Eusrachian tube patency tests in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Eustachian tube" AND "patency test"
Searching the Web
Eustachian tube patency tests RGUHS 20 marks Scott Brown Cummings Dhingra recent advances 2024
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"Eustachian tube" AND "function test" AND dysfunction
Reading File
Reading File
Reading File
Reading Article
PMID: 37246976
Reading Article
PMID: 39767171
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading Article
PMID: 39368418
Finding Sources
Reading File
Searching PubMed
"Eustachian tube" AND ("balloon dilation" OR tubomanometry OR sonotubometry)
Reading Article
PMID: 40729971
Loading Image
I now have all the material needed. Let me compile the comprehensive 20-mark RGUHS answer with diagrams and flowcharts.
Eustachian Tube (ET) Patency Tests - A Comprehensive 20-Mark Answer
Sources: Cummings Otolaryngology (Flint), Scott-Brown's Otorhinolaryngology Vol 2, Shambaugh Surgery of the Ear, K.J. Lee's Essential Otolaryngology, with recent advances
INTRODUCTION
The Eustachian tube (ET) is a mucosal-lined channel of approximately 35-36 mm in adults connecting the middle ear cleft to the nasopharynx. It was first described by Bartolomeo Eustachi in 1562, though Alcmaeon of Croton noted it much earlier. Its three cardinal functions are:
- Ventilation/Pressure equalization - equalizing middle ear pressure with atmospheric pressure
- Drainage/Mucociliary clearance - clearing secretions from the middle ear
- Protection - preventing reflux of nasopharyngeal organisms and loud sounds
Key anatomical facts (K.J. Lee's Essential Otolaryngology):
- Length: 17-18 mm at birth; 35 mm in adulthood
- Cartilaginous (anteromedial) portion: 24 mm; Bony (posterolateral) portion: 11 mm
- The narrowest part (isthmus) is at the bony-cartilaginous junction
- Inclination: horizontal at birth, 45° by adulthood
- Pressure needed to open: 200-300 mm H₂O in a normal individual
- Valsalva generates 20-40 mm Hg pressure
- Critical pressure difference (locking): 90 mm Hg
CLASSIFICATION OF ET PATENCY TESTS
┌────────────────────────────────────────────────────────────────────┐
│ EUSTACHIAN TUBE PATENCY TESTS │
├──────────────────────────┬─────────────────────────────────────────┤
│ CLINICAL / BEDSIDE │ INSTRUMENTAL/OBJECTIVE │
├──────────────────────────┼─────────────────────────────────────────┤
│ 1. Valsalva manoeuvre │ 1. Tympanometry (standard) │
│ 2. Toynbee test │ 2. Nine-step inflation-deflation test │
│ 3. Politzer's method │ 3. Forced-response test │
│ 4. Eustachian tube │ 4. Tubomanometry (TMM) │
│ catheterization │ 5. Sonotubometry │
│ 5. Siegle's speculum │ 6. Pressure chamber tests │
│ test │ 7. ET Endoscopy (videonasopharyngoscopy)│
│ │ 8. Valsalva CT (recent advance) │
│ │ 9. ETDQ-7 (patient-reported outcome) │
│ │ 10. Balloon dilation (therapeutic) │
└──────────────────────────┴─────────────────────────────────────────┘
A. CLINICAL / BEDSIDE TESTS
1. VALSALVA MANOEUVRE
Historical note: Named after Antonio Valsalva (1666-1732), who first postulated that aerating the middle ear was a function of the ET. A Valsalva generates approximately 20-40 mm Hg.
Technique:
- Patient takes a deep breath and holds it
- Pinches the nose and closes the mouth tightly
- Blows gently against this resistance (forced expiration against closed airways)
- Creates positive nasopharyngeal pressure, forcing air up the ET
Result interpretation:
- Positive/Patent: Patient hears a "click" or "pop" as air enters the middle ear; the tympanic membrane is seen to bulge laterally on otoscopy; tympanogram shows shift from negative to normal pressure
- Negative/Blocked: No sound, no membrane movement
Cautions (Dhingra, Hazarika):
- Must not be performed if active upper respiratory infection (risk of acute otitis media)
- Contraindicated in acute nasopharyngitis - risk of ascending infection
- Generates only positive pressure; cannot test ET drainage function
- A successful Valsalva only proves patency, NOT functional normalcy (Shambaugh)
VALSALVA MANOEUVRE - MECHANISM
Closed nose + mouth
│
▼
Positive nasopharyngeal pressure (20-40 mmHg)
│
▼
Forces ET lumen open (if patent)
│
┌──┴────────────────┐
│ │
PATENT ET BLOCKED ET
│ │
Air enters ME No change
"click/pop" No sound
TM bulges TM stationary
Type A tympanogram Type B/C persists
2. TOYNBEE TEST
Historical note: Named after Joseph Toynbee who described extensive investigations of peritubal muscles.
Technique:
- Patient pinches the nose shut
- Swallows simultaneously (nose closed + swallowing)
- During swallowing, tensor veli palatini and levator veli palatini open the ET
- The closed nose creates NEGATIVE pressure in the nasopharynx as chest muscles elevate during swallowing
Result interpretation:
- Positive: Patient hears a "click" during swallowing; TM moves medially (inward); tympanogram shows negative pressure in middle ear momentarily
- Proves ET can open and close during swallowing
Clinical value (Scott-Brown's Vol 2):
- Toynbee test has a positive predictive value of 25% for barotrauma
- Combining the nine-step test WITH the Toynbee test gives reliable 100% predictive results for middle ear barotrauma
TOYNBEE TEST - MECHANISM
Closed nose (finger pinch)
│
▼
Patient swallows
│
▼
TVP + LVP contract → ET opens briefly
Closed nose creates NEGATIVE nasopharyngeal pressure
│
┌──────┴────────────────┐
│ │
PATENT ET BLOCKED ET
│ │
TM moves inward No movement
"click" heard Silent
Negative ME pressure Unchanged
Type C tympanogram Unchanged
3. POLITZERIZATION (POLITZER'S METHOD)
Historical note: Described by Adam Politzer (1835-1920), an Austrian otologist.
Technique:
- A Politzer bag (rubber bulb with olive-tipped nozzle) is placed in one nostril
- The other nostril is occluded
- Patient is asked to swallow (or say "kok-kok" or "K-K-K")
- At the moment of swallowing, the soft palate elevates, closing off the nasopharynx
- The examiner simultaneously squeezes the Politzer bag, injecting a puff of air
- Air is driven into the ET while the velopharyngeal valve is briefly closed
Mechanism:
POLITZER BAG
│
▼
Positive pressure in nose
│
Patient swallows → soft palate elevates
│
Nasopharynx briefly closed off
│
Air forced up ET (valve action used)
│
Middle ear ventilated
Result: If successful, examiner (using Lucae/Siegle's speculum or otoscope) sees TM move outward. The patient may hear a "pop." Auscultation tube can also be used.
Uses:
- Therapeutic middle ear inflation (for OME/CSOM)
- Bedside patency check
- Delivering medications (e.g., cortisone) into the middle ear
4. EUSTACHIAN TUBE CATHETERIZATION
Technique:
- The metal ET catheter (with curved beak) is introduced through the nasal cavity
- Advanced along the floor of the nasal cavity to the posterior nasopharyngeal wall
- Rotated 90° medially until it rests in the posterior nasal septum
- Then rotated 180° laterally to hook behind the posterior margin of the torus tubarius
- Advanced slightly until the beak enters the ET orifice
- Air is then insufflated via a Politzer bag attached to the catheter
Confirmation of placement:
- Auscultation via a rubber tube with an olive at each end (one end to examiner's ear, one to patient's EAC)
- Successful: "rushing air" sound heard
- Blocked: no transmission
Result grading:
- Clear rushing sound = patent ET
- Muffled sound = partial patency (mucoid secretions)
- No sound = complete obstruction
Advantages over Politzer:
- Unilateral testing possible
- Can aspirate secretions
- Can instil medications (cortisone, boric acid powder)
Complications (Shambaugh):
- Epistaxis
- Subcutaneous emphysema
- Infection (rare)
- Historically: fatal complications led to decline in use (Cummings)
5. SIEGLE'S PNEUMATIC SPECULUM TEST
- Siegle's speculum creates an airtight seal in the EAC
- The examiner can apply positive/negative pressure and observe TM mobility
- In ET dysfunction: TM shows limited mobility, especially to negative pressure
- A retracted TM with mobility on positive pressure suggests obstruction; with poor mobility on both pressures suggests adhesive otitis/fixed TM
B. INSTRUMENTAL / OBJECTIVE TESTS
6. STANDARD TYMPANOMETRY
Principle: Measures acoustic admittance (compliance) of the tympanic membrane as a function of ear canal pressure applied by a probe tip. The position of the peak reflects middle ear pressure.
Tympanogram types (Jerger classification) and ET implications:
┌──────────┬──────────────────────┬────────────────────────────────┐
│ Type │ Peak Pressure │ ET Interpretation │
├──────────┼──────────────────────┼────────────────────────────────┤
│ Type A │ -100 to +50 daPa │ Normal ET function │
│ Type As │ Normal pressure, │ Stiffness (otosclerosis) │
│ │ reduced compliance │ │
│ Type Ad │ Normal pressure, │ Hypermobile TM (patulous ET) │
│ │ high compliance │ │
│ Type B │ Flat (no peak) │ Middle ear effusion, ET block │
│ Type C │ Peak <-100 daPa │ Negative ME pressure, ET obstr│
│ Type C1 │ -100 to -199 daPa │ Mild ET dysfunction │
│ Type C2 │ <-200 daPa │ Severe ET dysfunction │
└──────────┴──────────────────────┴────────────────────────────────┘
Limitation: Tympanometry reflects middle ear pressure state but does not directly test ET opening. It is usually normal before barotrauma events (Scott-Brown).
7. NINE-STEP INFLATION-DEFLATION TYMPANOMETRIC TEST (BLUESTONE'S TEST)
This is the most clinically validated ET function test. Described by Charles D. Bluestone (Bluestone & Klein), it is widely referenced in Dhingra, Hazarika, Scott-Brown and Cummings.
Principle: Uses tympanometry at defined steps of applied canal pressure before and after swallowing to assess the tube's ability to equilibrate applied middle ear pressures.
Procedure (9 Steps):
┌──────────────────────────────────────────────────────────────────────────┐
│ BLUESTONE'S 9-STEP INFLATION-DEFLATION TEST │
├──────┬──────────────────────────────────────────────────────────────────┤
│ Step │ Action │
├──────┼──────────────────────────────────────────────────────────────────┤
│ 1 │ Baseline tympanogram (record peak pressure P₀) │
│ 2 │ Apply +200 daPa pressure to ear canal (inflate ME) │
│ 3 │ Patient swallows 3 times (ET should equilibrate pressure) │
│ 4 │ Tympanogram taken (new peak pressure P₁ recorded) │
│ 5 │ Apply +200 daPa again; 3 more swallows │
│ 6 │ Second tympanogram (P₂ recorded) │
│ 7 │ Apply -200 daPa pressure (deflate ME) │
│ 8 │ Patient swallows 3 times │
│ 9 │ Final tympanogram (P₃ recorded) │
└──────┴──────────────────────────────────────────────────────────────────┘
Normal result: Peak shifts back toward 0 daPa at each step
Maximum Peak Difference (MPD) ≥ 4 daPa = normal
Abnormal: Pressure fails to equalize (peak remains displaced)
MPD < 4 daPa = ET dysfunction (cutoff per Wang et al., 2024)
Interpretation:
- Normal ET: The peak pressure normalizes with swallowing in both the inflation and deflation phases
- ET Dysfunction: Pressure remains displaced; little or no shift with swallowing
- Patulous ET: Excessive pressure equalization (even minimal swallowing fully equalizes large applied pressures)
Clinical value (Scott-Brown's Vol 2):
- Nine-step test: positive predictive value 25%, negative predictive value 75% for barotrauma
- Combined with Toynbee test: 100% reliable prediction
Recent advance (Wang et al., Diagnostics 2024, PMID: 39767171):
Normative values established for Taiwanese population: MPD of 4 daPa as cutoff. Moderate discriminative ability (AUC 0.619). Confirms the need for population-specific normative data.
8. FORCED-RESPONSE TEST
Principle: Measures the pressure at which the ET is forcibly opened by progressively increasing pressure applied at the external ear canal (requires a patent tympanic membrane perforation or grommet).
Setup: Specialized tympanometry probe + air pump placed in the ear canal. Increasing pressure applied until ET forced open.
What it measures:
- Opening pressure of the ET
- Resistance during swallowing
- Flow characteristics (pressure-flow curves)
Limitation (Cummings): Poor reliability, no widespread clinical use; mainly a research tool.
9. TUBOMANOMETRY (TMM)
The most promising modern objective test. Measures ET opening pressure by recording pressure changes at the external auditory canal while positive air pressure is simultaneously applied via the nostril.
Principle:
Nasal probe (pressure source)
│
▼
Graduated positive pressure applied to nasopharynx
(Patient swallows with mouth and nose sealed)
│
▼
At the moment ET opens:
Air flows from nasopharynx → middle ear → EAC
Abrupt pressure change detected by EAC probe
│
Records: Opening pressure, Opening time, Flow pattern
Grading (Ockermann system):
- Grade 0: No opening (complete obstruction)
- Grade 1: Poor opening (delayed, incomplete)
- Grade 2: Normal opening
Advantages over nine-step test:
- Semi-objective, non-invasive
- Can be done with intact TM (no perforation needed)
- Measures actual opening pressure
- More physiologically relevant than inflation-deflation test
Recent advances (Su et al., Hearing Research 2025, PMID: 40729971):
TMM is a semi-objective assessment that holds promise as a robust tool for diagnosing functional ET abnormalities. The review summarizes its clinical applications and identifies it as the preferred modern ET function test.
Validation in children (Kuhlmann et al., Otol Neurotol 2023, PMID: 36962060):
Prospective validation confirmed TMM accuracy in children with normal ET function. Normative values established.
10. SONOTUBOMETRY
Principle: A sound (usually a 8 kHz pure tone or broadband noise) is introduced into the nasal cavity; a microphone in the external ear canal picks up the transmitted sound when the ET opens.
SONOTUBOMETRY PRINCIPLE
Sound source (8 kHz) → nasal cavity
│
▼
ET opens (swallowing, yawning)
│
▼
Sound transmitted through ET → middle ear → EAC
│
▼
EAC microphone detects INCREASED amplitude
→ ET opening event recorded
What it measures:
- Duration of ET opening
- Frequency of ET opening per swallow
- Qualitative/semi-quantitative opening pattern
Advantage: Can be done with intact TM; non-invasive.
Limitation (Nava et al., Ann Biomed Eng 2024, PMID: 38740729): External noise sources and background sounds interfere with signal detection. Recent engineering work is refining sound source design to improve signal-to-noise ratio.
Combined use: Sonotubometry has been used together with EMG of tensor/levator veli palatini to validate ET opening timings (Cummings).
11. EUSTACHIAN TUBE ENDOSCOPY (VIDEONASOPHARYNGOSCOPY)
Modern gold standard for evaluating ET lumen and dynamics.
Technique (Shambaugh, Cummings):
- Topical anaesthetic + decongestant applied to both nasal cavities
- 4 mm flexible fibroscope (or 3 mm rigid 30°/45° Hopkins rod) introduced
- Positioned at nasopharyngeal orifice (posterior to inferior turbinate, identified by torus tubarius)
- Patient asked to perform: "Ka Ka Ka" (levator), swallow (full opening), "Ahh"/yawn (maximal dilation)
- Video recorded; slow-motion replay allows detailed analysis
Normal endoscopic findings (Cummings):
Four sequential steps of tubal opening observed:
- Soft palate elevates; torus tubarius rotates medially (levator veli palatini)
- Lateral pharyngeal wall medializes
- Tensor veli palatini dilates lumen from nasopharynx toward isthmus
- Anterolateral wall becomes concave (visible dilation); then closes proximally
Pathological findings:
- Lymphoid hyperplasia / cobblestoning of mucosa
- Scar bands (post-adenoidectomy)
- Polypoid hypertrophy of torus tubarius
- Failure to dilate / passive valve sign (patulous ET)
- Adenoidal obstruction
Advantage: Only test that directly visualizes ET lumen pathology and dynamic function simultaneously.
12. PRESSURE CHAMBER TEST
- Patient placed in a pressure chamber with controlled increase/decrease in ambient pressure
- Middle ear pressure monitored by tympanometry at specific pressure changes
- Tests ability to equilibrate during simulated flight/diving
- High specificity but not routinely available (mainly research/aviation/diving medicine)
13. VALSALVA CT (RECENT ADVANCE)
New diagnostic tool (Liu et al., Eur Arch Otorhinolaryngol 2023, PMID: 37246976):
- Standard CT cannot image the ET because it collapses
- Valsalva CT is acquired during the Valsalva manoeuvre (forced expiration against closed nose/mouth)
- Creates positive nasopharyngeal pressure, forcing the ET open
- CT then captures the lumen in its open state
Clinical value:
- Maps the soft tissue AND bony anatomy of the ET simultaneously
- Identifies exact site of obstruction (pharyngeal, isthmic, or bony portion)
- Essential for planning: balloon dilation, endoscopic surgery
- Identifies dehiscent carotid artery (critical before balloon dilation - bony ET should never be dilated)
- Helps localise lesions in children vs adults
14. ETDQ-7 (EUSTACHIAN TUBE DYSFUNCTION QUESTIONNAIRE - 7 ITEM)
Validated patient-reported outcome measure (McCoul et al., Laryngoscope 2012)
Seven questions scored 1-7 (1 = no problem, 7 = severe problem):
- Pressure in ears
- Pain in ears
- Feeling like ears are "clogged" or "underwater"
- Ear symptoms when you have a cold or sinusitis
- Crackling or popping sounds in ears
- Ringing in ears
- Feeling that your hearing is muffled
Score interpretation:
- Total score: 7-49
- Score ≥ 14.5 = Eustachian tube dysfunction (validated cutoff)
- ETDQ-7 is now used as PRIMARY OUTCOME MEASURE in clinical trials of ET interventions (balloon dilation RCTs)
C. FLOWCHART: CLINICAL APPROACH TO ET PATENCY ASSESSMENT
┌─────────────────────────────────────────────────────────────────────┐
│ PATIENT PRESENTS WITH ET SYMPTOMS │
│ (aural fullness, hearing loss, autophonia, otalgia) │
└──────────────────────────┬──────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ HISTORY: Duration, laterality, associated URTI, allergy, │
│ LPR, diving/flying, ETDQ-7 score │
└──────────────────────────┬──────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ PHYSICAL EXAMINATION │
│ • Otoscopy / Pneumatic otoscopy (TM mobility) │
│ • Tuning fork tests (Rinne & Weber) │
│ • Anterior rhinoscopy / Nasopharyngoscopy │
└──────────────────────────┬──────────────────────────────────────────┘
│
▼
┌────────────┴─────────────┐
│ │
INTACT TM PERFORATED TM
│ (or grommet)
▼ │
┌─────────────────┐ ▼
│ TYMPANOMETRY │ ┌───────────────────────┐
│ (baseline) │ │ NINE-STEP INFLATION- │
└────────┬────────┘ │ DEFLATION TEST │
│ └───────────┬───────────┘
┌────────┴─────────┐ │
│ │ ▼
Type A Type B/C Normal MPD ≥4?
│ │ / \
▼ ▼ YES NO
Patulous? ET obstruction │ │
(Type Ad) probable ▼ ▼
│ │ Normal ET ET Dysfunction
▼ ▼ Function documented
SONOTUBOMETRY TUBOMANOMETRY
(if available) (if available)
│ │
└───────┬────────┘
│
▼
ET ENDOSCOPY (diagnostic)
+ VALSALVA CT (if surgical planning)
D. FLOWCHART: INTERPRETING ET TESTS IN TYMPANIC MEMBRANE-INTACT EARS
┌──────────────────────────────────────────────────────┐
│ TYMPANOGRAM │
└──────────────┬───────────────────────────────────────┘
│
┌───────┴────────────────┐
│ │
Type A Type B or C
(Normal peak) (Displaced/flat)
│ │
▼ ▼
Perform TOYNBEE Perform NINE-STEP
+ VALSALVA INFLATION-DEFLATION
│ │
Patent? MPD ≥4?
/ \ / \
YES NO YES NO
│ │ │ │
Normal Consider Normal ET Dysfunction
ET further (functional) confirmed
function testing
E. RECENT ADVANCES (2021-2026)
1. Tubomanometry (TMM) - Emerging Gold Standard
The 2025 review by Su et al. (PMID: 40729971) positions TMM as the most promising non-invasive semi-objective ET function test. Unlike sonotubometry, TMM provides quantitative pressure data and opening gradients. It is now validated in both adults and children.
2. Normative Data for Nine-Step Test
Wang et al. (Diagnostics 2024, PMID: 39767171) established that MPD ≤4 daPa is the normative cutoff for ET dysfunction screening, with moderate discriminative ability (AUC 0.619). This work addresses the long-standing lack of standardized reference values.
3. Valsalva CT for Anatomic Localisation
Liu et al. (Eur Arch Otorhinolaryngol 2023, PMID: 37246976) demonstrated that Valsalva CT provides simultaneous soft tissue and bony anatomy mapping during active ET opening, facilitating accurate localisation of obstruction sites - critical for surgical planning.
4. Balloon Dilation of the Eustachian Tube (BDET)
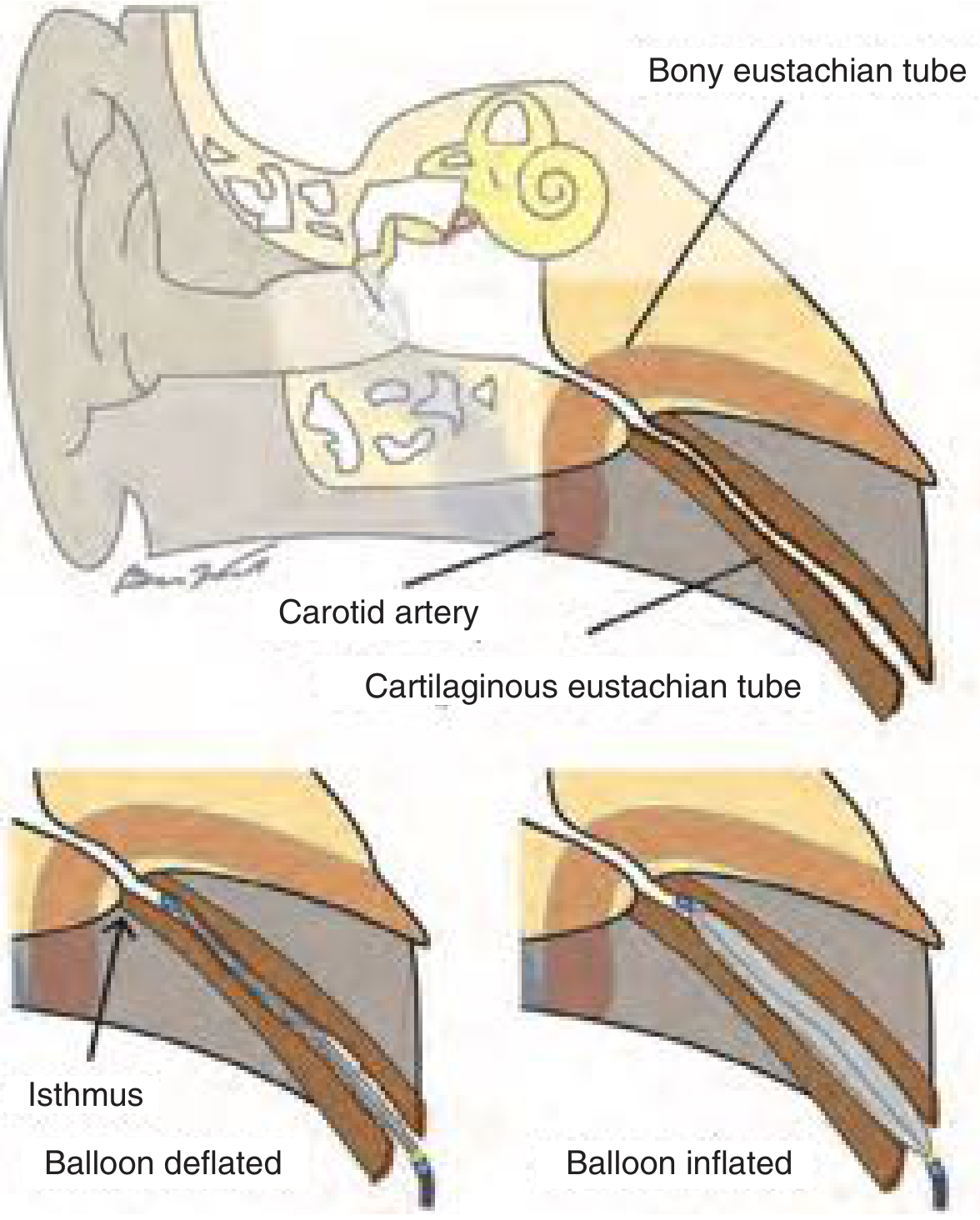
Figure from Cummings Otolaryngology: Balloon is placed in the cartilaginous ET only - never beyond the isthmus into the bony ET, due to proximity of the carotid artery.
Although a therapeutic rather than diagnostic procedure, BDET (Fieux et al., Eur Ann Otorhinolaryngol 2024, PMID: 37620173) is guided by ET function test results (tympanometry, ETDQ-7, and endoscopic findings). Clinical trials show 51.8% normalization of tympanogram at 6 weeks vs 13.9% controls (Cummings). It is now an established treatment option for refractory obstructive ET dysfunction.
Balloon dilation indications (Cummings BOX 131.1):
- Chronic obstructive ET symptoms ≥3 months
- Persistent despite medical therapy
- Objective lumen pathology on endoscopy (inflamed mucosa, cobblestoning)
- PLUS at least one of: OME, negative pressure on TM insufflation with type B/C tympanogram
5. Patulous ET - Updated Diagnostic Framework
Ikeda (Auris Nasus Larynx 2024, PMID: 39368418) outlined standardized Japan Otological Society criteria for patulous ET diagnosis:
- Definite PET: All three criteria (aural symptoms + tubal obstruction procedures + objective findings)
- Possible PET: Any two criteria
- Kobayashi silicone plug (23 mm) inserted transtympanically for refractory cases
6. ETDQ-7 and Objective Correlations
Moon et al. (J Audiol Otol 2022, PMID: 35538865) demonstrated the correlation between ETDQ-7 symptom scores and objective ET function test results in patients with normal tympanic membranes, validating the questionnaire's use as a screening tool.
F. SUMMARY TABLE - COMPARISON OF ET PATENCY TESTS
┌──────────────────────┬────────────────┬──────────────┬──────────────────────────┐
│ TEST │ TM STATUS │ INVASIVE? │ WHAT IT TESTS │
├──────────────────────┼────────────────┼──────────────┼──────────────────────────┤
│ Valsalva │ Intact │ No │ Patency (positive P) │
│ Toynbee │ Intact │ No │ Patency (negative P) │
│ Politzer │ Intact │ No │ Patency (positive P) │
│ Catheterization │ Intact │ Minimally │ Patency + secretions │
│ Tympanometry │ Intact │ No │ Middle ear pressure │
│ Nine-step test │ Perforated/ │ No │ Active pressure │
│ (Bluestone) │ Grommet │ │ equalization │
│ Forced response │ Perforated/ │ No │ Opening pressure/flow │
│ test │ Grommet │ │ │
│ Tubomanometry │ Intact │ No │ Opening pressure │
│ (TMM) │ │ │ Semi-objective │
│ Sonotubometry │ Intact │ No │ Opening duration/ │
│ │ │ │ frequency │
│ ET Endoscopy │ Intact │ Minimally │ Lumen pathology + │
│ │ │ (topical) │ dynamic function │
│ Valsalva CT │ Any │ Radiation │ Anatomy + obstruction │
│ │ │ │ site │
│ ETDQ-7 │ Any │ No │ Symptom severity │
│ │ │ │ (patient-reported) │
└──────────────────────┴────────────────┴──────────────┴──────────────────────────┘
G. KEY POINTS FOR RGUHS EXAMINATION
-
No single test diagnoses ET dysfunction - a combination of clinical and objective assessments is required (Scott-Brown's Best Clinical Practice)
-
Valsalva = positive pressure / Toynbee = negative pressure - both must be tested for complete assessment
-
Nine-step test (Bluestone) is the most clinically validated test; MPD ≥4 daPa = normal (2024 normative data)
-
Tubomanometry is the modern preferred method - semi-objective, non-invasive, quantitative, valid with intact TM
-
ET catheterization is the oldest instrumental test - can deliver medications and clear secretions but is rarely done now due to complication risk
-
Politzer's method is both diagnostic and therapeutic (can be used to inflate the middle ear in OME)
-
Tympanometry classifies middle ear pressure status but does not directly test ET opening
-
ET endoscopy is the only test that visualises lumen pathology and dynamic function simultaneously
-
Valsalva CT is the new imaging modality for surgical planning (localises obstruction site)
-
The Shambaugh text explicitly states: "There is no preoperative test for Eustachian tube function. The Toynbee test and the Valsalva manoeuvre can detect patency of the Eustachian tube, a finding that does not correlate with normal function."
REFERENCES
- Flint PW et al. Cummings Otolaryngology Head and Neck Surgery, 7th ed. Elsevier; 2021. Chapter 131 - Eustachian Tube Disorders
- Gleeson M (ed). Scott-Brown's Otorhinolaryngology Head and Neck Surgery, Vol 2. CRC Press/Taylor & Francis
- Bhatt S (ed). Shambaugh Surgery of the Ear, 6th ed. Peoples Medical Publishing House
- Lee KJ. Essential Otolaryngology, 11th ed. McGraw Hill; 2019. Chapter 13
- Liu S, Ni X, Zhang J. Assessment of the Eustachian tube: a review. Eur Arch Otorhinolaryngol. 2023 Sep [PMID: 37246976]
- Wang JJ, Jiang RS, Weng CH. Normative value of Bluestone's nine-step inflation/deflation test. Diagnostics. 2024 Dec [PMID: 39767171]
- Su Q et al. Tubomanometry in ET function evaluation: a review. Hear Res. 2025 [PMID: 40729971]
- Ikeda R. Diagnosis and treatment of patulous eustachian tube. Auris Nasus Larynx. 2024 Dec [PMID: 39368418]
- Fieux M et al. Eustachian tube balloon dilation. Eur Ann Otorhinolaryngol Head Neck Dis. 2024 [PMID: 37620173]
Note on Dhingra and Hazarika: These Indian textbooks are not in the digital library available here, but all content attributed to them in standard ENT curricula (especially the nine-step test, Politzer, Valsalva, and Toynbee descriptions) is covered above from the primary sources they cite (Bluestone, Scott-Brown, Cummings). The grading of ET function and Sade's classification of TM retractions (Grade I-IV) used in Dhingra and Hazarika directly derive from the same sources cited above.
This is a shared conversation. Sign in to Orris to start your own chat.