Reamer irrigator aspirator in orthopaedics 10 mark pg answer with flow chart and images
Reading File
Finding Sources
Finding Sources
Searching the Web
Reamer Irrigator Aspirator RIA orthopaedics mechanism indications complications autograft
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
I now have everything needed for a comprehensive 10-mark answer. Let me compose the full structured response.
Reamer Irrigator Aspirator (RIA) in Orthopaedics
Definition
The Reamer-Irrigator-Aspirator (RIA) is a single-pass intramedullary reaming device that simultaneously reams the medullary canal while delivering irrigation fluid distally and aspirating bone marrow, morselized bone, and debris proximally through a collection filter. It was originally developed by Synthes (now DePuy Synthes) to minimize the embolic complications of conventional intramedullary reaming, and its role has expanded significantly to include autologous bone graft harvest.
Device Components
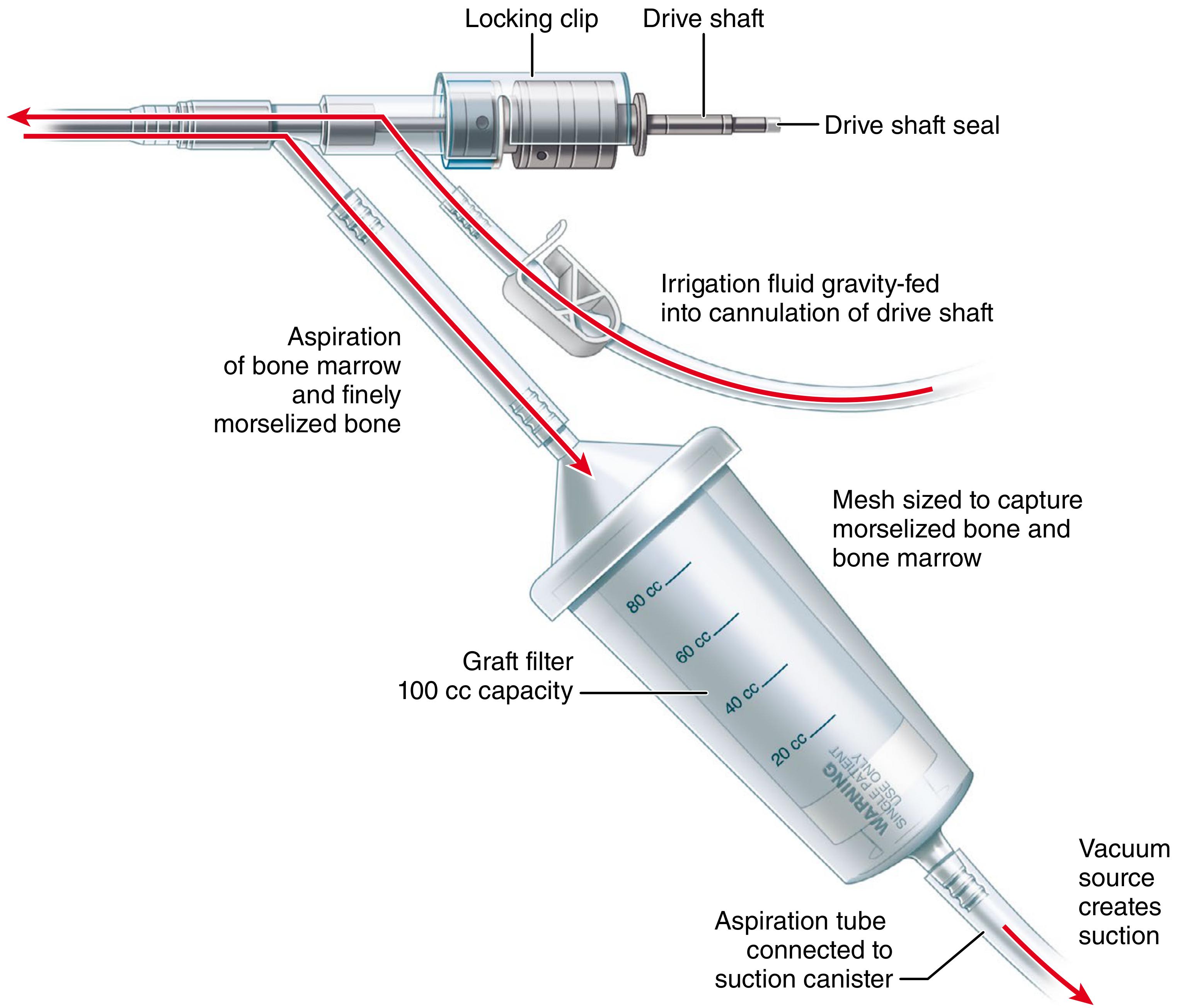
Figure 1: RIA device components - Campbell's Operative Orthopaedics, 15th Ed
| Component | Function |
|---|---|
| Reamer head (10-18 mm, 0.5 mm increments) | Cuts the endosteum; single-pass design |
| Drive shaft (hollow/cannulated) | Conducts irrigation fluid distally |
| Locking clip + drive shaft seal | Ensures sealed, pressurized system |
| Irrigation inlet | Delivers 0.9% saline gravity-fed |
| Aspiration outlet | Suction removes bone marrow, morselized bone, debris |
| Graft filter (100 cc capacity, mesh) | Collects bone graft from aspirate |
| Vacuum suction canister (2-5 L) | Houses the suction |
Mechanism of Action
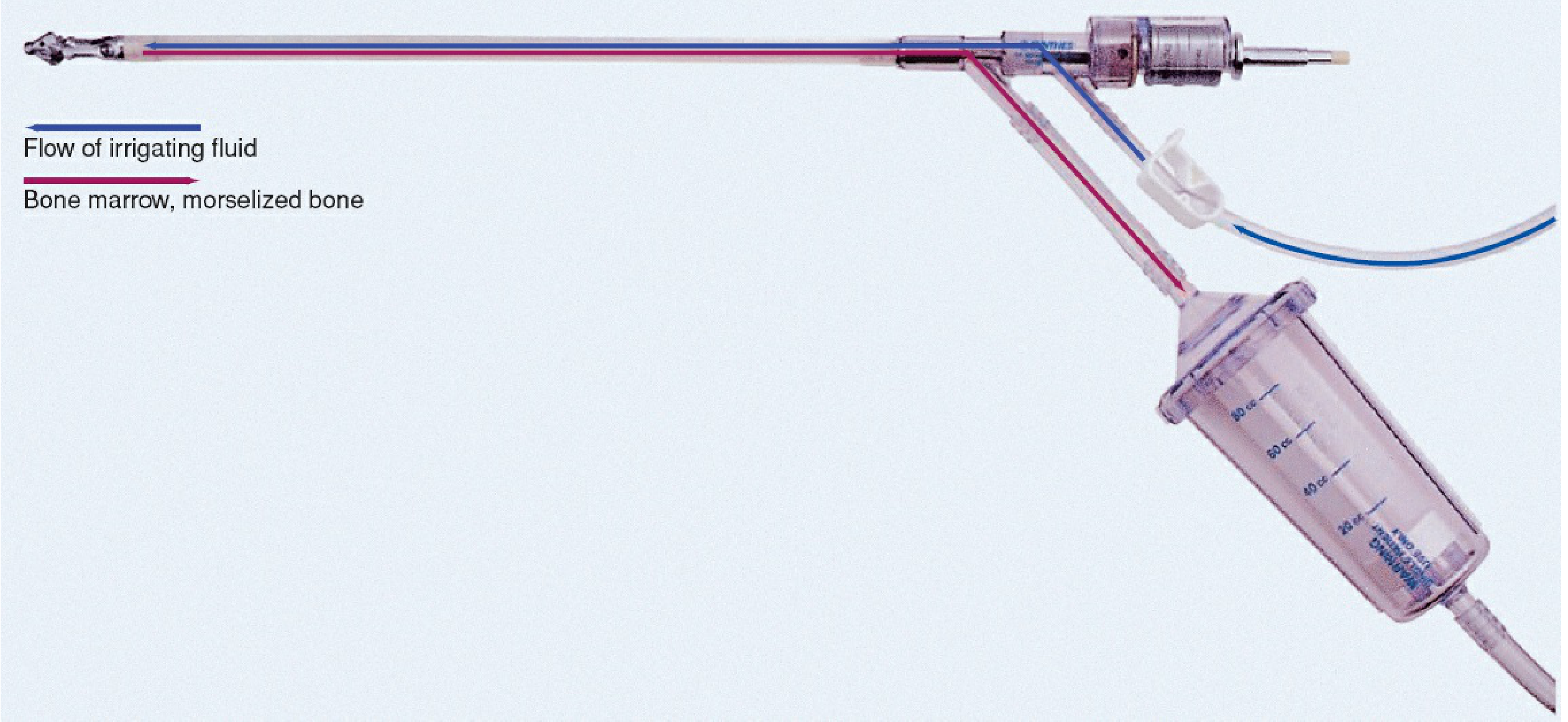
Figure 2: RIA fluid dynamics - Rockwood & Green's Fractures in Adults, 10th Ed
The key innovation is a bidirectional fluid circuit:
- Irrigation saline travels down through the hollow drive shaft to the reamer tip (cools and lubricates)
- Bone marrow, morselized bone, and debris are aspirated back up to the collection filter
- This prevents intramedullary pressure build-up, which is the primary driver of fat/marrow embolism in conventional reaming
- Reamings contain pluripotent mesenchymal stem cells, osteogenic growth factors (BMPs, IGF, VEGF), and mineralized bone fragments - making the aspirate a rich autograft source
FLOWCHART: RIA Surgical Technique
PREOPERATIVE PLANNING
|
▼
Measure isthmus diameter on X-ray/fluoroscopy
|
▼
Select reamer head: isthmus diameter + 1 to 1.5 mm (bone graft harvest)
OR isthmus + up to 4 mm (IM nail preparation)
|
▼
Position patient (supine/lateral for femur; supine for tibia)
|
▼
Standard IM nail entry point (piriformis fossa or trochanteric entry)
|
▼
Insert guidewire (reaming wire) down to physeal scar
Confirm: AP + lateral fluoroscopy
|
▼
Assemble RIA device:
→ Drive shaft → Locking clip → Drive shaft seal → Power drill
→ Irrigation tubing (saline 0.9%) → Aspiration tubing → Graft filter → Suction
|
▼
Position RIA over guidewire
Start irrigation + aspiration BEFORE inserting into bone
|
▼
Insert reamer; confirm position with image intensification
|
▼
REAMING TECHNIQUE (advance 20-30mm, retract 50-80mm, repeat)
"NEVER ream without active irrigation and aspiration"
|
▼
Continue until desired endpoint on fluoroscopy
(Reverse reamer direction if resistance encountered)
|
▼
Remove RIA from canal
STOP irrigation; clamp suction tubing
|
▼
Check fluoroscopy: evaluate for cortical perforation/fracture
|
▼
Compress graft in filter with plunger
Invert filter → push out bone graft into container
(Typical yield: 60-80 cc per femur)
|
▼
Close wound in layers (as for standard IM nailing)
Indications
Primary Indications (AO Foundation approved):
- Autologous bone graft harvest - to fill bone defects, facilitate arthrodesis/fusion, treat nonunions
- Canal clearance for intramedullary nail fixation - reduces embolic load vs. conventional reaming
- Sizing the medullary canal for IM implant or prosthesis
- Intramedullary osteomyelitis - removes infected, necrotic tissue and bone from canal
Extended/Reported Indications:
- Segmental bone defects (average defect 5.8 cm; 90% union at 12 months reported)
- Recalcitrant nonunions - combined RIA + rhBMP-2 for tibial nonunions
- Impending pathological fractures - reduces embolic load during reaming in tumor patients
- Ankle/subtalar arthrodesis with IM nail fixation
- Mesenchymal stem cell (MSC) harvest - the flow-through fraction is enriched with MSCs
Advantages Over Iliac Crest Bone Graft (ICBG)
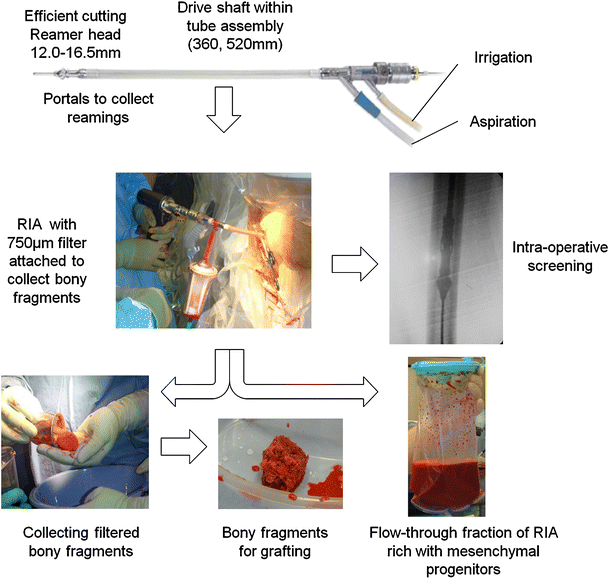
Figure 3: RIA surgical workflow from reaming to bone graft collection (Springer)
| Parameter | RIA | ICBG |
|---|---|---|
| Volume of graft | 38-48 cc mean (up to 80 cc) | ~20 cc (anterior ICBG) |
| RIA yields | 17 cc MORE than anterior ICBG on average | Standard |
| Complication rate | 1.4-6.0% | 19.4-30% |
| Donor site pain | Significantly less (p<0.004) | Chronic in up to 20% |
| Additional incision | None (same limb) | Yes (hip) |
| Graft quality | Comparable or superior osteogenic cell content | Gold standard |
| Union rates | Comparable or better | Comparative standard |
| Cost | Less than DBM allograft or BMP per 10 cc | Moderate |
Graft Biology
The aspirate contains:
- Morselized cortical and cancellous bone (osteoconductive scaffold)
- Bone marrow with hematopoietic and osteogenic progenitor cells
- Pluripotent mesenchymal stem cells capable of osteoblast differentiation
- Growth factors: BMP-2, BMP-7, IGF-1, TGF-beta, VEGF, PDGF
- In quantitative analysis, RIA aspirate growth factor concentrations are comparable or superior to ICBG (Rockwood & Green's, p.1022)
Complications and Prevention
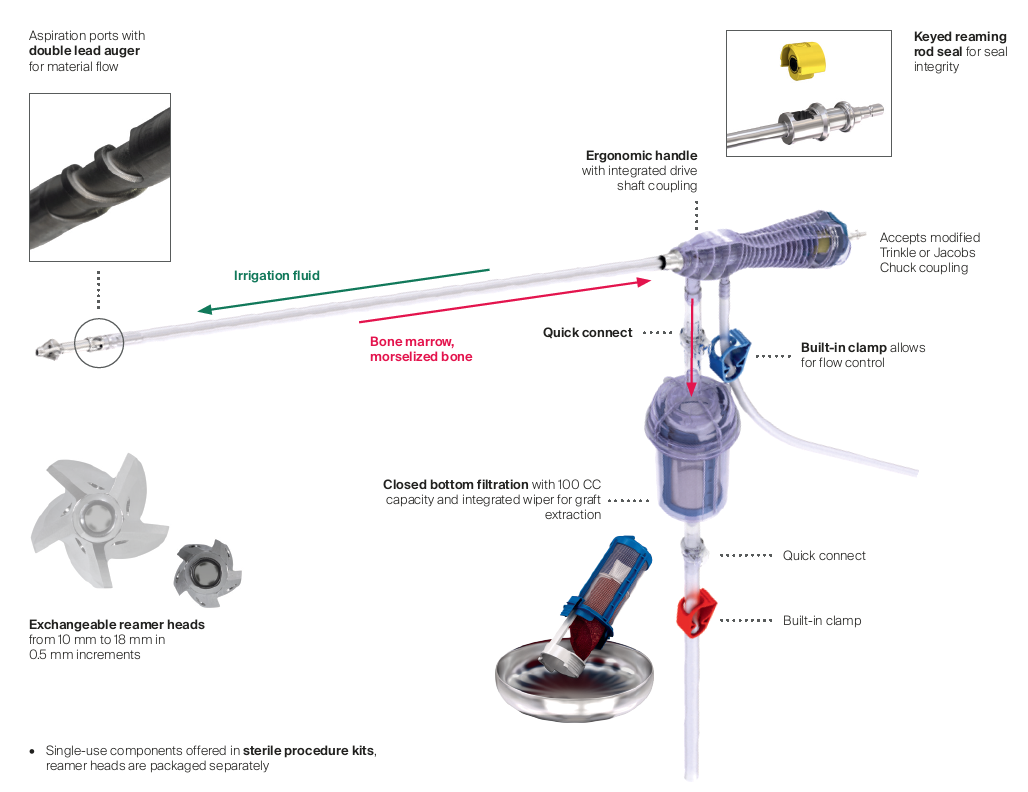
Figure 4: RIA2 system components (AO Foundation)
Complication Table (Campbell's Operative Orthopaedics, 15th Ed - Table 58.5):
| Complication | Incidence | Prevention |
|---|---|---|
| Cortical perforation | Most common (34/1834 cases) | Preop X-ray of donor bone; measure isthmus; check for deformity |
| Donor bone fracture | Reported (5 cases by Lowe et al.) | Avoid osteoporotic patients; protect postop weight-bearing; avoid thin cortices |
| Excessive blood loss / transfusion | 44% required transfusion; mean Hb drop 3.74 g/dL | Stop aspirator when not reaming; have blood available; recheck Hct at 24 hrs |
| Fat/marrow embolism | Reduced vs. conventional reaming | Continuous irrigation and aspiration; RIA design prevents pressure build-up |
| Intraoperative cardiac events | Rare but severe | Monitor continuously; have anesthetic support ready |
| Device failure (reamer head breakage) | 6/1834 cases | Correct torque (3.5-4.5 Nm), 700-900 RPM; avoid young high-BMI patients |
| Wound infection | Rare (similar IM nailing wound) | Standard aseptic technique |
Overall complication rate: 1.7% (Laubach et al., systematic review of 1,834 procedures) - Rockwood & Green's, p.1021
Contraindications
- Osteoporosis / osteopenia - risk of donor bone fracture (thin cortices)
- Deformed medullary canal (post-malunion, congenital deformity) - risk of perforation
- Active infection at entry site
- Canal too narrow to accommodate reamer head safely
- Patients with pre-existing fracture of donor bone
Postoperative Care
Per Campbell's Operative Orthopaedics (Technique 58.3):
- Cadaver studies confirm RIA does not dramatically diminish femoral mechanical properties
- Weight-bearing to tolerance is permitted in the donor limb
- Restrictions apply only if concomitant injuries or fixation dictates
- Monitor Hematocrit at end of procedure and at 24 hours
RIA vs. Conventional Reaming (for IM Nailing)
| Feature | Conventional Reaming | RIA |
|---|---|---|
| Intramedullary pressure | Markedly elevated | Minimal (suction relieves it) |
| Fat/marrow embolism | High risk | Significantly reduced |
| Reamer passes | Multiple | Single-pass |
| Bone graft recovery | Lost | Collected (60-80 cc) |
| Pulmonary complications | Higher | Comparable or lower |
Summary Points for Exam
- RIA = one-pass reamer with simultaneous irrigation (distal) + aspiration (proximal)
- Originally designed to reduce fat embolism during IM reaming
- Key advantage: harvests 60-80 cc autologous bone graft from femoral/tibial canal
- Graft contains MSCs, growth factors, morselized bone - osteogenic, osteoconductive, osteoinductive
- Complication rate 1.7% vs. ICBG 19-30%; donor site pain significantly less
- Main complications: cortical perforation, blood loss/transfusion, fracture
- Contraindicated in osteoporosis and deformed canals
- Extended use: osteomyelitis debridement, segmental defects, nonunions, ankle fusion
- Reamer head = isthmus diameter + 1-1.5 mm for graft harvest
- Never ream without active irrigation and aspiration
Sources: Rockwood & Green's Fractures in Adults, 10th Ed (2025), pp.1021-1022 | Campbell's Operative Orthopaedics, 15th Ed (2026), Technique 58.3, Table 58.5 | AO Foundation RIA-FAQ | Laubach et al., systematic review of 1,834 RIA procedures
This is a shared conversation. Sign in to Orris to start your own chat.