-Previa-PAS Triangle
Understanding these three conditions as an interconnected clinical entity is essential:
- Placenta previa is the principal risk factor for PAS (co-occurrence >60% with 3+ prior CS)
- PAS is the most common cause of emergency peripartum hysterectomy
- APH in a patient with previa should always prompt evaluation for PAS before any surgical intervention
- Low-lying placenta that resolves clinically still carries elevated PPH risk: 8% PPH rate even when resolved, and PAS affects 9% of all low-lying placenta cases - Bonanni et al. 2025
- All women with prior cesarean sections and current placenta previa must be evaluated for PAS - Creasy & Resnik Key Points
Key Points Summary (Examination-Level)
| Point | Details |
|---|---|
| TVUS is mandatory | For any woman >20 weeks with vaginal bleeding, before any vaginal exam |
| No digital examination | Absolute contraindication until previa excluded |
| Terminology update | Abandon marginal/partial previa; use "previa" vs. "low-lying" |
| Trophotropism | Explains "migration" - not true movement but differential growth |
| PAS risk stratification | Use previa + number of prior CS to stratify |
| Delivery timing | Uncomplicated previa: 36-37 wk; PAS: 34-35 wk |
| Conservative vs hysterectomy | Conservative PAS: lower blood loss, fewer urologic complications, but 25% need eventual hysterectomy; increased endometritis/readmission |
| Abruption diagnosis | Clinical, not imaging; ultrasound only excludes previa |
| Couvelaire uterus | Myometrial bleeding in severe abruption; causes atony |
| Centers of excellence | Mandatory for planned PAS surgery - outcomes are dramatically better |
Recent Literature Updates (2023-2026) Summary
| PMID | Authors/Year | Key Finding |
|---|---|---|
| 39884567 | Hessami et al. 2025 (AJOG) | Conservative PAS management: lower blood loss (+974 mL less than hysterectomy), fewer GU injuries (OR 3.79-4.11 lower), better ICU outcomes |
| 38969992 | Pan et al. 2024 (BMC Preg) | Conservative: 25% eventual hysterectomy; UAE used in 78%; shorter OR time by 74 min |
| 40552443 | Pinto et al. 2026 (IJGO) | Uterine-sparing feasible in majority; 11.2% need hysterectomy; myometrial resection preferred technique |
| 37401769 | Lucidi et al. 2023 (UOG) | Urologic complications 15.2% overall; percreta: 38.5%; emergency surgery: 24.6% |
| 40472373 | Bonanni et al. 2025 (Obstet Gynecol) | Low-lying placenta: 2x PPH risk; PPH 16% even at 11-20 mm from os; PAS in 9% of low-lying placentas |
| 37565895 | Huang & Yang 2023 (Medicine) | Planned CS for PAS/abnormal placentation: better neonatal outcomes vs. emergency CS |
References:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, 8e - Chapters 27 (Abnormal Placentation - Imaging) and 43 (Placenta Previa, Placenta Accreta, Abruptio Placentae, Vasa Previa)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Chapter on Antepartum Hemorrhage
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Obstetric Anesthesia chapter
- Textbook of Family Medicine, 9e
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Miller's Anesthesia, 10e - Obstetric Anesthesia
This is a shared conversation. Sign in to Orris to start your own chat.