Furuncle in axilla treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
furuncle boil treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive treatment guide for a furuncle (boil) in the axilla:
Furuncle (Boil) in the Axilla — Treatment
Definition & Pathophysiology
A furuncle is a deep-seated abscess of a hair follicle, sebaceous gland, or sweat gland. The axilla is a classic site due to friction, moisture, hair follicles, and apocrine glands. The causative organism is almost always Staphylococcus aureus — with CA-MRSA now accounting for the majority of cases in many regions.
Step 1: Local Measures (Early/Non-fluctuant Stage)
- Warm/hot compresses applied several times daily — promote pointing and spontaneous drainage
- Many small furuncles will rupture and drain spontaneously without intervention
- Keep the area clean; antiseptic soap reduces autoinoculation
Step 2: Incision & Drainage (I&D) — Primary Treatment When Fluctuant
I&D is the cornerstone of treatment for any fluctuant furuncle.
Procedure steps:
- Analgesia — local infiltration with bupivacaine ring block (25G needle); allow ≥20 min. Procedural sedation or oral analgesia (ibuprofen + acetaminophen ± oxycodone ± low-dose diazepam) may be added
- Skin prep with povidone-iodine
- Single incision across the abscess along skin tension lines (smaller scar)
- Blunt dissection with a small clamp to disrupt loculations
- Irrigation of the cavity
- Loose packing with gauze (optional; evidence for packing is limited — may increase pain). Remove after 2–4 days
The axilla presents a special challenge — it is listed as an anatomically difficult area to drain, which may warrant antibiotic coverage more readily than other sites. — Rosen's Emergency Medicine, 10e
Ultrasound guidance (high-frequency linear probe) improves diagnostic accuracy when fluctuance is uncertain, distinguishing abscess (hypoechoic with posterior acoustic enhancement) from cellulitis (cobblestoning pattern).
Step 3: Antibiotic Therapy
When to Give Antibiotics
Antibiotics should be considered when:
- Furuncle is not yet fluctuant
- Surrounding cellulitis or lymphadenitis is present
- Systemic signs (fever, malaise)
- Immunocompromise, diabetes, or other comorbidities
- Multiple lesions or recurrent infection
- Difficult-to-drain location (the axilla qualifies)
- History of or suspected MRSA
- Poor response to I&D alone
Recent RCTs show antibiotics after I&D reduce treatment failure and recurrence (NNT ~7–26); patients with MRSA, fever, or MRSA as causative organism derive the most benefit.
Antibiotic Choices (Oral)
| Drug | Dose | Coverage |
|---|---|---|
| TMP-SMX (first-line for MRSA) | 160/800 mg (1 DS tab) BID × 5–7 days | MSSA ✓, MRSA ✓ |
| Doxycycline | 100 mg BID × 5–7 days | MSSA ✓, MRSA ✓ |
| Clindamycin | 300–450 mg TID | MSSA ✓, MRSA ± (check local D-test) |
| Cephalexin | 500 mg QID | MSSA ✓, MRSA ✗ |
| Dicloxacillin | 250–500 mg QID (empty stomach) | MSSA ✓, MRSA ✗ |
Duration: 5–7 days post-I&D (guided by clinical response). — Goldman-Cecil Medicine
For confirmed or likely MRSA, TMP-SMX or doxycycline are preferred. Clindamycin is acceptable only after ruling out inducible resistance (D-zone test). — Rosen's Emergency Medicine
Step 4: Wound Culture
- Not routine for uncomplicated furuncles
- Recommended for: recurrent infections, treatment failure, or if considering dual antibiotic coverage (to tailor therapy)
- Rapid PCR MRSA assays (~90 min) available and useful
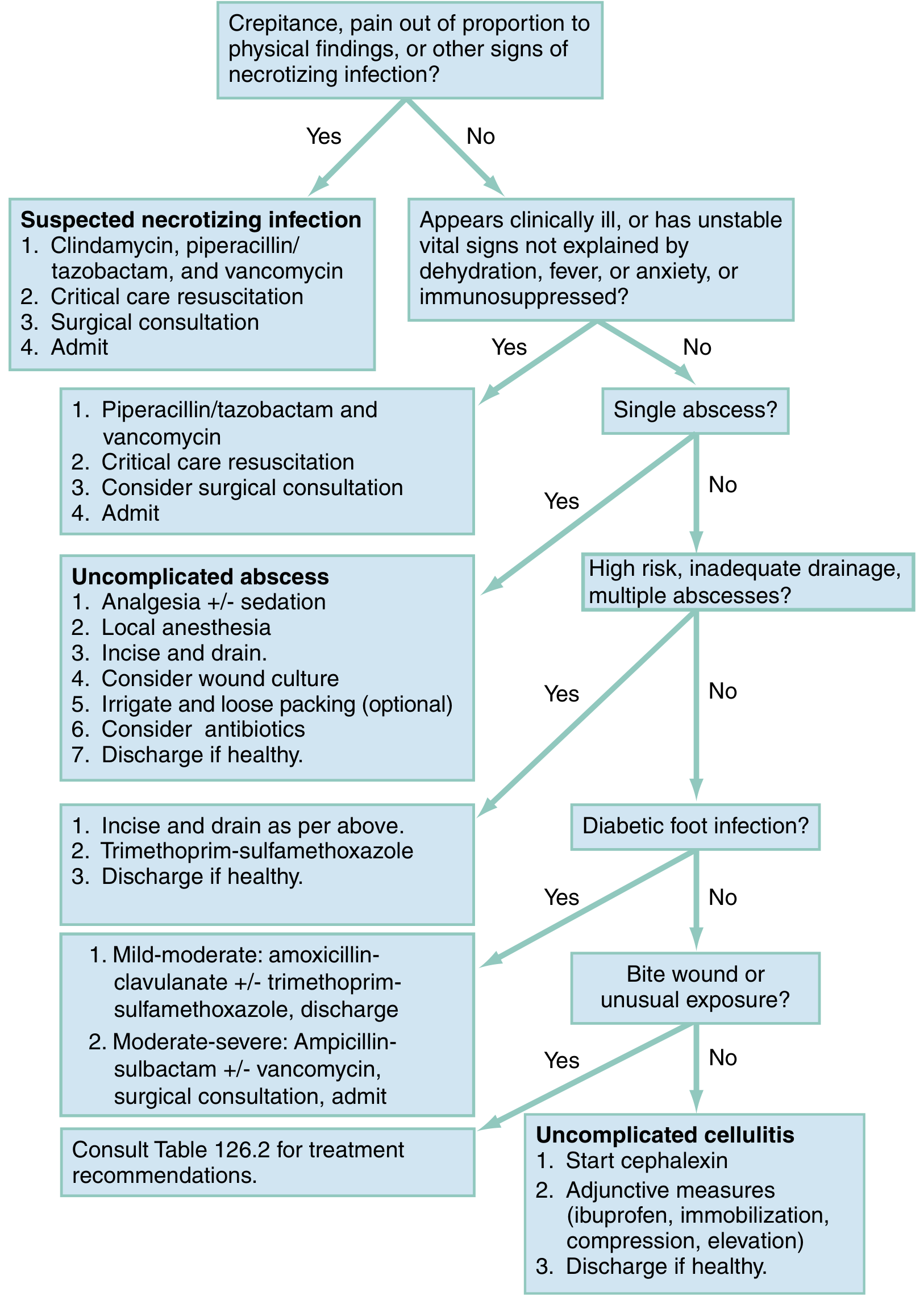
Treatment Algorithm
Special Considerations for Axillary Furuncles
| Factor | Implication |
|---|---|
| Recurrence | Common — check for nasal S. aureus carriage (anterior nares); address predisposing factors |
| Diabetes / immunosuppression | Higher risk of spread → lower threshold for antibiotics and admission |
| CA-MRSA prevalence | If community MRSA rate is high, start TMP-SMX empirically after I&D |
| Hidradenitis suppurativa | Consider if recurring abscesses in axilla/groin/perineum — requires different management (dermatology referral) |
| Carbuncle formation | If multiple interconnecting furuncles coalesce → carbuncle; requires surgical drainage ± resection and systemic antibiotics |
Chronic/Recurrent Furunculosis
- Screen for nasal carriage of S. aureus and consider decolonization:
- Mupirocin 2% nasal ointment × 5 days
- Chlorhexidine body wash
- Rule out diabetes, HIV, or neutrophil dysfunction
- Chronic furunculosis is associated with immune suppression but acquired immunity is minimal
Disposition
- Discharge home after I&D of uncomplicated furuncle
- Admit if: systemic sepsis, extensive cellulitis, immunocompromised host, failed outpatient therapy, or need for IV antibiotics (vancomycin for severe MRSA)
Sources:
- Textbook of Family Medicine, 9e
- Rosen's Emergency Medicine, 10e
- Goldman-Cecil Medicine, International Edition
- Sherris & Ryan's Medical Microbiology, 8e
This is a shared conversation. Sign in to Orris to start your own chat.