Hernia surgery
Reading File
Asking for Preferences
Finding Sources
Searching the Web
hernia types anatomy surgical classification medical student overview 2024
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative surgical textbooks. Let me compose the full answer.
Hernia Surgery: Types & Anatomy (Medical Student Reference)
Definition
A hernia is the protrusion of a viscus (or part of it) through an abnormal opening in the wall of its containing cavity. Most clinically relevant hernias involve abdominal contents protruding through defects in the abdominal wall.
Classification by Reducibility (Exam Favourite)
| State | Definition | Risk |
|---|---|---|
| Reducible | Contents return freely to cavity | Low immediate risk |
| Irreducible / Incarcerated | Cannot be reduced without surgery; sac contents swell | Moderate |
| Strangulated | Incarcerated + blood supply compromised | Surgical emergency - necrosis if not relieved |
Key rule: hernias with a small neck are most likely to strangulate. Direct inguinal hernias (wide neck) rarely strangulate; femoral hernias (narrow rigid ring) strangulate most readily.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1039
Groin Hernias (Most Commonly Tested)
The Inguinal Canal
The inguinal canal is an oblique 4 cm passage through the anterior abdominal wall, running from the deep (internal) inguinal ring to the superficial (external) inguinal ring. It transmits the spermatic cord in males and the round ligament in females.
Walls:
- Anterior: External oblique (EO) aponeurosis + internal oblique (lateral 1/3)
- Posterior: Transversalis fascia + conjoint tendon (medial)
- Roof: Arched fibres of internal oblique and transversus abdominis
- Floor: Inguinal (Poupart) ligament
Hesselbach's Triangle (Inguinal Triangle)
Boundaries:
- Medially: Lateral border of rectus abdominis
- Superolaterally: Inferior epigastric vessels
- Inferiorly: Inguinal ligament
This is the single most important anatomical landmark for the exam.
Laparoscopic view of inguinal hernia defects (Bailey & Love, 28th Ed.):
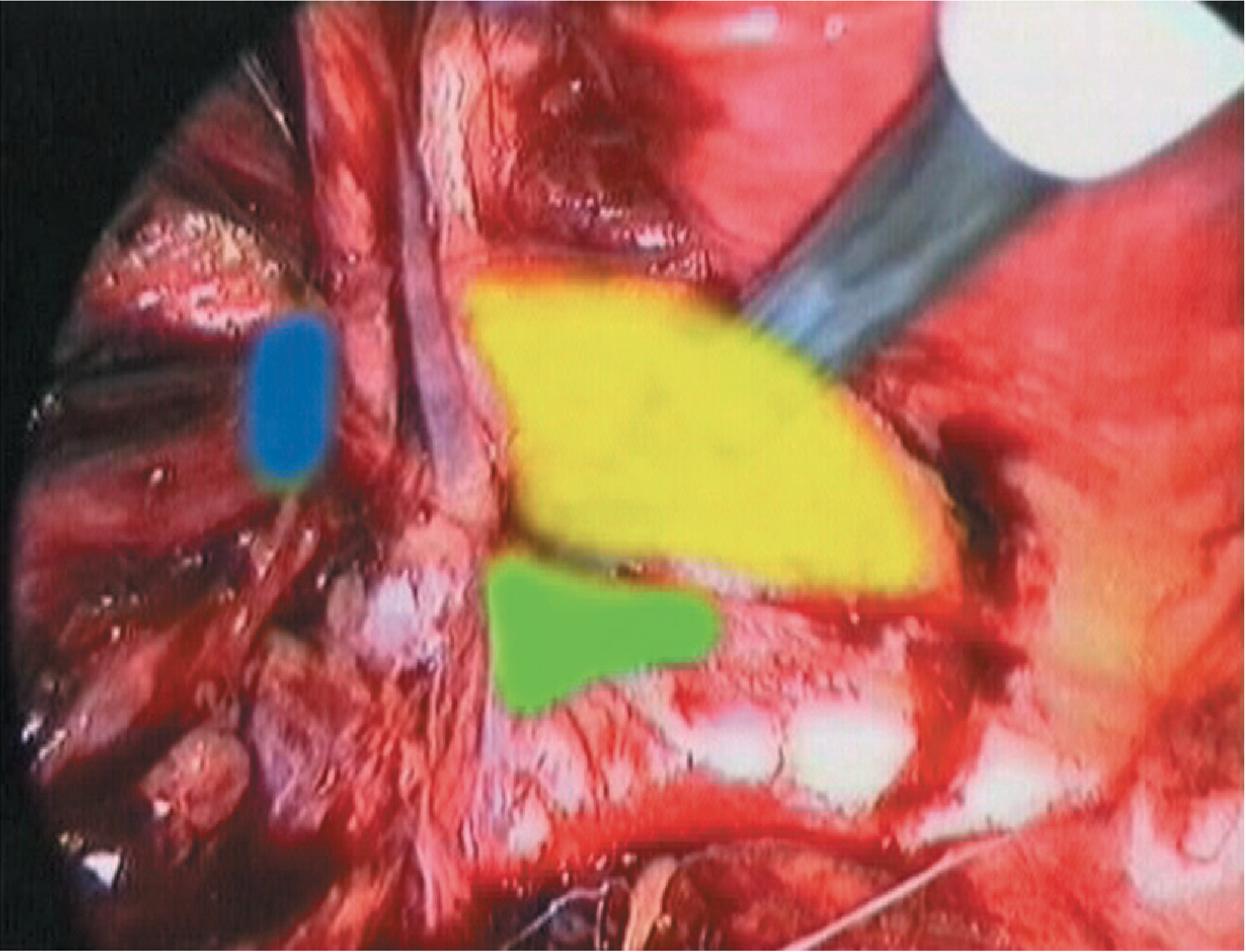
Yellow = Hesselbach's triangle (direct inguinal); Blue = lateral/indirect inguinal; Green = femoral
Inguinal Hernias: Direct vs. Indirect
| Feature | Indirect Inguinal Hernia | Direct Inguinal Hernia |
|---|---|---|
| Origin | Lateral to inferior epigastric vessels | Medial to inferior epigastric vessels, within Hesselbach's triangle |
| Path | Through the deep inguinal ring, along the inguinal canal (oblique) | Directly through abdominal wall (perpendicular) |
| Aetiology | Congenital (patent processus vaginalis) or acquired | Always acquired (transversalis fascia weakness) |
| Sex/Age | Males > females; any age (commonest in children) | Elderly males |
| Sac and cord | Sac is within the spermatic cord (covered by cremasteric fascia) | Sac lies adjacent to cord, not within it |
| Reaches scrotum? | Yes - can become a scrotal hernia | Rarely |
| Strangulation risk | Higher (narrow deep ring) | Low (wide neck) |
| Frequency | Two-thirds of inguinal hernias | One-third |
Lifetime risk of groin hernia: 27-43% in males, 3-6% in females. Over 20 million inguinal hernia repairs performed annually worldwide.
- Sabiston Textbook of Surgery, p. 1680
Femoral Hernia
- Passes below the inguinal ligament through the femoral canal, medial to the femoral vein
- The femoral ring (internal opening) has a sharp-edged lacunar ligament medially - the reason strangulation is so common
- 3% of all groin hernias but carries the highest strangulation risk of all hernias
- Female:male ratio ~10:1 (broader pelvis, larger femoral ring); however, inguinal hernias still outnumber femoral hernias in women
- More common on the right (sigmoid colon "plugs" the left femoral canal)
- THIEME Atlas of Anatomy, p. 236
Clinical trick: Feel below and lateral to the pubic tubercle for a femoral hernia; above and medial for inguinal.
Pantaloon (Saddle-Bag) Hernia
A combined direct + indirect inguinal hernia straddling the inferior epigastric vessels, producing a double-lobulated bulge like pantaloon trousers. Rare.
Ventral (Abdominal Wall) Hernias
| Type | Location | Key Facts |
|---|---|---|
| Umbilical | At the umbilical ring | Most common non-groin hernia; common in infants (usually close spontaneously by age 3-4), adults with ascites/obesity |
| Paraumbilical | Adjacent to (not through) the umbilicus | Adults; does NOT close spontaneously - needs repair |
| Epigastric | Midline above umbilicus, through linea alba | Contain pre-peritoneal fat; often multiple |
| Incisional | At or near a previous surgical scar | Recurrence rate 20-50%; mesh required |
| Spigelian | Lateral to rectus abdominis, through linea semilunaris | Interstitial (intramural) - can be missed on examination |
| Hypogastric | Midline below umbilicus | Rare |
- Yamada's Textbook of Gastroenterology; Fischer's Mastery of Surgery, 8th Ed.
Rare/Special Hernia Types (OSCE Trivia)
| Name | Description |
|---|---|
| Richter's hernia | Only part of the bowel circumference is trapped in the sac - can strangulate without obstruction |
| Maydl's hernia (hernia-en-W) | Two loops of bowel in sac; the segment connecting them (inside the abdomen) strangulates |
| Littre's hernia | Contains Meckel's diverticulum |
| Sliding hernia | Part of the sac wall is formed by a retroperitoneal organ (e.g. caecum, sigmoid, bladder) |
| Obturator hernia | Through obturator foramen; elderly women; Howship-Romberg sign (pain along medial thigh) |
| Lumbar hernia | Through Petit's or Grynfeltt's triangle posteriorly |
| Gluteal/sciatic hernia | Passes through sciatic foramen |
| Internal hernia | Through abnormal opening inside abdominal cavity (e.g. after Roux-en-Y bypass) |
Hiatal Hernia (Diaphragmatic)
| Type | Description |
|---|---|
| Type I - Sliding (95%) | GEJ and fundus slide upward through hiatus; associated with GERD |
| Type II - Rolling/Paraesophageal | Fundus rolls up alongside fixed GEJ; risk of gastric volvulus |
| Type III - Mixed | Both GEJ and fundus herniate |
| Type IV | Other viscera (colon, spleen) also herniate |
Eponyms Summary Table (High-Yield for Exams)
| Eponym | What it is |
|---|---|
| Hesselbach's triangle | Boundary of direct inguinal hernia |
| Poupart's ligament | Inguinal ligament |
| Gimbernat's (lacunar) ligament | Sharp medial boundary of femoral ring - causes strangulation |
| Cooper's ligament | Pectineal ligament - used in McVay repair |
| Corona mortis | Anastomosis of obturator and epigastric vessels - "crown of death" if injured |
Quick Memory Aid
"DELI-M" for Direct vs Indirect:
- Direct = older, Degenerative, Doesn't go to scrotum, Doesn't strangulate much
- Indirect = Innate (congenital), goes Into scrotum, Incarceration risk higher
Strangulation risk ranking (highest to lowest): Femoral > Indirect inguinal > Umbilical > Direct inguinal
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Ch. 64: Inguinal region
- Sabiston Textbook of Surgery, Inguinal Hernia Repair
- Fischer's Mastery of Surgery, 8th Ed. - Ch. 221
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 236
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.