
Assessment the frontal view posture of this image
lateral sagittal postural assessment plumb line alignment head neck trunk pelvis
lateral posture assessment plumb line sagittal alignment
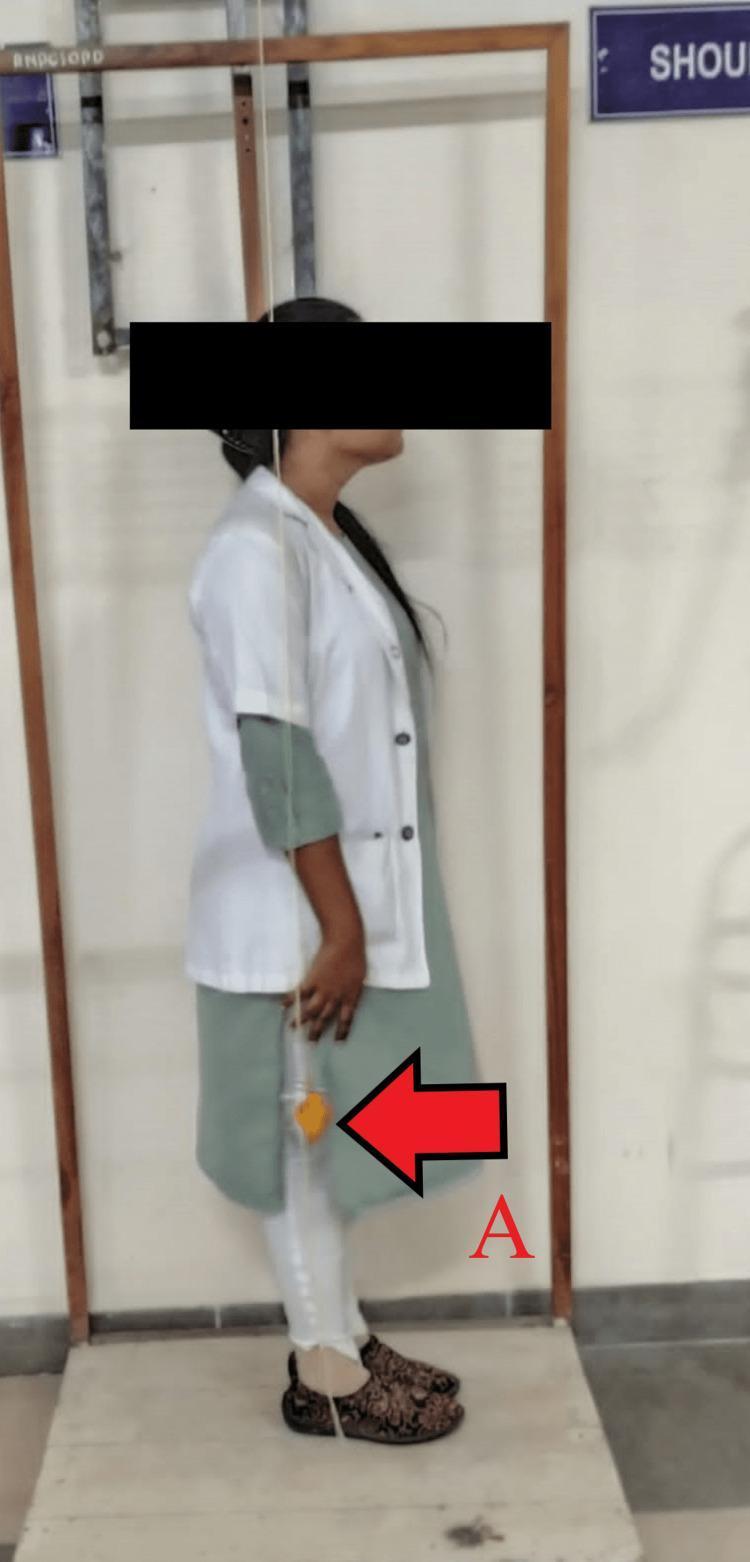
Note: The image provided is a lateral (sagittal) view, not a frontal (coronal) view. The assessment below is based on the lateral view that is actually visible.
Lateral (Sagittal Plane) Postural Assessment
Plumb Line Reference
- External auditory meatus (ear lobe)
- Tip of the shoulder (acromion)
- Greater trochanter of the hip
- Just anterior to the lateral malleolus of the ankle
Findings by Region
| Region | Observation | Deviation |
|---|---|---|
| Head/Cervical | Head is significantly forward of the plumb line; chin is tucked/flexed downward | Forward Head Posture (FHP) — marked |
| Cervical spine | Reduced or flattened cervical lordosis due to chin-down position | Cervical hypolordosis / forward flexion |
| Thoracic spine | Increased thoracic kyphosis — the upper back is visibly rounded and posterior to the plumb line | Hyperkyphosis (thoracic) |
| Lumbar spine | The trunk leans forward; lumbar lordosis appears reduced or obliterated | Possible lumbar hypolordosis |
| Pelvis | Appears to have a slight anterior tilt with the trunk leaning slightly forward | Mild anterior pelvic tilt |
| Hips & Knees | Knees appear in neutral to mild flexion; hip appears slightly flexed | No gross deformity visible |
| Feet | Bare feet, flat on floor; slight toe splaying noted | No obvious pes planus from this view |
Key Deviations Identified
Summary
- Marked forward head posture
- Thoracic hyperkyphosis
- Reduced lumbar lordosis
- Global anterior lean of the trunk

Put plumb line for the image and adjust the image properly and create me a image
-
PostureScreen Mobile or PostureCo apps — designed specifically for this purpose; auto-draw plumb lines on patient photos
-
PowerPoint / Google Slides — insert the image, then draw a vertical line from head to feet using the shapes tool
-
Paint / Preview (Mac) — open image, draw a straight vertical line using the line tool
- The vertical line should pass through:
- Midpoint of the skull
- Nose/chin midline
- Sternal notch
- Navel/umbilicus
- Pubic symphysis midpoint
- Midpoint between both feet
| Region | Finding |
|---|---|
| Head | Slight left lateral tilt |
| Shoulders | Right shoulder appears slightly lower |
| Trunk | Mild lean to the right |
| Pelvis | Mild right pelvic drop (Trendelenburg tendency) |
| Knees | Mild genu varum (bow-legged) bilaterally |
| Feet | Slight external rotation bilaterally |
Icf check list for right side stroke
ICF International Classification of Functioning checklist stroke body functions structures activity participation
right hemisphere stroke clinical features left hemiplegia neglect cognition communication
ICF Checklist — Right Side Stroke (Left Hemiplegia)
ICF Qualifier Scale: 0 = No problem (0–4%) | 1 = Mild (5–24%) | 2 = Moderate (25–49%) | 3 = Severe (50–95%) | 4 = Complete (96–100%) | 8 = Not specified | 9 = Not applicable
PART 1: BODY FUNCTIONS (b)
b1 — Mental Functions
| ICF Code | Domain | Qualifier (0–4) | Notes |
|---|---|---|---|
| b110 | Consciousness functions | Alertness, orientation | |
| b114 | Orientation functions | Time, place, person | |
| b117 | Intellectual functions | Cognitive processing | |
| b122 | Global psychosocial functions | ||
| b126 | Temperament & personality | Impulsivity, emotional lability | |
| b130 | Energy & drive functions | Motivation, fatigue | |
| b134 | Sleep functions | ||
| b140 | Attention functions | Hemispatial neglect — hallmark of right hemisphere stroke (Harrison's, p. 873) | |
| b144 | Memory functions | Short-term memory | |
| b147 | Psychomotor functions | ||
| b152 | Emotional functions | Depression, emotional dysregulation | |
| b156 | Perceptual functions | Left-sided neglect, anosognosia | |
| b160 | Thought functions | ||
| b164 | Higher-level cognitive functions | Problem solving, judgment | |
| b167 | Mental functions of language | Prosody deficits (right hemisphere) | |
| b172 | Calculation functions |
b2 — Sensory Functions & Pain
| ICF Code | Domain | Qualifier (0–4) | Notes |
|---|---|---|---|
| b210 | Seeing functions | Left homonymous hemianopia | |
| b215 | Functions of structures adjoining the eye | ||
| b230 | Hearing functions | ||
| b235 | Vestibular functions | Balance, dizziness | |
| b260 | Proprioceptive function | Left side proprioception loss | |
| b265 | Touch function | Left-sided sensory loss | |
| b270 | Sensory functions related to temperature & pain | ||
| b280 | Sensation of pain | Central post-stroke pain |
b3 — Voice & Speech Functions
| ICF Code | Domain | Qualifier (0–4) | Notes |
|---|---|---|---|
| b310 | Voice functions | Dysarthria possible | |
| b320 | Articulation functions | ||
| b330 | Fluency & rhythm of speech | Dysprosody (flat/monotone speech) |
b4 — Functions of the Cardiovascular, Haematological, Immunological & Respiratory Systems
| ICF Code | Domain | Qualifier (0–4) | Notes |
|---|---|---|---|
| b410 | Heart functions | Atrial fibrillation (common etiology) | |
| b420 | Blood pressure functions | Hypertension | |
| b440 | Respiration functions | Reduced respiratory effort | |
| b445 | Respiratory muscle functions |
b5 — Functions of the Digestive, Metabolic & Endocrine Systems
| ICF Code | Domain | Qualifier (0–4) | Notes |
|---|---|---|---|
| b510 | Ingestion functions | Dysphagia | |
| b525 | Defecation functions | Bowel incontinence | |
| b530 | Weight maintenance functions | Nutritional status | |
| b620 | Urination functions | Urinary incontinence/retention |
b7 — Neuromusculoskeletal & Movement-Related Functions
| ICF Code | Domain | Qualifier (0–4) | Notes |
|---|---|---|---|
| b710 | Mobility of joint functions | Left UL & LL | |
| b715 | Stability of joint functions | Shoulder subluxation (left) | |
| b720 | Mobility of bone functions | ||
| b730 | Muscle power functions | Left hemiplegia/hemiparesis | |
| b735 | Muscle tone functions | Spasticity — left side | |
| b740 | Muscle endurance functions | ||
| b750 | Motor reflex functions | Hyperreflexia left side | |
| b755 | Involuntary movement reaction functions | ||
| b760 | Control of voluntary movement | Dyscoordination | |
| b765 | Involuntary movement functions | ||
| b770 | Gait pattern functions | Hemiplegic gait | |
| b780 | Sensations related to muscles & movement |
PART 2: BODY STRUCTURES (s)
| ICF Code | Structure | Qualifier | Nature of Impairment |
|---|---|---|---|
| s110 | Structure of brain | Right hemisphere lesion | |
| s120 | Spinal cord & related structures | ||
| s130 | Structure of meninges | ||
| s710 | Structure of head & neck region | ||
| s720 | Structure of shoulder region | Left shoulder subluxation | |
| s730 | Structure of upper extremity | Left UE | |
| s750 | Structure of lower extremity | Left LE | |
| s760 | Structure of trunk | Trunk control impairment | |
| s810 | Skin & related structures | Pressure ulcer risk |
PART 3: ACTIVITIES & PARTICIPATION (d)
d1 — Learning & Applying Knowledge
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d110 | Watching | Left neglect affects | ||
| d115 | Listening | |||
| d160 | Focusing attention | Attention deficits | ||
| d175 | Solving problems | Executive dysfunction |
d2 — General Tasks & Demands
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d210 | Undertaking single task | |||
| d220 | Undertaking multiple tasks | |||
| d230 | Carrying out daily routine | |||
| d240 | Handling stress & demands |
d3 — Communication
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d310 | Communicating — receiving spoken messages | |||
| d315 | Communicating — receiving non-verbal messages | |||
| d330 | Speaking | Dysarthria, dysprosody | ||
| d335 | Producing non-verbal messages | |||
| d350 | Conversation |
d4 — Mobility
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d410 | Changing basic body position | Bed mobility | ||
| d415 | Maintaining body position | Sitting/standing balance | ||
| d420 | Transferring oneself | |||
| d430 | Lifting & carrying objects | Left UE deficit | ||
| d440 | Fine hand use | Left hand | ||
| d445 | Hand & arm use | |||
| d450 | Walking | Hemiplegic gait | ||
| d455 | Moving around | |||
| d460 | Moving around in different locations | |||
| d465 | Moving around using equipment | Wheelchair, walking aid | ||
| d470 | Using transportation |
d5 — Self-Care
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d510 | Washing oneself | |||
| d520 | Caring for body parts | Left neglect | ||
| d530 | Toileting | |||
| d540 | Dressing | Left side dressing apraxia | ||
| d550 | Eating | Dysphagia | ||
| d560 | Drinking | |||
| d570 | Looking after one's health | Medication compliance |
d6 — Domestic Life
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d620 | Acquisition of goods & services | |||
| d630 | Preparing meals | |||
| d640 | Doing housework | |||
| d660 | Assisting others |
d7 — Interpersonal Interactions & Relationships
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d710 | Basic interpersonal interactions | |||
| d720 | Complex interpersonal interactions | |||
| d730 | Relating with strangers | |||
| d740 | Formal relationships | |||
| d750 | Informal social relationships | |||
| d760 | Family relationships | |||
| d770 | Intimate relationships |
d8 — Major Life Areas
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d820 | School education | |||
| d850 | Remunerative employment | |||
| d870 | Economic self-sufficiency |
d9 — Community, Social & Civic Life
| ICF Code | Domain | Capacity | Performance | Notes |
|---|---|---|---|---|
| d910 | Community life | |||
| d920 | Recreation & leisure | |||
| d930 | Religion & spirituality | |||
| d940 | Human rights | |||
| d950 | Political life & citizenship |
PART 4: CONTEXTUAL FACTORS
Environmental Factors (e) — Barriers (−) / Facilitators (+)
| ICF Code | Factor | Rating | Notes |
|---|---|---|---|
| e110 | Products for personal consumption | Medications, nutrition | |
| e115 | Products for personal use in daily living | Assistive devices | |
| e120 | Products for indoor/outdoor mobility | Wheelchair, AFO | |
| e150 | Design of public buildings | Accessibility | |
| e155 | Design of private buildings | Home modifications | |
| e310 | Immediate family | Caregiver support | |
| e320 | Friends | Social support | |
| e325 | Acquaintances, peers | ||
| e330 | People in positions of authority | ||
| e340 | Personal care providers | Physiotherapist, OT, SLP | |
| e355 | Health professionals | Multidisciplinary team | |
| e410 | Individual attitudes of family members | ||
| e450 | Individual attitudes of health professionals | ||
| e465 | Social norms, practices & ideologies | ||
| e570 | Social security services | Disability benefits | |
| e580 | Health services | Rehab access |
Personal Factors (non-coded in ICF)
| Factor | Details |
|---|---|
| Age | Older age — poorer prognosis |
| Sex | Male/Female |
| Premorbid functional level | Independent vs. dependent |
| Comorbidities | DM, HTN, CAD, AF |
| Education level | Affects cognitive rehab |
| Motivation | Key for rehab adherence |
| Coping style | Psychological resilience |
| Social support | Family involvement |
Key Right Hemisphere Stroke-Specific Highlights
| Feature | ICF Domain | Code |
|---|---|---|
| Left hemispatial neglect | Body Functions | b156, b140 |
| Anosognosia (unawareness of deficits) | Body Functions | b164 |
| Impulsivity / poor safety judgment | Body Functions | b126, b164 |
| Left hemiplegia/hemiparesis | Body Functions | b730 |
| Left shoulder subluxation | Body Structures | s720 |
| Dysprosody (flat, monotone speech) | Body Functions | b330 |
| Visuospatial deficits | Body Functions | b156 |
| Dressing apraxia | Activities | d540 |
| Hemiplegic gait | Activities | d450, b770 |
Clinical Note: Right hemisphere strokes are often underestimated in severity because language (aphasia) is absent. However, neglect, anosognosia, and impaired safety awareness make rehabilitation significantly more challenging. Caregiver education and environmental modification (e310, e155) are critical facilitators.
Give problem list short term and long term goals and advanced treatment of physiotherapy treatment of 60 year old man with mca stroke with upper limb spasticity and lower limb only weekness
MCA stroke upper limb spasticity lower limb weakness physiotherapy treatment rehabilitation
stroke spasticity management physiotherapy goals short term long term hemiplegia
stroke rehabilitation advanced physiotherapy techniques constraint induced movement therapy task specific training neuroplasticity
MCA stroke problem list functional deficits balance gait training lower limb strengthening
Physiotherapy Management
60-Year-Old Male | MCA Stroke | UL Spasticity + LL Weakness
PATIENT PROFILE
| Parameter | Detail |
|---|---|
| Age | 60 years, Male |
| Diagnosis | MCA territory stroke (ischemic/hemorrhagic) |
| Upper Limb | Spasticity (flexor pattern — shoulder adduction, elbow flexion, wrist/finger flexion) |
| Lower Limb | Weakness only (no significant spasticity) |
| Stage | Subacute to chronic |
PROBLEM LIST
Impairment Level
| # | Problem | Clinical Presentation |
|---|---|---|
| 1 | UL Spasticity | Flexor synergy pattern — shoulder adductor/IR, elbow flexor, wrist/finger flexor spasticity; MAS Grade 2–3 |
| 2 | LL Weakness | Hip abductor, knee extensor, dorsiflexor weakness; MRC Grade 2–3 |
| 3 | Shoulder subluxation | Inferior subluxation due to rotator cuff/deltoid weakness |
| 4 | Impaired trunk control | Reduced lateral and anterior trunk stability |
| 5 | Balance impairment | Reduced static and dynamic standing balance; Berg Balance Scale deficit |
| 6 | Gait dysfunction | Hemiplegic gait — circumduction, reduced heel strike, foot drop tendency |
| 7 | Sensory deficits | Reduced proprioception and superficial sensation left/right side |
| 8 | Pain | Shoulder-hand syndrome / central post-stroke pain |
| 9 | Reduced endurance | Cardiovascular deconditioning, fatigue |
| 10 | Postural malalignment | Asymmetric weight bearing, lateral trunk lean |
Activity Limitation Level
| # | Problem |
|---|---|
| 11 | Impaired bed mobility and transfers |
| 12 | Difficulty with ADLs — dressing, grooming (UL spasticity) |
| 13 | Impaired ambulation — requires assistive device |
| 14 | Inability to climb stairs |
| 15 | Reduced fine motor and hand function |
Participation Restriction Level
| # | Problem |
|---|---|
| 16 | Unable to return to occupational/social roles |
| 17 | Dependence on caregiver |
| 18 | Restricted community mobility |
| 19 | Psychosocial — depression, reduced self-efficacy |
SHORT-TERM GOALS
| # | Goal | Measure |
|---|---|---|
| STG 1 | Reduce UL spasticity by 1 grade | MAS reduction from Grade 2–3 → 1–2 |
| STG 2 | Improve LL muscle strength by 1 MRC grade | Hip abductors, knee extensors, dorsiflexors |
| STG 3 | Achieve independent sitting balance | Static sitting balance — unsupported 30 sec |
| STG 4 | Achieve safe sit-to-stand transfer with minimal assist | FIM score improvement |
| STG 5 | Prevent shoulder subluxation complications | Maintain pain-free shoulder range |
| STG 6 | Reduce spasticity-related pain | VAS 3/10 from baseline |
| STG 7 | Maintain full passive ROM all joints | Prevent contractures |
| STG 8 | Initiate standing balance training | Stand with support 1–2 min |
| STG 9 | Improve trunk control in sitting | Lateral weight shift — active |
| STG 10 | Patient/caregiver education on positioning | Correct lying/sitting posture 100% compliance |
LONG-TERM GOALS
| # | Goal | Measure |
|---|---|---|
| LTG 1 | Independent ambulation with or without assistive device | FAC Level 4–5; 10MWT improvement |
| LTG 2 | Functional use of affected UL in bimanual ADLs | ARAT score improvement ≥10 points |
| LTG 3 | Normalize gait pattern — reduce circumduction & foot drop | Gait analysis parameters |
| LTG 4 | Independent stair climbing | 1 flight with rail |
| LTG 5 | Manage UL spasticity long-term | MAS Grade ≤1 with combined therapy |
| LTG 6 | Independent self-care ADLs | FIM score ≥ 90 |
| LTG 7 | Return to community ambulation | 6MWT ≥ 300 m |
| LTG 8 | Prevent secondary complications | Zero pressure ulcers, no falls, no frozen shoulder |
| LTG 9 | Improve quality of life | Stroke Impact Scale improvement |
| LTG 10 | Caregiver independence in home exercise program | HEP adherence ≥80% |
ADVANCED PHYSIOTHERAPY TREATMENT PLAN
PHASE 1 — ACUTE/EARLY SUBACUTE (Week 1–2)
A. Positioning & Handling
- Antispasticity positioning: UL in shoulder abduction, elbow extension, wrist/finger extension using splints
- Avoid traction on subluxed shoulder
- Proper hemiplegic positioning in bed (avoid shoulder internal rotation, hip external rotation)
- Use of Bobath handling techniques for tone normalization
B. Passive & Active-Assisted ROM
- Gentle passive ROM all joints 2× daily
- Shoulder: scapular mobilization before glenohumeral movement
- Wrist/finger extension stretching for spastic flexors
- Neural mobilization — median nerve (for UL spasticity)
C. Respiratory Physiotherapy
- Diaphragmatic breathing, trunk expansion exercises
- Positioning for optimal ventilation
PHASE 2 — SPASTICITY MANAGEMENT (Ongoing)
1. Stretching & Inhibitory Techniques
- Prolonged static stretching of spastic muscles (≥20 min sustained stretch)
- Reflex Inhibiting Patterns (RIPs) — Bobath NDT approach
- Rhythmic Rotation — slow, rhythmic passive movement to reduce tone
- Weight bearing through affected UL — inhibits flexor spasticity (neurodevelopmental technique)
2. Neuromuscular Facilitation
- Proprioceptive Neuromuscular Facilitation (PNF)
- D1 extension pattern (UL): shoulder flexion/abduction/ER + elbow extension
- D2 flexion/extension patterns for LL strengthening
- Hold-Relax and Contract-Relax techniques for spastic muscles
3. Splinting & Orthotic Management
- Resting hand splint (night) — maintain wrist/finger in extension
- Lycra arm sleeve — proprioceptive input, tone normalization
- AFO (Ankle Foot Orthosis) — for foot drop and safe ambulation during LL weakness phase
4. Extracorporeal Shock Wave Therapy (ESWT)
- Radial ESWT over spastic UL muscles (biceps, wrist flexors)
- Protocol: 1500–2000 shocks, 0.1 mJ/mm², 3–5 sessions weekly
- Evidence: Significant MAS reduction at short, mid, and long-term follow-up (Management of Stroke Rehabilitation, p. 73)
5. Botulinum Toxin (Adjunct — coordinated with physician)
- Injection into: biceps brachii, brachialis, flexor carpi radialis/ulnaris, finger flexors
- Post-injection physiotherapy within 2 weeks mandatory
- Effect lasts 12–16 weeks; combine with intensive PT (Management of Stroke Rehabilitation, p. 68)
6. Functional Electrical Stimulation (FES)
- FES to wrist/finger extensors — reduces flexor spasticity, facilitates active extension
- Cyclic FES during task practice for neuroplastic effect
- NMES to shoulder stabilizers for subluxation prevention
PHASE 3 — LOWER LIMB STRENGTHENING & GAIT TRAINING
A. Strengthening Program (Progressive Resistance)
| Muscle Group | Exercise | Sets/Reps |
|---|---|---|
| Hip abductors | Side-lying abduction, TheraBand | 3×15 |
| Hip extensors | Bridging, prone hip extension | 3×15 |
| Knee extensors | Seated knee extension, mini-squats | 3×15 |
| Dorsiflexors | Ankle DF against resistance, theraband | 3×20 |
| Calf/plantarflexors | Heel raises | 3×20 |
| Trunk stabilizers | Core activation — drawing-in, dead bug | Daily |
B. Balance Training (Progressive)
- Level 1: Supported standing — parallel bars
- Level 2: Standing weight shift — lateral, anterior-posterior
- Level 3: Single leg stance (unaffected side support)
- Level 4: Tandem standing, perturbation training
- Level 5: Dynamic balance — stepping, reaching tasks
- Balance Board / Wobble Board — proprioceptive training
- Virtual Reality Balance Training — evidence-based; interactive, motivating
C. Gait Rehabilitation
- Parallel bars → walking frame → tripod/quad stick → independent
- Pre-gait activities: weight shifting, step-up, stepping over obstacles
| Technique | Description | Benefit |
|---|---|---|
| Treadmill Training (BWS-TT) | Body weight supported treadmill — 20–40% unloading | High repetition, safe gait practice |
| Lokomat / Robotic Gait Trainer | Exoskeleton-assisted treadmill | Precise joint kinematics, high intensity |
| Overground with visual/auditory cues | Metronome-paced walking, floor targets | Rhythmic auditory stimulation (RAS) improves cadence |
| Obstacle course training | Community-simulated environment | Transfers to real-world ambulation |
| Aquatic therapy / Hydrotherapy | Buoyancy reduces LL load; resistance builds strength | Safe early strengthening |
PHASE 4 — ADVANCED UPPER LIMB REHABILITATION
1. Constraint-Induced Movement Therapy (CIMT)
- Restrain unaffected UL with mitt/sling for 90% waking hours
- Intensive shaping tasks with affected UL — 6 hours/day × 2 weeks
- Modified CIMT (mCIMT): 3–5 hours/day for patients with moderate function
- Best evidence for UL recovery in stroke — drives neuroplastic cortical reorganization
2. Mirror Therapy
- Affected UL placed behind mirror; patient views reflection of unaffected limb moving
- 30 min sessions, 5 days/week × 4 weeks
- Activates motor cortex via visual feedback; effective in spasticity + weakness
3. Mental Practice / Motor Imagery
- Patient mentally rehearses UL movements
- Combine with physical practice — additive neuroplastic effect
- Protocol: 20 min imagery × 5 sessions/week
4. Task-Specific Training
- Repetitive, goal-directed functional tasks:
- Reaching for objects at various heights
- Opening jars, turning door handles
- Typing, folding clothes
- Pouring water — graded task difficulty
5. Robotic-Assisted UL Therapy
- Armeo Spring / MIT-MANUS — gravity-compensated UL robotic training
- High-repetition, low-effort reaching in gamified environments
- Indicated when active movement is minimal
6. Electromyographic (EMG) Biofeedback
- Surface EMG on target muscles (wrist extensors, biceps antagonists)
- Real-time visual/auditory feedback of muscle activity
- Improves voluntary motor control, reduces co-contraction
7. Transcranial Magnetic Stimulation (TMS) — Adjunct
- Inhibitory rTMS to contralesional (unaffected) hemisphere — reduces interhemispheric inhibition
- Excitatory TMS to ipsilesional hemisphere — facilitates motor cortex
- Combine with physiotherapy immediately after session
PHASE 5 — FUNCTIONAL & COMMUNITY REHABILITATION
| Area | Intervention |
|---|---|
| Stair training | Step-up/down training, rail use, negotiating curbs |
| Fall prevention | Hip strengthening, balance retraining, home hazard assessment |
| Energy conservation | Activity pacing, rest-work cycles |
| Community mobility | Outdoor walking program, transport skills |
| Home program | Structured HEP: stretching, strengthening, balance — 45 min/day |
| Caregiver training | Transfer assistance, positioning, spotting during gait |
OUTCOME MEASURES
| Domain | Measure |
|---|---|
| Spasticity | Modified Ashworth Scale (MAS) |
| UL Function | Action Research Arm Test (ARAT), Fugl-Meyer UL |
| LL Strength | MRC grading, Hand-held dynamometry |
| Balance | Berg Balance Scale (BBS), TUG |
| Gait | 10-Metre Walk Test (10MWT), 6MWT, FAC |
| Functional Independence | FIM, Barthel Index |
| Quality of Life | Stroke Impact Scale (SIS) |
| Pain | VAS, CPSP screening |
SUMMARY TREATMENT ALGORITHM
Acute Phase
↓
Positioning + Passive ROM + Respiratory PT
↓
Spasticity Management (Stretching + FES + ESWT + Splinting ± Botox)
↓
Trunk Control + Sitting Balance
↓
LL Strengthening (PNF + Progressive Resistance)
↓
Standing Balance + Pre-gait Activities
↓
Gait Training (BWS-TT → Overground → Community)
↓
Advanced UL (CIMT + Mirror Therapy + Robotics + Task-Specific)
↓
Community Reintegration + HEP + Caregiver Education
Clinical Note: The distinct pattern of UL spasticity with LL weakness only (without LL spasticity) suggests the corticospinal tract lesion may be incomplete or that lower motor neuron pathways to the LL are relatively preserved. This is a favorable prognostic sign for LL functional recovery. Priority should be aggressive spasticity management in UL combined with high-intensity strengthening and gait retraining for the LL. (Management of Stroke Rehabilitation, pp. 68, 73)
First give short term treatment plan for old cva case
chronic old CVA stroke short term physiotherapy treatment plan rehabilitation goals
Short-Term Physiotherapy Treatment Plan
Old (Chronic) CVA Case — Week 1 to Week 4
Key Considerations for Chronic CVA
In an old/chronic CVA (>6 months post-stroke), neuroplasticity is still present but slower. The focus shifts from spontaneous recovery to skill relearning, compensatory strategies, spasticity/contracture management, and preventing secondary complications. Intensity of practice remains the strongest driver of improvement.
WEEK 1 — ASSESSMENT & BASELINE ESTABLISHMENT
Day 1–3: Comprehensive Evaluation
| Assessment Area | Tool Used |
|---|---|
| Spasticity | Modified Ashworth Scale (MAS) |
| Muscle strength | MRC grading |
| ROM | Goniometry — all joints |
| Balance | Berg Balance Scale (BBS) |
| Gait | FAC, 10MWT, TUG |
| Sensation | Light touch, proprioception, pain |
| Functional independence | Barthel Index / FIM |
| Pain | VAS |
| Posture | Static postural assessment |
| Tone & reflexes | Clinical neurological exam |
Day 1–7: Initial Treatment Priorities
1. Pain & Spasticity Control (UL)
- Prolonged passive stretching of spastic muscles — 20–30 min
- Elbow extensors stretch, wrist/finger extension stretch
- Hold each stretch 60 seconds × 3 sets
- Reflex Inhibiting Patterns (RIP) — Bobath technique
- Key pattern: Shoulder ER + abduction + elbow extension + wrist extension
- Ice/cold pack over spastic UL muscles — 10–15 min before stretching
- Resting hand splint application — nights + 2 hrs daytime
- Proper antispasticity positioning in sitting and lying
2. Passive & Active-Assisted ROM
- All joints — upper and lower limb
- Shoulder: scapular mobilization first, then glenohumeral
- Hip, knee, ankle — full range daily
- Prevents contracture (primary risk in chronic CVA)
3. Trunk Activation
- Supported sitting — active trunk holding 30 sec × 5 reps
- Lateral weight shift in sitting — active
- Anterior-posterior weight shift with therapist support
- Deep breathing + trunk expansion exercises
4. Positioning Education
- Caregiver training on:
- Correct hemiplegic lying positions (supine, side-lying)
- Seated posture with arm support
- Avoid prolonged elbow/wrist flexion postures
WEEK 2 — FUNCTIONAL ACTIVATION & STRENGTHENING
1. Continued Spasticity Management
- Progress stretching — increase duration to 30–45 min
- Neurodevelopmental Technique (NDT):
- Weight bearing through affected UL (elbow extended, palm flat on plinth)
- Inhibits flexor spasticity reflexively
- Slow, rhythmic rotation of limb segments — tone reduction
- FES/NMES to wrist and finger extensors (antagonists of spastic muscles)
- 20 min sessions, 5 days/week
2. Lower Limb Strengthening (Progressive)
| Exercise | Position | Sets × Reps |
|---|---|---|
| Bridging | Supine | 3 × 15 |
| Hip abduction | Side-lying | 3 × 15 |
| Straight leg raise | Supine | 3 × 15 |
| Knee extension | Sitting | 3 × 15 |
| Ankle dorsiflexion | Sitting, TheraBand | 3 × 20 |
| Heel-toe raises | Standing with support | 3 × 20 |
3. Sitting Balance — Progressive
- Static: Unsupported sitting 1–3 min
- Dynamic: Reaching tasks in sitting — forward, lateral, diagonal
- Perturbation in sitting — gentle manual destabilization → reactive balance
- Ball rolling on plinth — weight shift facilitation
4. Sitting to Standing Practice
- Assisted sit-to-stand with verbal cues
- Focus: equal weight bearing through both lower limbs
- Mirror feedback for symmetry correction
- Repeat 10–15 times per session
WEEK 3 — STANDING BALANCE & PRE-GAIT TRAINING
1. Standing Balance Program
| Level | Activity | Target |
|---|---|---|
| Level 1 | Standing in parallel bars — static hold | 2–3 min |
| Level 2 | Lateral weight shift in standing | 3 × 10 reps |
| Level 3 | Forward reach in standing | Without losing balance |
| Level 4 | Stepping in place | 3 × 10 steps |
| Level 5 | Tandem standing | 30 sec |
2. Pre-Gait Activities
- Pelvic tilting in standing — anterior/posterior
- Hip hiking exercises — prepares for swing phase
- Stepping over lines/obstacles on floor
- Marching in place with parallel bar support
- Weight shifting to affected LL — crucial for stance phase preparation
- Ankle rocking — heel to toe weight transfer
3. UL Functional Activation
- Mirror therapy — 20–30 min daily
- Mirror placed sagittally; patient watches unaffected hand move
- Facilitates motor cortex activation of affected side
- Bilateral arm training — symmetric reaching tasks
- Unaffected side guides affected side
- Gravity-eliminated UL exercises:
- Shoulder flexion/abduction in side-lying
- Elbow flexion/extension in supported position
- Wrist extension facilitation — tapping, brushing, quick stretch
4. Sensory Re-education
- Tactile stimulation — different textures on affected limb
- Proprioceptive training — joint repositioning tasks
- Weight bearing on affected UL for deep pressure input
- Vibration therapy over affected muscles
WEEK 4 — GAIT INITIATION & ADL TRAINING
1. Gait Training
- Parallel bars → Walking frame → Quad stick
- Therapist: manual guidance at pelvis and affected knee
- Gait cues:
- "Lift the knee"
- "Push off with the toes"
- "Heel first"
- Rhythmic auditory stimulation (RAS) — metronome at comfortable cadence
- AFO fitting if foot drop present — for safe ambulation
- Walk 10–15 metres × 3–5 repetitions per session
2. Stair Training (if appropriate)
- Step-up/step-down on single step
- Rail support — unaffected side
- Principle: "Good goes up, bad goes down"
3. ADL Integration
| ADL Task | Training Focus |
|---|---|
| Dressing | UL involvement in pulling/pushing clothes |
| Grooming | Bimanual task — affected UL as assist hand |
| Eating | Stabilize plate with affected hand |
| Writing/reaching | Task-specific reaching practice |
| Transfers | Bed ↔ chair, chair ↔ toilet |
4. Home Exercise Program (HEP) Initiation
- Teach patient + caregiver:
- Daily stretching routine (UL spastic muscles)
- LL strengthening exercises
- Balance practice — safe standing at kitchen counter
- Walking practice indoors
- Written illustrated HEP provided
SHORT-TERM TREATMENT SUMMARY TABLE
| Week | Priority Focus | Key Techniques |
|---|---|---|
| Week 1 | Assessment + Pain/Spasticity control + ROM + Positioning | Stretching, RIP, Splinting, Caregiver education |
| Week 2 | Spasticity inhibition + LL strengthening + Sitting balance | NDT weight bearing, FES, Progressive strengthening, Sit-to-stand |
| Week 3 | Standing balance + Pre-gait + UL activation | Balance progression, Mirror therapy, Bilateral training, Sensory re-education |
| Week 4 | Gait initiation + ADL training + HEP | Parallel bars walking, RAS, AFO, Task-specific ADL training |
SHORT-TERM GOALS ACHIEVED BY WEEK 4
| Goal | Expected Outcome |
|---|---|
| Spasticity | MAS reduced by 1 grade |
| ROM | Full passive ROM maintained — no new contractures |
| LL Strength | MRC improved by 1 grade in key muscle groups |
| Sitting balance | Independent unsupported sitting ≥ 3 min |
| Transfers | Modified independent sit-to-stand |
| Standing | Supported standing ≥ 5 min |
| Gait | Initiation of walking with assistive device in parallel bars |
| ADL | Improved participation in 2–3 self-care tasks |
| Pain | VAS reduced by 2 points |
| HEP | Patient/caregiver independently performing home program |
Clinical Note: In chronic CVA, intensity and repetition are the most critical factors for neuroplastic recovery — even years post-stroke. A minimum of 45 minutes of active task practice per session is recommended. Passive modalities alone are insufficient; every session should include active patient participation wherever possible. (Management of Stroke Rehabilitation, p. 55)
Long term goals
chronic stroke long term rehabilitation gait retraining neuroplasticity community ambulation functional recovery
stroke long term upper limb rehabilitation CIMT mirror therapy robot assisted task specific training
Long-Term Physiotherapy Treatment Plan
Old (Chronic) CVA Case — Month 2 to Month 6
KEY PRINCIPLE
Intensity of training is the most critical determinant of sustained long-term improvement in chronic stroke. Activity-dependent neuroplasticity drives cortical motor map reorganization and functional recovery even in old CVA cases. Technology-assisted high-repetition training maximizes this potential. (Harrison's, p. 13833)
LONG-TERM GOALS (Month 2–6)
| # | Goal | Target Outcome Measure |
|---|---|---|
| LTG 1 | Independent community ambulation | FAC Level 5; 6MWT ≥ 300 m |
| LTG 2 | Normalize gait pattern | Reduced circumduction, heel strike restored — Gait analysis |
| LTG 3 | Functional UL use in bimanual ADLs | ARAT ≥ 10 point improvement |
| LTG 4 | Sustained spasticity reduction | MAS ≤ Grade 1 |
| LTG 5 | Independent stair climbing | 1 flight with rail — FAC stair level |
| LTG 6 | Full independence in self-care ADLs | Barthel Index ≥ 85 / FIM ≥ 90 |
| LTG 7 | Prevent secondary complications | Zero falls, zero contractures, zero pressure ulcers |
| LTG 8 | Return to social/community roles | Stroke Impact Scale improvement |
| LTG 9 | Independent home exercise program | HEP adherence ≥ 80% — caregiver report |
| LTG 10 | Improved cardiovascular endurance | 6MWT improvement ≥ 54 m (MCID) |
MONTH 2 — ADVANCED SPASTICITY MANAGEMENT & GAIT CONSOLIDATION
1. Advanced Spasticity Management
Extracorporeal Shock Wave Therapy (ESWT)
- Radial ESWT over biceps, brachialis, wrist/finger flexors
- Protocol: 1500–2000 shocks, 0.1 mJ/mm², 3 sessions/week × 4 weeks
- Significant MAS reduction at short, mid, and long-term follow-up (Management of Stroke Rehabilitation, p. 73)
Botulinum Toxin (Coordinated with Physician)
- Injection sites: biceps brachii, brachialis, flexor carpi radialis, flexor carpi ulnaris, finger flexors
- Mandatory: intensive physiotherapy within 2 weeks post-injection
- Effect window: 12–16 weeks — maximize therapy during this period
- Repeat cycle every 3–4 months as needed (Management of Stroke Rehabilitation, p. 68)
Serial Casting
- Progressive plaster casting of elbow/wrist in increasing extension
- Changed every 5–7 days — gradual lengthening of spastic muscles
- Best for fixed or near-fixed contractures developing from chronic spasticity
Sustained Mechanical Stretch
- Dynasplint or Ultraflex splint — prolonged low-load stretch overnight
- 6–8 hours wear — biomechanical remodeling of soft tissue
2. Gait Consolidation Program
| Stage | Activity | Target |
|---|---|---|
| Overground walking | Walking frame → Quad stick → Single point stick | 20–30 m independently |
| Speed training | Fast/slow walking alternation | Improve cadence and step length |
| Dual-task walking | Walk + carry object / walk + counting | Cognitive-motor integration |
| Direction changes | Figure-of-8 walking, turning | Safety in real environments |
| Uneven surfaces | Grass, gravel, slope simulation | Community readiness |
| RAS (Rhythmic Auditory Stimulation) | Metronome-paced walking | Improve gait cadence and symmetry |
MONTH 3 — ADVANCED UL REHABILITATION & BALANCE MASTERY
1. Constraint-Induced Movement Therapy (CIMT)
- At least 10° active wrist extension
- At least 10° active finger extension in 2 fingers
| Component | Detail |
|---|---|
| Restraint | Mitt/sling on unaffected UL — 90% waking hours |
| Practice | Task-specific shaping of affected UL — 3–6 hrs/day |
| Duration | 2 weeks intensive OR mCIMT — 3 hrs/day × 4–6 weeks |
| Transfer package | ADL skill transfer to home environment |
- Picking up objects of varying size/weight
- Stacking blocks, turning pages
- Opening jars, door handles, taps
- Feeding, grooming, dressing activities
CIMT is appropriate only for those with some active movement in the paretic limb. mCIMT (≤3 hours/day) is suitable for patients who cannot tolerate full CIMT intensity. (Management of Stroke Rehabilitation, p. 47)
2. Mirror Therapy
- Mirror placed sagittally on midline
- Affected UL behind mirror; patient views reflection of unaffected UL
- Protocol: 30 min × 5 days/week × 4 weeks
- Tasks: wrist flexion/extension, finger movements, grasp/release
- Activates mirror neuron system — facilitates ipsilesional motor cortex
3. Mental Practice / Motor Imagery
- 20 min imagery sessions × 5 days/week
- Patient mentally rehearses specific UL tasks (reaching, grasping)
- Combine with physical practice immediately after — additive neuroplastic effect
- Use audio-guided imagery scripts for compliance
4. Advanced Balance Training
| Level | Exercise | Progression |
|---|---|---|
| Static | Single leg stance (affected limb) | Eyes open → eyes closed |
| Dynamic | Step and reach, star excursion balance | Increase reach distance |
| Perturbation | Manual push/pull in standing | Unpredictable directions |
| Dual task | Standing + cognitive task (counting, naming) | Increases difficulty |
| Functional | Obstacle negotiation, stepping over objects | Real-world simulation |
| Technology | Balance board, Wii-Fit balance games | Biofeedback, engaging |
MONTH 4 — TECHNOLOGY-ASSISTED REHABILITATION
1. Robotic-Assisted Upper Limb Training
| Device | Function | Indication |
|---|---|---|
| Armeo Spring | Gravity-compensated arm support + gamified reaching | Minimal active UL movement |
| MIT-MANUS | Shoulder-elbow robot — planar reaching | Moderate UL weakness + spasticity |
| Hand of Hope | EMG-triggered finger extension robot | Finger flexor spasticity |
- Sessions: 45–60 min × 5 days/week
- High repetition (500–1000 movements/session) — drives neuroplasticity
2. Body Weight Supported Treadmill Training (BWSTT)
- 20–40% body weight support via overhead harness
- Treadmill speed: start slow (0.2–0.5 km/h) → progress to comfortable speed
- Therapist manually facilitates hip/knee during swing if needed
- Benefit: safe high-repetition stepping — activates spinal locomotor CPGs
- Progress: reduce body weight support by 5–10% every 2 weeks
3. Lokomat / Robotic Gait Trainer
- Exoskeleton-guided treadmill walking
- Precise joint kinematics — hip and knee guidance
- High-intensity, high-repetition gait practice
- Indicated when: unable to walk on treadmill independently or fear of falling
4. Virtual Reality (VR) Rehabilitation
- UL: VR reaching, grasping, manipulation tasks
- Balance/Gait: VR obstacle avoidance, community navigation simulation
- Immersive environment — high motivation, reduces perceived effort
- Wearable sensor-based systems (e.g., Leap Motion, Nintendo Switch) for home VR
5. Neuromuscular Electrical Stimulation (NMES) / FES
| Application | Target | Protocol |
|---|---|---|
| FES cycling | LL muscles during cycling | 30 min × 5/week |
| FES-assisted walking | Peroneal FES for foot drop | During every gait session |
| NMES wrist extensors | Antagonist to spastic flexors | 20 min × daily |
| EMG-triggered NMES | Patient initiates, device amplifies | Voluntary + electrical |
MONTH 5 — COMMUNITY REINTEGRATION & FUNCTIONAL INDEPENDENCE
1. Community Ambulation Training
| Activity | Goal |
|---|---|
| Outdoor walking — footpath | Manage uneven surfaces |
| Crossing road | Traffic awareness, timed crossing |
| Supermarket simulation | Trolley pushing, reaching shelves |
| Public transport | Steps, standing balance |
| Ramp/slope walking | Incline/decline management |
| Stairs — multiflight | Independence with/without rail |
2. Advanced ADL Training
| ADL | Training Strategy |
|---|---|
| Cooking | Bimanual tasks — affected UL as stabilizer |
| Laundry | Reaching, lifting, folding |
| Personal hygiene | One-handed techniques if needed |
| Writing | Affected hand or compensatory dominant hand |
| Mobile phone use | Affected hand keyboard tapping |
| Driving assessment | Referral if appropriate |
3. Cardiovascular Conditioning
- Aerobic exercise: walking, cycling, swimming — 3–5 days/week
- Target: 40–70% heart rate reserve (moderate intensity)
- Duration: build to 30–45 min continuous activity
- Reduces stroke recurrence risk — secondary prevention
- Monitor BP before/after exercise (target: <130/80 mmHg)
4. Falls Prevention Program
| Component | Detail |
|---|---|
| Home hazard assessment | Remove loose mats, improve lighting, grab rails |
| Hip strengthening | Reduces fall risk significantly |
| Tai Chi-based balance | Evidence-based fall prevention in elderly |
| Education | When/how to safely get up from floor |
| Hip protectors | Consider for high-risk patients |
MONTH 6 — MAINTENANCE, REVIEW & DISCHARGE PLANNING
1. Reassessment of All Outcome Measures
- Compare Month 6 values to baseline (Week 1)
- Document functional gains across all domains
- Identify residual deficits requiring ongoing therapy
2. Maintenance Exercise Program
| Component | Frequency | Duration |
|---|---|---|
| UL stretching (spastic muscles) | Daily | 30 min |
| LL strengthening | 3×/week | 30–45 min |
| Balance exercises | Daily | 20 min |
| Aerobic walking | 5×/week | 30–45 min |
| Mirror/mental practice | 5×/week | 20 min |
| Community walking | Daily | As tolerated |
3. Discharge Planning Checklist
| Criteria | Achieved? |
|---|---|
| Independent or supervised community ambulation | ☐ |
| Independent self-care ADLs | ☐ |
| Caregiver fully trained in HEP | ☐ |
| Home environment modified for safety | ☐ |
| Follow-up appointments scheduled | ☐ |
| Spasticity management plan established | ☐ |
| Secondary stroke prevention plan in place | ☐ |
| Psychological support arranged if needed | ☐ |
LONG-TERM TREATMENT SUMMARY
| Month | Primary Focus | Key Techniques |
|---|---|---|
| Month 2 | Advanced spasticity + Gait consolidation | ESWT, Botox + PT, Serial casting, Overground gait, RAS |
| Month 3 | Advanced UL rehab + Balance mastery | CIMT/mCIMT, Mirror therapy, Motor imagery, Perturbation training |
| Month 4 | Technology-assisted rehabilitation | Robotics, BWSTT, Lokomat, VR, FES cycling |
| Month 5 | Community reintegration + Functional independence | Outdoor ambulation, ADL training, Aerobic conditioning, Falls prevention |
| Month 6 | Maintenance + Discharge planning | HEP, Outcome review, Caregiver training, Secondary prevention |
OUTCOME MEASURES — BASELINE vs. MONTH 6 TARGETS
| Measure | Baseline (Week 1) | Target (Month 6) |
|---|---|---|
| MAS (Spasticity) | Grade 2–3 | Grade 0–1 |
| MRC LL Strength | 2–3/5 | 4–5/5 |
| Berg Balance Scale | < 40/56 | > 45/56 |
| TUG | > 20 sec | < 14 sec |
| 10MWT | > 0.4 m/s | > 0.8 m/s |
| 6MWT | < 200 m | > 300 m |
| Barthel Index | < 60 | > 85 |
| ARAT | < 20/57 | > 30/57 improvement |
| FAC | Level 2–3 | Level 4–5 |
Core Principle: Neuroplasticity does not have a fixed endpoint — even in chronic stroke, high-intensity, task-specific, repetitive practice continues to drive measurable cortical reorganization and functional improvement. Technology-assisted training (robotics, VR, FES) allows delivery of the required dose when manual therapy alone is insufficient. (Harrison's, p. 13833; Management of Stroke Rehabilitation, p. 47)