Prosthetic management after maxillectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"maxillectomy" AND "obturator prosthesis" AND "rehabilitation"
Finding Sources
Finding Sources
Searching PubMed
"maxillectomy" AND "obturator"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks and clinical images. Here is the full structured answer:
Prosthetic Management After Maxillectomy
Overview
Maxillectomy creates a communication between the oral cavity and the nasal/sinonasal cavities, resulting in impaired speech (hypernasal), swallowing, mastication, and facial aesthetics. Prosthetic management centers on the obturator prosthesis - a device that seals this defect to restore function. Management is a three-phase continuum led by the maxillofacial prosthodontist as part of the multidisciplinary team (MDT).
Pre-surgical Assessment
All patients with oral, maxillary, and mid-face tumors should be assessed by the maxillofacial prosthodontist before surgery:
- Panoramic dental radiograph (OPG) + detailed oral examination
- Assessment of remaining teeth - their periodontal status and role as future abutments
- Decision on dental extractions, restorations, and implant planning
- Pre-operative impressions of the palate to fabricate the immediate surgical obturator
- Patient counseling regarding aims, advantages, and limitations of prosthetic rehabilitation
Classification of Maxillectomy Defects (Aramany Classification)
| Class | Defect Description |
|---|---|
| I | Unilateral resection along the midline |
| II | Unilateral resection not involving midline (posterior) |
| III | Central resection (bilateral anterior) |
| IV | Anteroposterior resection crossing the midline |
| V | Posterior unilateral defect |
| VI | Anterior defect only |
The Aramany class influences prosthesis design, retention strategy, and complexity of rehabilitation.
Three Phases of Obturator Management
Phase 1 - Surgical (Immediate) Obturator
Fabricated pre-operatively from pre-surgical impressions and inserted at the time of surgery, before extubation.
Functions:
- Separates oral and nasal cavities immediately post-op
- Supports the surgical pack/dressing
- Holds the skin graft against the defect walls
- Maintains cheek contour and provides soft tissue support
- Allows early oral feeding and speech
Retention methods:
- Circumzygomatic or circummalar wires passed through loops on the obturator (see image below)
- Screws through the zygoma/remaining palatal bone
- In dentate patients, wire clasps on remaining teeth

Figure: Surgical obturator with loops for circum-zygomatic wires (Scott-Brown's Otorhinolaryngology)
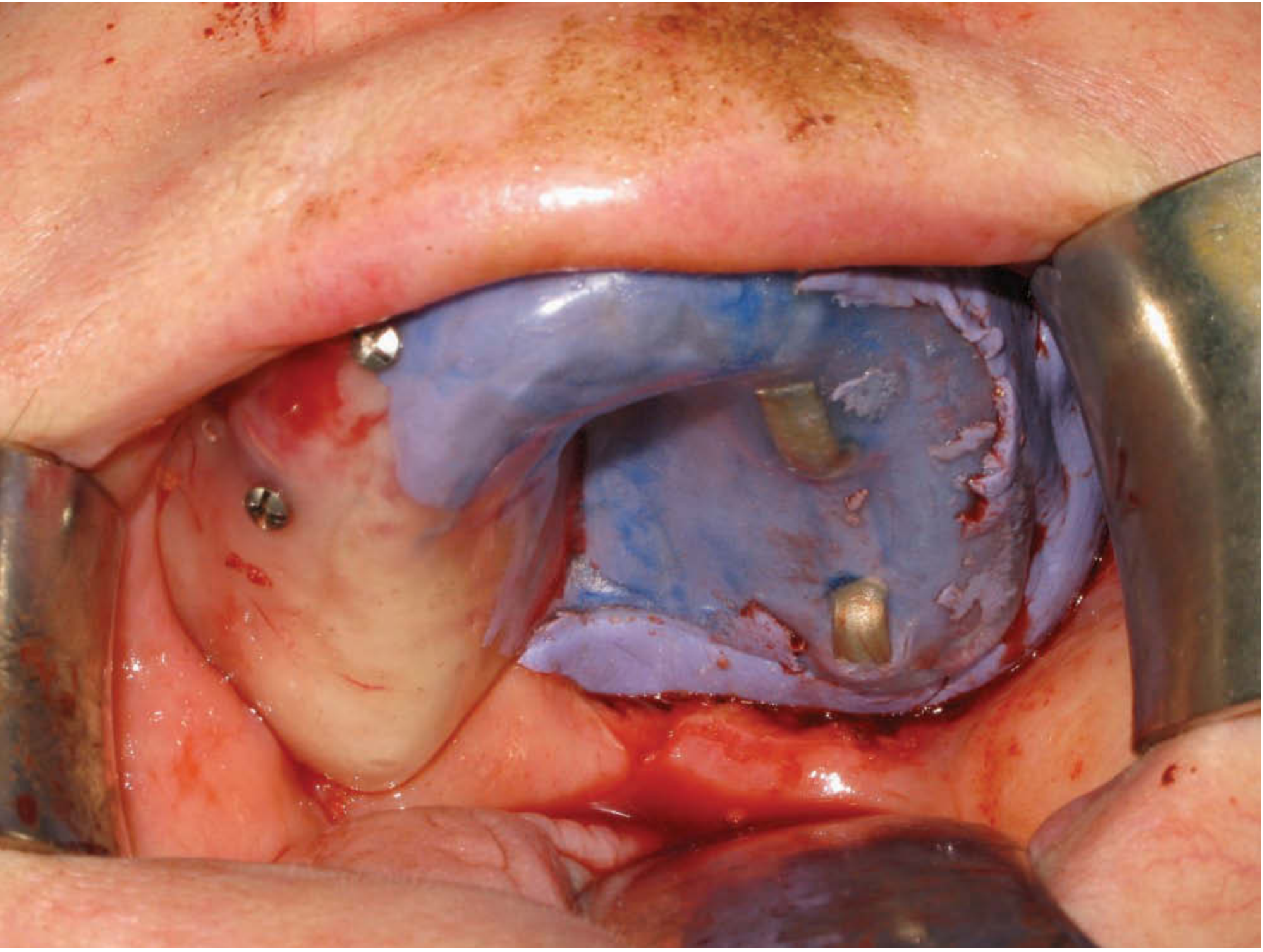
Figure: Screw-retained surgical obturator relined with silicone putty, intra-operatively (Scott-Brown's Otorhinolaryngology)
Materials used to obturate the defect:
- Addition-cured silicone putty (preferred by many - readily available, engages undercuts, provides rigid cheek support, assists haemostasis)
- Black gutta percha
- Foam-based products
Phase 2 - Interim (Transitional) Obturator
Provided approximately 4-6 weeks post-operatively as the defect contracts and heals:
- Replaces or substantially modifies the surgical obturator
- Allows progressive wound healing assessment
- Adjusted and relined regularly over the following months as the defect changes shape
- Carries prosthetic teeth for esthetics and early function
- Can incorporate soft silicone "bung" material to engage defect undercuts and aid retention
Key considerations during this phase:
- Trismus is common, especially when surgery is combined with radiotherapy - limits access for impression taking and prosthesis insertion; this must be planned for
- Defect continues to contract for 3-6 months post-surgery and post-radiotherapy
Phase 3 - Definitive Obturator
Constructed once the defect has stabilized (usually 6-12 months post-surgery, or after completion of adjuvant radiotherapy and adequate tissue recovery):
- Optimized for function, retention, and esthetics
- May include prosthetic teeth in full occlusion
- For low-level partial maxillectomy, a soft silicone bung engages defect undercuts and assists retention alongside dental clasps
The definitive obturator fabricated in synthetic polymer (acrylic resin base) provides oronasal separation, yielding normal speech and swallowing. It allows direct visualization of the defect for tumor surveillance - an important oncological advantage over free tissue transfer.
Surgical Modifications to Facilitate Obturator Provision
Surgeons should work in coordination with the prosthodontist:
- Palatal mucosal incisions should be made laterally to bone cuts to create a keratinized mucosal flap over the cut palatal bone edge - acts as a cushion/fulcrum for the prosthesis during masticatory function
- Split-skin graft to the cheek defect - produces a scar band which engages the obturator and provides retention (particularly important for conventional obturators without implants)
- Inferior turbinate removal - provides vertical space for the obturator elements and prevents trauma
- Abutment teeth - periodontal health must be maintained, as remaining teeth are vital for obturator support, retention, and stability
Multi-part Obturators and Osseointegrated Implants
Multi-part Design
Used when:
- The defect is large
- Significant trismus limits access (prosthesis inserted in two parts and joined intra-orally)
- For posterior maxilla defects where access is restricted
A separate dental prosthesis component joins the obturator component intra-orally.
Osseointegrated (Endosseous) Implants
Implants dramatically improve obturator retention and stability, especially in:
- Edentulous patients (no teeth for clasping)
- Large defects (limited remaining bone and soft tissue support)
- Patients in whom conventional retention is inadequate
Placement options:
- At the time of primary surgery (primary/simultaneous implant placement)
- As part of secondary definitive rehabilitation
Zygomatic implants are particularly useful after total maxillectomy where alveolar bone is absent - they anchor in the zygomatic arch and can support an obturator or fixed prosthesis. A 2025 study (Kumari et al., JMOS) specifically addresses rehabilitation using zygoma implants in maxillectomy patients.
A novel technique described in recent literature uses an intramucosal retention system to improve obturator stability without implants (Alves et al., 2024, PMID 38963534).
Obturator vs. Free Flap Reconstruction
| Factor | Obturator | Free Flap |
|---|---|---|
| Invasion | Non-invasive | Requires second surgical site |
| Tumor surveillance | Direct visualization of defect | Limited inspection |
| Complexity | Requires ongoing maintenance | Single surgical procedure |
| Large/complex defects | Difficult; retention challenging | Better HRQoL with microvascular flap for complex resections |
| Edentulous patients | Worse outcomes vs. dentate | Offers bone for implants |
| Radiotherapy effect | Worsens mouth opening and oral/swallowing function | Also affected but anatomically more stable |
Obturator prosthesis is a highly positive and non-invasive approach to improve quality of life for maxillectomy defects - Scott-Brown's Otorhinolaryngology, p. 390. For large complex resections (palate + maxilla + sinuses + orbit), microvascular reconstruction may give better HRQoL outcomes.
Prosthetic Management of Facial Defects
After total maxillectomy or mid-facial resections involving the orbit and nose:
- Extra-oral facial prostheses (nasal, orbital, or combined auricular prostheses) may be required
- Facial prostheses are fabricated from medical-grade silicone, intrinsically or extrinsically colored to match skin
- Retention via: spectacle frames, adhesives, magnets, or osseointegrated implants (craniofacial implants)
- Osseointegrated implants in the supraorbital rim, zygomatic arch, or mastoid region provide superior retention over adhesives
Dental Rehabilitation Considerations
Post-ablative surgery patients face significant dental challenges:
- High rates of dental phobia and anxiety
- Many are edentulous at presentation
- Resective surgery removes sections of dentition
- Adjuvant radiotherapy causes xerostomia, increased caries risk, and osteoradionecrosis risk
- Bulky soft-tissue free flaps can obstruct dental rehabilitation (vestibuloplasty and flap reduction may be needed)
Pre-surgical decisions on remaining teeth must weigh:
- Patient motivation and oral hygiene
- Tumour site, stage, and prognosis
- Adjuvant radiotherapy dose/fields and effect on remaining teeth
- Implant timing and site planning
Summary Flowchart
Diagnosis → Pre-surgical assessment (prosthodontist + MDT)
→ Dental treatment / OPG / implant planning
→ Surgery + IMMEDIATE SURGICAL OBTURATOR (inserted pre-extubation)
→ 4-6 weeks → INTERIM OBTURATOR (serial relining/adjustments)
→ 6-12 months (after RT recovery) → DEFINITIVE OBTURATOR
↓ (if retention inadequate or edentulous)
Osseointegrated / zygomatic implants → implant-retained obturator or fixed prosthesis
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 31 (Prosthetic Rehabilitation), pp. 542-549
- K.J. Lee's Essential Otolaryngology, Palatal Reconstruction, p. 851
- Cummings Otolaryngology Head and Neck Surgery, Hard Palate and Subtotal/Total Maxillectomy chapters
This is a shared conversation. Sign in to Orris to start your own chat.