Pheochromocytoma tabulated notes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data. Let me compile the full tabulated notes:
Pheochromocytoma - Tabulated Notes
1. Overview
| Feature | Detail |
|---|---|
| Definition | Neoplasm of chromaffin cells (adrenal medulla) that synthesizes and releases catecholamines |
| Cell of origin | Chromaffin cells (neural crest-derived) |
| Synonym | "Paraganglioma" when arising at extraadrenal sites |
| Incidence | 2-8 cases/million/year; found in 0.2-0.6% of hypertensive patients |
| Significance | Surgically correctable cause of hypertension; can cause fatal hypertensive crises if missed |
2. The "10% Rules"
| Rule | Detail |
|---|---|
| 10% extraadrenal | Organ of Zuckerkandl (aortic bifurcation/origin of IMA), carotid body, bladder, sympathetic ganglia |
| 10% bilateral | Rises to ~50% in familial syndromes |
| 10% malignant | Up to 20% malignancy in extraadrenal tumors |
| 10% normotensive | Increasingly found on incidental imaging |
| 10% in children | More common in hypertensive children (~1.7%) |
| >10% familial | Proportion has risen; genetic testing now standard |
| >10% metastatic at diagnosis | Also increasing in recent series |
Note: The strict 10% rule is now considered outdated and applies best to familial/syndromic cases. - Robbins & Kumar Basic Pathology
3. Genetics & Associated Syndromes
| Syndrome | Gene | Chromosome | Pheo Features | Other Features |
|---|---|---|---|---|
| MEN2A | RET (proto-oncogene) | 10q11 | ~50%, often bilateral | Medullary thyroid carcinoma, parathyroid adenoma, cutaneous lichen amyloidosis |
| MEN2B | RET | 10q11 | Usually bilateral | Medullary thyroid carcinoma, mucosal/submucosal neuromas, marfanoid habitus, Hirschsprung disease |
| Von Hippel-Lindau (VHL) type 2 | VHL (tumor suppressor) | 3p25-26 | ~20% get pheo/paraganglioma | Retinal & cerebellar hemangioblastomas, clear cell renal carcinoma, pancreatic neuroendocrine tumors |
| Neurofibromatosis type 1 (NF1) | NF1 (tumor suppressor) | 17q11.2 | ~2%, usually adrenal | Café au lait spots, neurofibromas, Lisch nodules, axillary freckling |
| SDHx mutations | SDHA/B/C/D | Various | Higher metastatic risk (SDHB) | Paraganglioma syndromes; SDHB associated with malignant disease |
| Sporadic | Multiple (RET, VHL, NF1, EPAS1, SDHx) | - | ~40% carry somatic mutations | - |
Pathogenic mechanisms:
- RET, NF1 → enhanced growth factor receptor signaling
- VHL, SDHx subunits, EPAS1 → increased hypoxia-inducible factor (HIF) activity
4. Clinical Presentation
| Feature | Detail |
|---|---|
| Classic triad | Headache, sweating attacks, hypertension (present in ~95% in large series) |
| Hypertension pattern | Sustained in majority; paroxysmal in ~2/3 |
| Paroxysmal episode contents | Abrupt BP rise + tachycardia, palpitations, headache, diaphoresis, tremor, apprehension, nausea/vomiting, abdominal/chest pain |
| Triggers of paroxysms | Palpation of tumor, physical exertion, drugs (e.g., tricyclics, dopamine antagonists), anesthesia induction, surgery |
| Acute complications | Congestive heart failure, pulmonary edema, MI, ventricular fibrillation, CVA |
| Chronic complications | Catecholamine cardiomyopathy, catecholamine-induced vasculitis |
| Other hormones secreted | ACTH, somatostatin (can cause Cushing's features) |
| Micturition syncope | Pathognomonic of bladder paraganglioma |
Physical signs in syndromic patients:
- Café au lait spots + neurofibromas → NF1
- Retinal hemangiomas → VHL
- Port wine stain → Sturge-Weber
- Marfanoid habitus + mucosal neuromas → MEN2B
- Subungual fibromas, ash leaf patches, adenoma sebaceum → tuberous sclerosis
5. Morphology & Histology
| Feature | Detail |
|---|---|
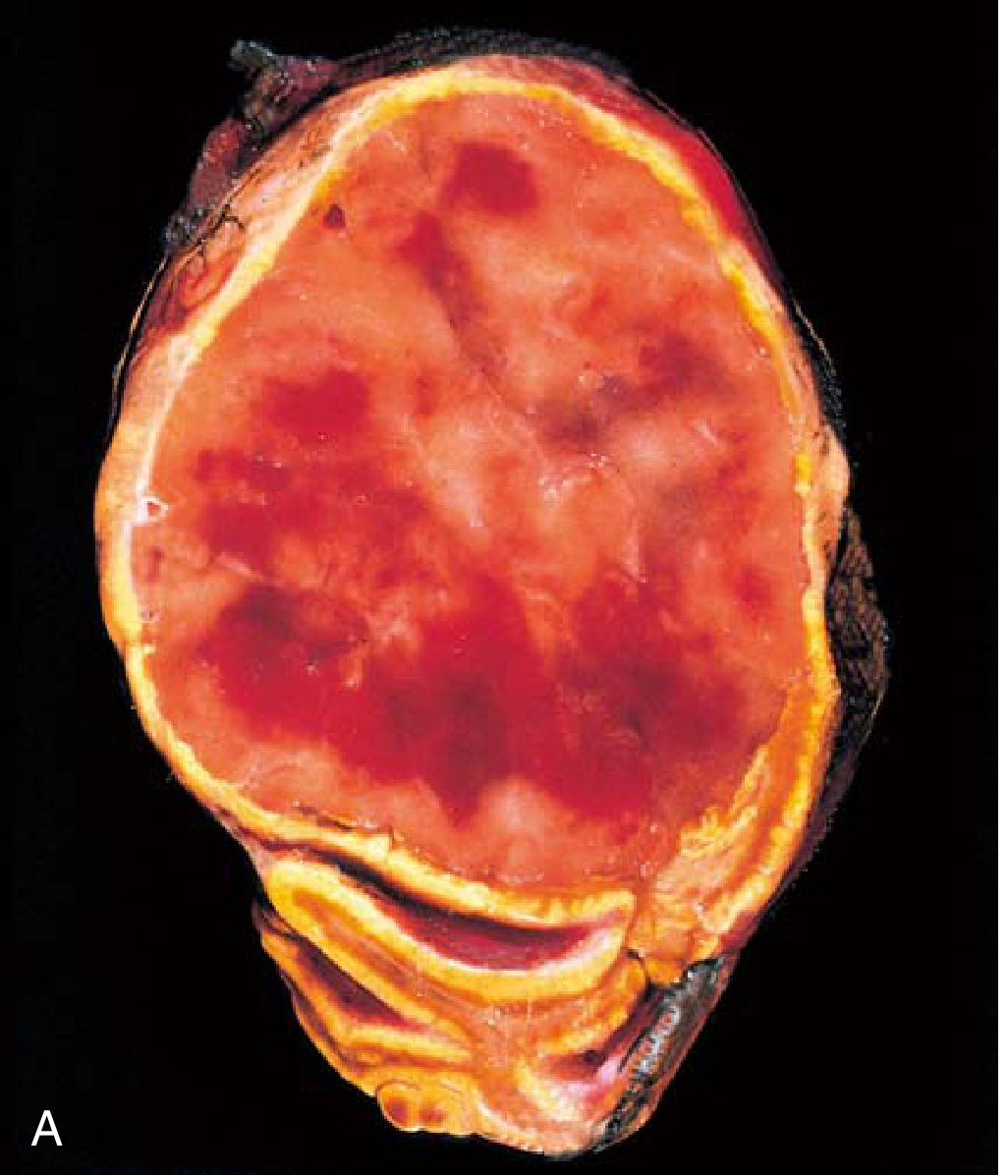
| Gross appearance | Yellow-tan, well-circumscribed; large tumors are hemorrhagic, necrotic, cystic |
| Size | Small confined lesions to several-kilogram masses |
| Dichromate test | Turns dark brown with potassium dichromate (oxidizes catecholamines) |
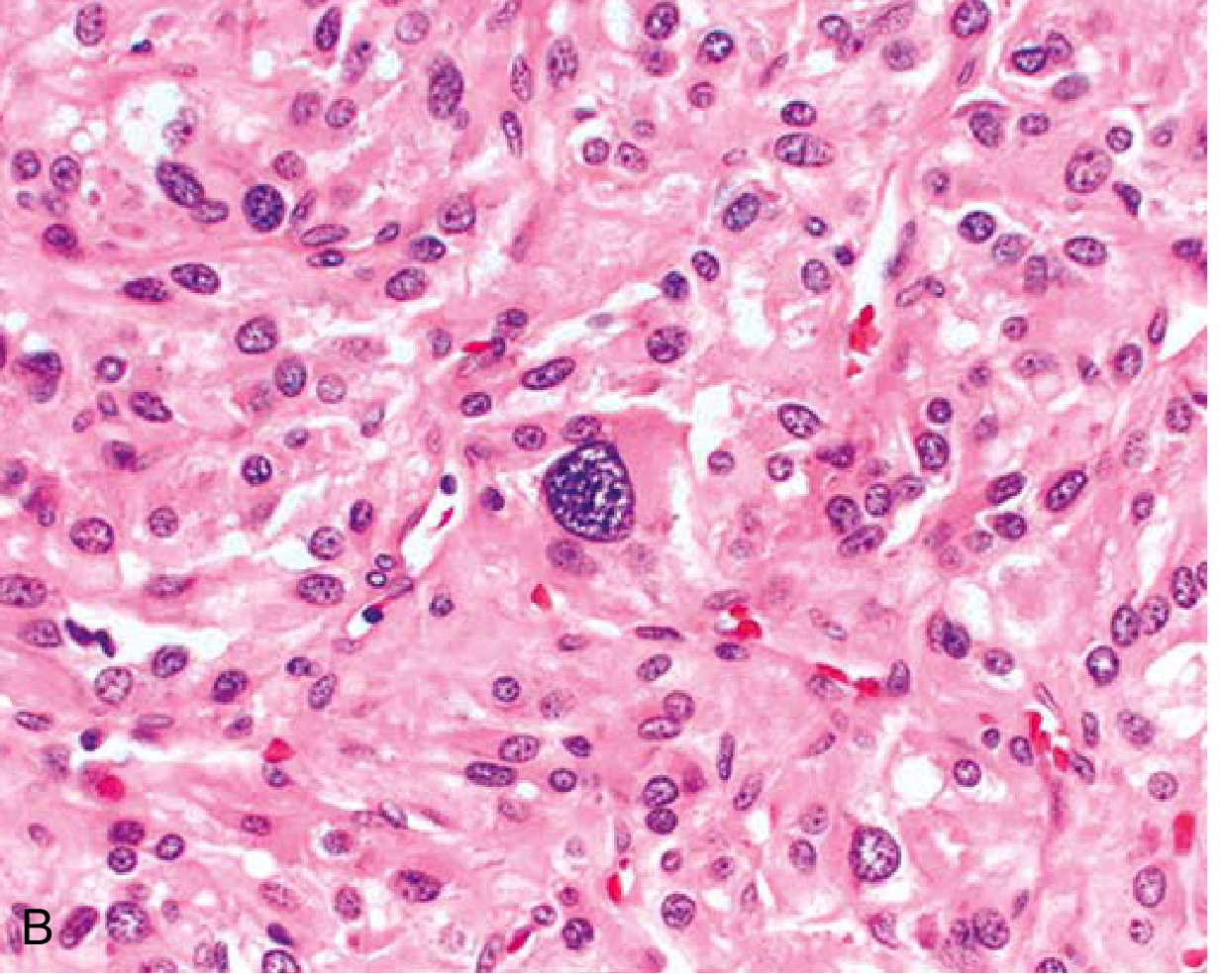
| Microscopy | Polygonal-to-spindle chromaffin cells in "zellballen" (small nests) separated by rich vascular network |
| Cytoplasm | Finely granular (catecholamine-containing granules); highlighted by silver stains |
| Nuclei | Often pleomorphic even in benign tumors |
| EM finding | Variable membrane-bound, electron-dense secretory granules |
| Malignancy criterion | Only by the presence of metastases (not by histological features alone) |
| Metastatic sites | Regional lymph nodes, liver, lung, bone |
6. Biochemical Diagnosis
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Plasma-free metanephrines (metanephrine + normetanephrine) | 96-100% | 85-89% (drops to 77% in >60 yrs) | Best screening test; high sensitivity but many false positives |
| 24-hr urine fractionated metanephrines + catecholamines | 98% | 98% | Best confirmatory test; two collections recommended |
| Urinary VMA (vanillylmandelic acid) | Lower (historical) | - | Less used now; replaced by fractionated metanephrines |
| Clonidine suppression test | - | - | 0.3 mg oral clonidine → measure plasma normetanephrine; used for equivocal results |
Cutoff principle: Values >2x upper limit of normal on urine testing = positive
Drugs/conditions causing false positives:
- Tricyclics, levodopa, cocaine, amphetamines, ephedrine, pseudoephedrine, phencyclidine, LSD, isoproterenol
- Clonidine/alcohol withdrawal
- Subarachnoid hemorrhage, migraine, preeclampsia, acute illness
7. Localization & Imaging
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| CT (with/without contrast) | 90-100% | ~70% | First-line; HU >10, vigorous early enhancement, <60% washout; 5 mm slices |
| MRI | Slightly higher than CT | ~70% | Preferred in pregnancy, children, lactation, CT contrast allergy; T2-weighted hyperintense ("light-bulb sign") |
| MIBG scintigraphy (¹²³I or ¹³¹I) | 77-90% | Very high | Reserved for suspected multifocal/malignant disease; high specificity |
| ⁶⁸Ga-DOTATATE PET/CT | 97.6% | High | Best overall lesion detection; superior to FDG-PET (49%) and ¹⁸F-DOPA PET (75%) |
| ¹⁸F-DOPA PET/CT | 75% | High | Good for hereditary cases |
| ¹⁸F-FDG PET/CT | 49% | - | Useful for SDHB-related metastatic disease |
Important rule: Always confirm biochemically before imaging.
8. Perioperative Management
| Step | Detail |
|---|---|
| Alpha-blockade first | Start 7-14 days preoperatively (longer if cardiomyopathy/vasculitis) |
| Preferred alpha-blocker | Phenoxybenzamine (irreversible, non-selective) - initial 10 mg BD, titrate to 20-100 mg/day |
| Alternative alpha-blocker | Doxazosin (selective α1) - start 1 mg at night; increasingly preferred |
| BP targets (seated) | <120/80 mmHg seated; systolic >90 mmHg standing |
| Beta-blockade | ONLY after adequate alpha-blockade (risk of unopposed alpha stimulation = worse hypertension if given first) |
| Beta-blocker indication | HR >80 bpm after alpha-blockade; e.g., extended-release metoprolol 25 mg once daily |
| High-sodium diet | ≥5000 mg/day (to reverse catecholamine-induced volume contraction and alpha-blockade-related orthostasis) |
| Additional agents | Metyrosine (α-methyl-p-tyrosine, 250 mg q6h) - inhibits catecholamine synthesis; amlodipine up to 20 mg/day |
| Intraoperative hypertensive crisis | IV sodium nitroprusside, phentolamine, or nicardipine (NOT beta-blockers) |
| Perioperative mortality | Historically 26-50%; now ~1% at specialty centers |
9. Surgical Management
| Feature | Detail |
|---|---|
| Treatment of choice | Complete surgical resection |
| Surgical survival rate | 98-100% |
| Preferred approach | Laparoscopic adrenalectomy for most tumors |
| Open approach | Large (>6 cm), malignant, or locally invasive tumors |
| Pheo-specific consideration | Early ligation of adrenal vein to minimize catecholamine spillage |
| Post-excision BP | May drop significantly (have IV fluids and vasopressors ready) |
| Hypertension cure rate | ~75% (rest may have persistent essential hypertension) |
| Postop monitoring | 24-48 hr ICU; glucose monitoring (rebound hypoglycemia from insulin release) |
10. Metastatic/Malignant Pheochromocytoma
| Feature | Detail |
|---|---|
| Definition of malignancy | Presence of metastases only (no reliable histological criteria) |
| Incidence | >10% metastatic at diagnosis (rising) |
| Risk factors | Extraadrenal location, large size, SDHB mutation (highest risk) |
| Metastatic sites | Lymph nodes, bone, liver, lung |
| Treatment options | ¹³¹I-MIBG therapy, CVD chemotherapy (cyclophosphamide + vincristine + dacarbazine), sunitinib, ⁶⁸Ga-DOTATATE-guided PRRT, metyrosine for symptom control |
| 5-year survival | ~50% for metastatic disease |
11. Follow-Up
| Parameter | Detail |
|---|---|
| Annual biochemical testing | Fractionated plasma/urine metanephrines for life (detects recurrence, delayed primaries, metastatic disease) |
| Imaging follow-up | Not needed unless biochemistry becomes elevated |
| Genetic testing | Recommended for all patients, especially young age (<40), bilateral, extraadrenal, malignant, or family history |
| Family screening | Offered to first-degree relatives if germline mutation identified |
12. Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Essential hypertension | No paroxysms; normal catecholamines |
| Panic disorder | Normal catecholamines; normal BP between attacks |
| Hyperthyroidism | Thyroid function tests elevated; TFTs differentiate |
| Carcinoid syndrome | Flushing + diarrhea; elevated urine 5-HIAA |
| Autonomic epilepsy | EEG changes; no catecholamine elevation |
| Drug withdrawal (clonidine) | History; resolves with reinstatement |
| Renovascular hypertension | Renal artery imaging; normal catecholamines |
| Adrenal carcinoma | Non-functional or cortisol-secreting; different biochemistry |
13. Key Points / Exam Mnemonics
| Mnemonic | Meaning |
|---|---|
| 5 Hs | Headache, Hypertension, Hyperhidrosis, Hyperglycemia, Heart palpitations |
| "10% tumor" | 10% extraadrenal, bilateral, malignant, normotensive, familial, in children |
| Alpha before Beta | NEVER start beta-blockade before alpha-blockade |
| Zellballen | Pathognomonic nest-like histological pattern |
| "Light-bulb sign" | Bright T2 signal on MRI |
| PHEO = Paraganglioma/pheo Has Extra Origins | Neural crest → chromaffin cells → both adrenal and extraadrenal sites |
Sources: Robbins & Kumar Basic Pathology; Sabiston Textbook of Surgery 21e; Goldman-Cecil Medicine; Brenner & Rector's The Kidney; Current Surgical Therapy 14e; Campbell Walsh Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.