Women with 50 having in ankle side and cracking sound leg and swelling
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
ankle pain swelling women perimenopausal osteoarthritis
I now have enough information to provide a thorough, well-structured response. Let me compile everything.
Ankle-Side Pain, Cracking Sound & Swelling in a 50-Year-Old Woman
This is a very common presentation in women around age 50. The combination of lateral ankle pain + popping/cracking + swelling points to several likely causes, which often overlap.
Most Likely Causes
1. Peroneal Tendon Disorder (Top Suspect)
The peroneal tendons run just behind and below the lateral (outer) malleolus (the bony bump on the outside of your ankle). This is the most fitting explanation for your exact symptoms.
Classic symptoms of Peroneal Longus Tendon Tear/Tendinitis (from Campbell's Operative Orthopaedics 15th Ed 2026):
- Swelling
- Tenderness
- Popping
- Crepitus (cracking/grating) just posterior to the lateral malleolus
- Fluid palpable within the tendon sheath
- Weakness or pain on turning the foot outward (eversion)
This condition primarily affects middle-aged individuals during repetitive activity or those with underlying foot alignment problems. Women at 50 are a classic age group.
2. Ankle Osteoarthritis (OA)
OA of the ankle joint causes:
- Joint stiffness that is worse after rest, then eases with movement
- Crepitus - a grinding or cracking sensation on joint movement (described in Goldman-Cecil Medicine as "a grinding sensation under the examiner's hand during active or passive joint motion")
- Swelling - both soft tissue (synovial fluid) and bony enlargement over time
- Pain that worsens with prolonged activity and toward end of day
At age 50, the drop in estrogen around menopause significantly increases OA risk - cartilage has estrogen receptors and degrades faster after menopause.
3. Lateral Ankle Ligament Laxity / Chronic Instability
Repetitive minor sprains or ligament loosening can cause:
- A clicking/snapping feeling
- Swelling along the outer ankle
- A sense that the ankle "gives way"
Frameworks for Internal Medicine notes: "The presence of crepitus, clicking, or snapping with joint movement commonly occurs as a result of ligamentous stretch."
4. Rheumatoid Arthritis or Gout (Less Likely but Important to Rule Out)
- RA tends to affect joints symmetrically and cause >60 minutes of morning stiffness
- Gout can affect the ankle and causes hot, red, very tender swelling (usually sudden attacks)
- Both need blood tests to distinguish
Red Flag Signs - See a Doctor Urgently If You Have:
- Severe redness, warmth, and rapid swelling (possible infection or gout)
- The ankle "locked" or you cannot bear weight
- Obvious deformity
- Fever with joint swelling
What Your Doctor Will Likely Do
| Step | Details |
|---|---|
| Physical exam | Palpate peroneal tendons, check range of motion, test ankle stability, feel for crepitus |
| X-ray | First test - checks for OA (joint space narrowing, bone spurs), fractures |
| Ultrasound / MRI | Better for soft tissue - shows tendon tears, fluid, ligament damage |
| Blood tests | ESR, CRP, uric acid, RF, anti-CCP to rule out RA/gout |
Self-Care While Awaiting Assessment
- Rest the ankle - reduce activities that cause the cracking/pain
- Ice for 15-20 minutes after activity to reduce swelling
- Elevate the leg when sitting/lying
- NSAIDs (e.g., ibuprofen) if no contraindications - reduce inflammation and pain
- Wear supportive footwear with good ankle support; avoid flat slippers or heels
- Avoid pushing through severe pain
From Campbell's Operative Orthopaedics: Non-operative treatment with "cast or boot immobilization, oral anti-inflammatory medications, and subsequent physical therapy can relieve tendinitis symptoms." An orthotic (shoe insert) or ankle brace for 4-6 months after inflammation resolves is often recommended long-term.
Summary
| Most Likely Diagnosis | Key Feature Matching Your Symptoms |
|---|---|
| Peroneal tendinitis/tear | Lateral ankle, popping, crepitus, swelling - exact match |
| Ankle osteoarthritis | Age 50, cracking, swelling, post-menopausal risk |
| Ligament laxity/instability | Clicking, outer ankle, swelling |
Please see an orthopedic surgeon, sports medicine doctor, or rheumatologist for a proper examination. An X-ray and ultrasound of the ankle will likely be ordered to confirm the diagnosis. The good news is that most of these conditions respond well to non-surgical treatment.
In one sided legs only
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
This is very helpful - now I have a clinical image showing both DVT and Baker's cyst presentations. Here is the focused answer:
One-Sided (Unilateral) Leg Swelling - Why It Matters
Unilateral swelling is a key clinical clue. According to Rosen's Emergency Medicine, "unilateral leg swelling" is rated as a +4 (strongest) sign for Deep Vein Thrombosis (DVT). This changes the priority of diagnoses significantly.
The Most Important Causes for ONE-Sided Leg
⚠️ 1. Deep Vein Thrombosis (DVT) - Must Rule Out First
A blood clot forming in the deep veins of the calf or thigh. This is a medical emergency because clots can travel to the lungs (pulmonary embolism).
Why it fits a 50-year-old woman:
- Older age increases risk (hypercoagulability + venous stasis)
- Estrogen (including HRT, if she is taking it) is a documented risk factor
- Women around menopause are at increased risk
Signs of DVT:
- Swelling of the entire leg or calf on ONE side
- Pitting edema (pressing on the skin leaves a dent) confined to that leg
- Aching or heaviness in the calf or leg
- The leg may feel warm and look slightly red
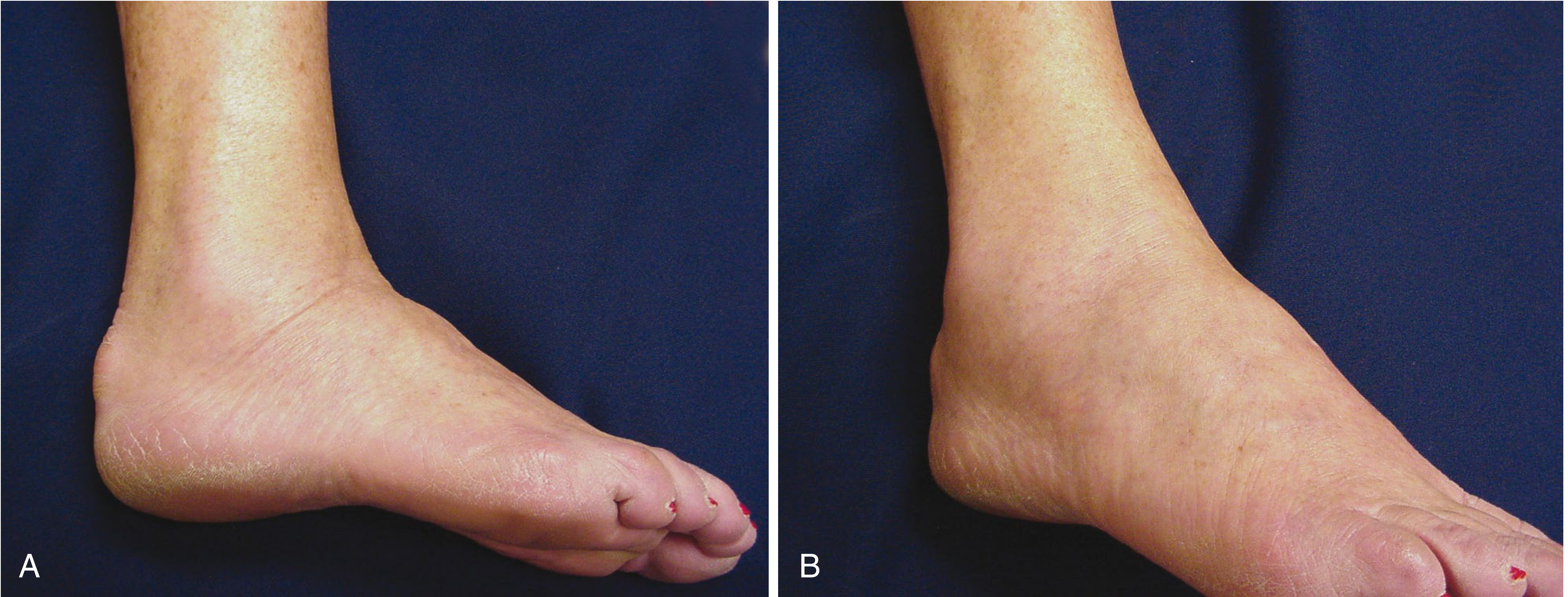
Below is a clinical photo from Rosen's Emergency Medicine showing one-sided leg swelling from DVT (left) vs. ruptured Baker's cyst (right) - both look very similar:

Wells Score for DVT (from Rosen's Emergency Medicine) - each feature scores +1:
| Feature | Present? |
|---|---|
| Entire leg swollen | Check |
| Calf swelling >3 cm larger than the other side | Check if present |
| Pitting edema only on the swollen leg | Check if present |
| Tenderness along the deep vein distribution | Check if present |
| Active cancer | - |
| Recent bed rest or surgery | - |
- Score ≥ 2 = High probability of DVT → needs urgent ultrasound
- Score < 2 = Low probability, but still needs D-dimer blood test
2. Peroneal Tendinitis / Tendon Tear (Lateral Ankle Side)
As discussed before, the peroneal tendons sit on the outer (lateral) side of the ankle. A tear or inflammation here causes:
- Swelling specifically at the outer ankle side
- Popping and crepitus just behind the lateral malleolus
- Pain on turning foot outward
- This is naturally one-sided - affects whichever foot is overused or injured
This is still the best explanation for the cracking sound at the ankle side specifically.
3. Ruptured Baker's Cyst
A fluid-filled cyst behind the knee (popliteal fossa) that ruptures can cause:
- Sudden one-sided calf swelling and pain
- Can look identical to DVT on examination (see image above)
- Diagnosed by ultrasound
4. Venous Insufficiency / Varicose Veins (One Side)
- Damaged valves in leg veins cause blood pooling on the affected side
- Swelling worse at end of day and after standing
- Often visible varicose veins
- No cracking sound - this fits less well
5. Cellulitis
- Bacterial skin infection causing red, hot, swollen one leg
- No cracking sound - fits less
Putting It Together for This Patient
| Symptom | What It Suggests |
|---|---|
| One-sided swelling | DVT, peroneal tendon issue, venous insufficiency |
| Lateral ankle-side location | Peroneal tendon problem (most specific) |
| Cracking/popping sound | Peroneal tendinitis/tear (crepitus) |
| Age 50, female | DVT risk elevated; OA possible |
| No mention of redness/heat | Less likely cellulitis or gout |
⚠️ URGENT: What to Do Now
DVT must be excluded first because it can be life-threatening.
-
See a doctor TODAY or go to Emergency if you also have:
- The whole leg is swollen (not just ankle)
- The calf is significantly larger than the other side
- Leg feels warm or looks red/discolored
- Shortness of breath or chest pain (this means clot may have reached lungs - call emergency services immediately)
-
If swelling is confined to just the ankle side with the cracking, it is more likely the peroneal tendon, and an urgent (but not emergency) orthopedic or sports medicine appointment is appropriate.
Tests your doctor will order:
-
Doppler ultrasound of the leg veins - rules out DVT quickly
-
D-dimer blood test - if DVT is suspected
-
X-ray of ankle - checks for bone/joint problems
-
MRI or ultrasound of ankle tendons - if tendon tear is suspected
-
Rosen's Emergency Medicine, DVT chapter
-
Campbell's Operative Orthopaedics 15th Ed 2026, Peroneal Tendon Disorders
Treatment and popping sound ankle pain heat up and swelling by stand
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching PubMed
peroneal tendinopathy ankle treatment conservative
I have all the information needed. Here is the complete, focused treatment guide.
Treatment for Ankle Popping + Heat + Swelling Worse on Standing
The fact that swelling heats up and gets worse with standing tells us there is active inflammation with fluid pooling under gravity. This is classic for peroneal tenosynovitis (inflamed tendon sheath on the outer ankle) - the most fitting diagnosis for all your symptoms combined.
Here is the clinical appearance - this is exactly what peroneal tenosynovitis looks like:
Treatment - Step by Step
PHASE 1: Immediate (First 1-2 Weeks) - Reduce Inflammation
The PRICE Method:
| Step | What to Do | Why |
|---|---|---|
| P - Protect | Wear an ankle brace or support bandage | Stops further tendon stress |
| R - Rest | Avoid prolonged standing, walking long distances | Reduces irritation of inflamed tendon |
| I - Ice | Ice pack wrapped in cloth for 15-20 minutes, 3-4 times daily | Reduces heat and swelling |
| C - Compression | Wear a firm compression bandage or ankle sleeve | Reduces fluid buildup that worsens on standing |
| E - Elevate | Keep leg raised above heart level when sitting/lying | Fluid drains away from ankle by gravity - directly counteracts the standing-worsening |
Key for you: Because swelling worsens on standing, elevation when resting is especially important. Every hour you stand without a break, the fluid pools further. Try to rest with the leg up for 20-30 minutes between periods of standing.
PHASE 2: Anti-Inflammatory Medication
Over-the-counter options:
| Medicine | Dose (adult) | Duration |
|---|---|---|
| Ibuprofen (Brufen, Advil) | 400 mg, 3 times daily with food | Up to 5-7 days |
| Naproxen (Naprosyn) | 250-500 mg, twice daily with food | Up to 5-7 days |
| Diclofenac gel (topical) | Apply to ankle 3-4 times daily | Can use longer than tablets |
- Take with food to protect the stomach
- Avoid if you have kidney disease, stomach ulcers, or are on blood thinners
- Topical diclofenac gel is safer and works well for localized ankle inflammation
From Campbell's Operative Orthopaedics: "Cast or boot immobilization, oral anti-inflammatory medications, and subsequent physical therapy can relieve tendinitis symptoms."
PHASE 3: Doctor-Prescribed Treatments (If No Improvement in 2-4 Weeks)
| Treatment | Details |
|---|---|
| Boot/Cast immobilization | A removable walking boot takes all stress off the tendon for 3-6 weeks |
| Ankle brace (orthosis) | Used for 4-6 months after inflammation settles to prevent recurrence |
| Physiotherapy | Strengthening exercises for peroneal muscles, stretching of calf/Achilles, balance training |
| Corticosteroid injection | Doctor injects steroid around the tendon sheath to rapidly reduce severe inflammation (used cautiously - not directly into the tendon) |
| Ultrasound-guided therapy | Physiotherapist uses therapeutic ultrasound to reduce deep inflammation |
PHASE 4: If All Else Fails - Surgery
According to Campbell's Operative Orthopaedics 15th Ed 2026:
"For patients who do not respond to nonoperative treatment, tenosynovectomy with repair and stabilization as needed is indicated."
This involves surgically cleaning the inflamed tendon sheath and repairing any tears. This is rarely needed - most cases resolve with conservative treatment.
Exercises You Can Start Now (Gentle Phase)
Do these only when not in the acute hot/swollen phase - wait until heat settles:
- Ankle circles - Sit down, lift foot, rotate ankle clockwise and anticlockwise x 10 each way
- Towel calf stretch - Sit on floor, loop a towel around the ball of the foot, gently pull toes toward you, hold 30 seconds x 3 sets
- Ankle alphabet - Trace the alphabet in the air with your big toe to restore range of motion
- Resistance band eversion - Gently turn foot outward against a light resistance band to strengthen peroneal muscles
What Makes It WORSE - Avoid These
- Standing on hard floors without support for long periods
- Flat shoes and slippers (no arch support)
- High heels (increase tendon stress)
- Walking on uneven ground
- Ignoring it and pushing through severe pain
Footwear Advice (Very Important)
- Wear shoes with good lateral ankle support and a slight heel (1-2 cm)
- Use insoles/orthotics to correct foot alignment - this is critical for long-term benefit
- Avoid completely flat footwear
Warning Signs - See a Doctor Urgently If:
-
The heat and redness spreads up the leg (could be cellulitis/infection)
-
You develop a fever with the swelling
-
The swelling becomes very hard and the whole leg swells (DVT risk - go to emergency)
-
You cannot bear weight at all on the leg
-
Campbell's Operative Orthopaedics 15th Ed 2026, Peroneal Tendon Disorders
Cause of it
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I have rich textbook content and a detailed diagram. Here is the complete answer on causes.
Causes of Ankle-Side Popping + Heat + Swelling in a 50-Year-Old Woman
There are two main underlying mechanisms happening at the same time in this patient - a tendon/structural cause (producing the popping and lateral pain) and joint/cartilage degeneration (producing heat and swelling). Here is a full breakdown:
CAUSE 1: Peroneal Tenosynovitis / Tendon Tear
What is it?
The two peroneal tendons (peroneus longus and brevis) run in a groove behind the outer ankle bone (lateral malleolus). They are held in place by a band of tissue called the superior peroneal retinaculum. When these tendons become inflamed, irritated, or partially torn, the result is exactly the symptoms described.
Why does it happen - the causes:
| Cause | Explanation |
|---|---|
| Overuse / repetitive standing | Long hours of standing, walking on hard floors - the tendons are under continuous load and eventually become irritated. Swelling worsens with standing because fluid accumulates in the inflamed tendon sheath under gravity. |
| Abnormal foot alignment | A high-arched foot (cavus) or foot that rolls outward places extra stress on the outer tendons. Flat feet can also alter the pulling direction of these tendons. This is the #1 underlying mechanical cause. |
| Previous ankle sprain | Even an old sprain that "healed" can stretch or damage the retinaculum, causing the tendons to slip and pop over the bone with movement - producing the snapping/popping sound. |
| Age-related tendon change | After age 40-50, tendons lose water content and elasticity. They become stiffer, more brittle, and more prone to small tears and inflammation with the same level of activity that was fine in younger years. |
| Wrong footwear | Flat shoes, worn-out soles, or high heels change the force distribution on the outer ankle tendons, accelerating wear. |
| Sudden increase in activity | A sudden increase in walking, exercise, or standing (e.g., new job, travel, household work) can overload tendons that were not conditioned for it. |
| Bony variants | An enlarged peroneal tubercle (a small bone bump on the heel bone) or an accessory bone called os peroneum can physically impinge the peroneal tendon, causing friction, inflammation, and popping. |
CAUSE 2: Ankle Osteoarthritis (OA) - Why it Happens at Age 50
This diagram from Robbins Pathologic Basis of Disease shows exactly how OA develops inside the joint:
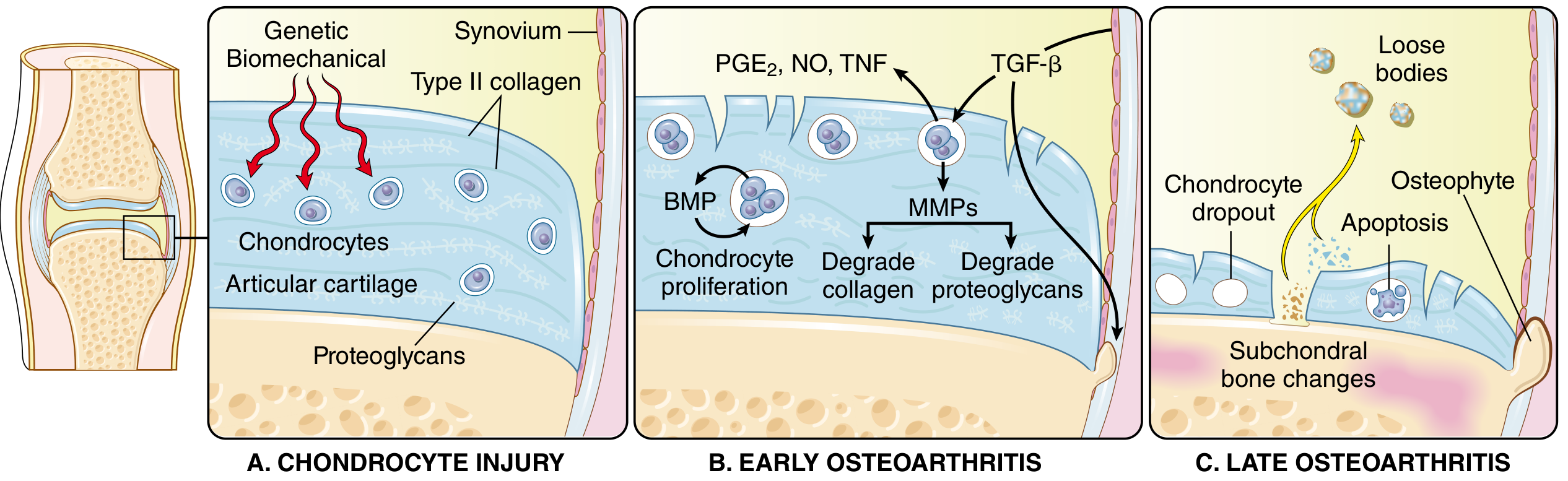
The biological process:
- Chondrocyte injury - Cartilage cells (chondrocytes) are damaged by mechanical stress, genetics, or aging
- Enzyme release - Damaged cells release destructive enzymes (MMPs - matrix metalloproteinases) that break down the cartilage's collagen and proteoglycan framework
- More degradation than repair - In younger people, repair keeps up. After 50, degradation wins
- Cartilage thins and cracks - The smooth surface becomes rough and pitted - this roughness is what generates the cracking/grinding sound
- Synovial inflammation - The joint lining (synovium) becomes irritated by loose cartilage fragments, producing fluid (effusion), heat, and swelling
- Bone spurs (osteophytes) form at joint edges, causing further pain and restriction
Why age 50 is the peak onset:
From Robbins Pathologic Basis of Disease:
"The prevalence of OA increases exponentially beyond 50 years of age, and about 40% of people older than 70 years are affected."
Why women specifically are at higher risk:
| Factor | How It Contributes |
|---|---|
| Menopause / falling estrogen | Estrogen normally protects cartilage. As estrogen drops around age 50, cartilage degrades faster. Women have a steep rise in OA after menopause. |
| Wider pelvis / Q-angle | Women's hip-to-knee alignment puts different mechanical forces on lower leg joints compared to men |
| Lower muscle mass | Less muscle bulk around the ankle means less shock absorption, more stress transferred to cartilage and tendons |
| Weight gain around menopause | Extra body weight multiplies the load on ankle joints with every step (every 1 kg of body weight = ~3-4 kg of force on the ankle while walking) |
| Ligament laxity | Hormonal changes increase ligament looseness, making joints less stable and more prone to repetitive micro-injury |
CAUSE 3: Why Swelling Gets Worse When Standing (The Gravity Effect)
This is a separate but important cause of the symptom worsening on standing:
- The ankle is the lowest point of the body when upright
- Inflamed tissues produce excess fluid (exudate)
- Gravity pulls this fluid down into the ankle and foot when standing
- The longer you stand, the more fluid accumulates - swelling grows progressively
- When you lie down or elevate the leg, fluid drains back up - swelling reduces
- This gravity-dependent swelling on top of tendon inflammation makes the condition feel much worse after a day on your feet
CAUSE 4: The Popping Sound Specifically - 3 Mechanisms
| Mechanism | How It Produces Sound |
|---|---|
| Tendon snapping | Inflamed or displaced peroneal tendon snaps back and forth over the lateral malleolus bone with ankle movement - produces a distinct popping or snapping |
| Gas bubble in joint fluid | Nitrogen gas dissolved in joint fluid forms and pops when the joint is moved under negative pressure (same as "cracking knuckles") |
| Rough cartilage surfaces | Degenerated, roughened cartilage surfaces grind against each other - produces crepitus (a grinding crackle rather than a single pop) |
Summary - Why All This Happened Together
Age 50 + Falling estrogen
↓
Tendon elasticity ↓ + Cartilage protection ↓
↓
Overuse / prolonged standing / wrong shoes
↓
Peroneal tendon irritation + Ankle joint wear
↓
Inflammation → heat + synovial fluid → swelling
↓
Gravity pulls fluid down → worse on standing
↓
Tendon snapping over bone → popping sound
- Robbins Pathologic Basis of Disease, Chapter 26 - Osteoarthritis
- Campbell's Operative Orthopaedics 15th Ed 2026 - Peroneal Tendon Disorders
Treatment
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Excellent - I have very thorough, evidence-based content. Here is the complete treatment guide.
Complete Treatment Plan
Based on authoritative guidelines from Miller's Review of Orthopaedics (AAOS Evidence-Based Guidelines) and Goldman-Cecil Medicine, here is the full, structured treatment from least to most intensive.
STAGE 1: Home Treatment (Start Today)
The PRICE Protocol
| Step | Action | How Long |
|---|---|---|
| Protect | Ankle support bandage or brace when standing/walking | Always when weight-bearing |
| Rest | Reduce prolonged standing; sit every 30-45 min | Ongoing |
| Ice | Ice pack (wrapped in cloth) on outer ankle 15-20 min | 3-4 times daily |
| Compress | Firm elastic compression bandage or ankle sleeve | During the day |
| Elevate | Prop leg above heart level when resting | Every rest break |
Key rule: Ice in the acute hot/swollen phase. After 3-4 days when heat reduces, you may use gentle warmth (warm water soak) before exercises to loosen the joint.
STAGE 2: Medications
Over-the-Counter (No Prescription Needed)
| Medicine | Dose | Notes |
|---|---|---|
| Ibuprofen (Brufen, Advil) | 400 mg, 3x daily with food | Maximum 5-7 days continuously |
| Naproxen (Naprosyn, Aleve) | 500 mg, twice daily with food | Longer lasting than ibuprofen |
| Diclofenac gel (Voltaren topical) | Apply to ankle 3-4x daily | Preferred - works locally, safer for stomach/kidneys |
| Paracetamol (Acetaminophen) | 500-1000 mg, 3-4x daily | Safe for longer use; good for background pain |
According to AAOS Evidence-Based Guidelines (Miller's Review of Orthopaedics):
- Topical NSAIDs - Strongly Recommended
- Oral NSAIDs - Strongly Recommended
- Oral Acetaminophen - Strongly Recommended
- Oral opioids/narcotics - NOT Recommended
Avoid oral NSAIDs if you have stomach ulcers, kidney problems, or take blood thinners. Use topical gel instead.
STAGE 3: Physical Therapy (Most Important Long-Term Treatment)
Exercise is the single most effective long-term treatment. From Goldman-Cecil Medicine:
"Physical therapy appears to be better than standard glucocorticoid injections for relieving pain and preserving function."
Phase A - Acute Phase (First 1-2 weeks, when hot and swollen)
Only gentle, pain-free movements:
- Ankle circles - Sitting down, lift foot, rotate 10x each direction
- Toe flexing - Curl and extend toes slowly x 10 reps
- Heel raises (seated) - Lift heels off floor while seated x 10
Phase B - Sub-Acute Phase (After swelling reduces)
| Exercise | How To Do It | Reps |
|---|---|---|
| Calf stretch | Stand facing wall, step affected foot back, keep heel flat, lean forward | Hold 30 sec x 3 |
| Towel stretch | Sit on floor, loop towel around ball of foot, gently pull toes toward you | Hold 30 sec x 3 |
| Resistance band eversion | Sit, wrap band around foot, push foot outward against resistance | 15 reps x 3 sets |
| Single leg balance | Stand on affected leg only, hold 30 seconds - builds stability | 3 sets daily |
| Heel-to-toe walking | Walk in a straight line placing heel then toe deliberately | 10 lengths |
| Wobble board | Stand on a balance board - trains ankle stability | 5 min daily |
Evidence-Based Exercise Types (from Goldman-Cecil Medicine):
| Type | Examples | Benefit |
|---|---|---|
| Strengthening | Resistance bands, body weight squats | Supports the joint, reduces tendon stress |
| Aerobic (low-impact) | Swimming, cycling, walking | Reduces inflammation, controls weight |
| Neuromuscular/balance | Single leg stand, wobble board | Prevents re-injury, restores ankle stability |
| Water-based (hydrotherapy) | Aqua aerobics, pool walking | Low-impact, reduces load on inflamed joint |
| Tai chi / yoga | Gentle flow movements | Improves balance, flexibility, pain perception |
STAGE 4: Doctor-Prescribed Treatments
Orthotic Devices
| Device | Purpose |
|---|---|
| Custom insoles (orthotics) | Correct foot alignment - reduces abnormal force on peroneal tendons |
| Ankle brace / support | Used for 4-6 months after inflammation settles |
| Walking boot (CAM boot) | For severe cases - rests the tendon completely for 3-6 weeks |
| Walking cane | Reduces load on the affected ankle by 20-30% |
AAOS Guidelines: Brace treatment and walking aids - Moderately Recommended
Injections (Given by Doctor)
| Injection | Use | Notes |
|---|---|---|
| Corticosteroid (e.g., triamcinolone) | Rapid relief of severe inflammation | Short-term benefit (weeks); not repeated more than 3x/year |
| Hyaluronic acid (viscosupplementation) | Lubricates the ankle joint | Moderate evidence; useful when steroids fail |
From Goldman-Cecil Medicine: "Intraarticular corticosteroids for short-term relief - Recommended. Viscosupplements - at most very modest benefit."
Weight Management
From Goldman-Cecil Medicine:
"If BMI >25 or waist >80 cm in women, counsel about weight loss through both diet and exercise. Aim for 5-10% body weight reduction."
Every 1 kg lost = 3-4 kg less force on your ankle with every step.
STAGE 5: Surgical Treatment (Last Resort)
Only considered when all conservative treatment has failed for 6+ months.
| Surgery | What It Does | When Used |
|---|---|---|
| Tenosynovectomy | Removes inflamed tendon sheath tissue, repairs tears | Failed conservative peroneal tendinitis |
| Ankle arthroscopy | Keyhole surgery to clean joint debris, remove bone spurs | Moderate OA not responding to treatment |
| Ankle fusion (arthrodesis) | Fuses the joint bones together permanently - eliminates pain | End-stage severe OA |
| Total ankle replacement | Replaces ankle joint with prosthesis | End-stage OA in active patients |
From Goldman-Cecil Medicine:
"Referral to an orthopedic surgeon should be considered when joint pain disrupts normal sleep, severely reduces walking distance, markedly restricts daily activities, or significantly reduces quality of life after all conservative options have failed."
STAGE 6: Lifestyle Changes (Ongoing)
| Change | Why It Helps |
|---|---|
| Footwear with arch support | Reduces abnormal forces on peroneal tendons |
| Anti-fatigue mats when standing | Reduces impact on ankle for those who stand at work |
| Take standing breaks every 30-45 min | Prevents fluid pooling that worsens swelling |
| Avoid flat/worn-out shoes | Flat shoes increase tendon strain |
| Maintain healthy weight | Every kg lost directly reduces ankle load |
| Swimming or cycling instead of running | Same fitness, far less ankle impact |
Treatment Timeline Summary
Week 1-2: PRICE + Ice + Topical anti-inflammatory gel
Week 2-4: Add oral NSAIDs + gentle exercises + ankle support
Month 1-3: Physiotherapy (strengthening + balance training)
Month 3-6: Ankle brace/orthotics + continue exercises + weight management
If no improvement after 6 months → Doctor assessment for injection or surgery
Quick Reference: What to Do When Symptoms Flare
| Symptom | Action |
|---|---|
| Ankle gets hot after standing | Elevate leg + ice 15 min immediately |
| Popping sound with movement | Gentle ankle circles; avoid forced movement |
| Morning stiffness | Warm foot soak before walking; gentle range-of-motion exercises |
| Swelling at end of day | Compression stocking during the day; elevate overnight |
| Sudden severe pain/swelling | See a doctor urgently - rule out DVT or tendon rupture |
- Miller's Review of Orthopaedics 9th Ed - AAOS Evidence-Based Guidelines for OA
- Goldman-Cecil Medicine - Osteoarthritis Management
- Campbell's Operative Orthopaedics 15th Ed 2026 - Peroneal Tendon Treatment
Uri
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.