Descending tract of spinal cord
Reading File
Finding Sources
Searching Images
descending tracts spinal cord diagram
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Descending Tracts of the Spinal Cord
Descending tracts carry motor commands from the cerebral cortex and brainstem down to lower motor neurons (LMNs) in the spinal cord. They are organized into two major systems: the Lateral Motor System and the Medial Motor System.
Overview Diagram
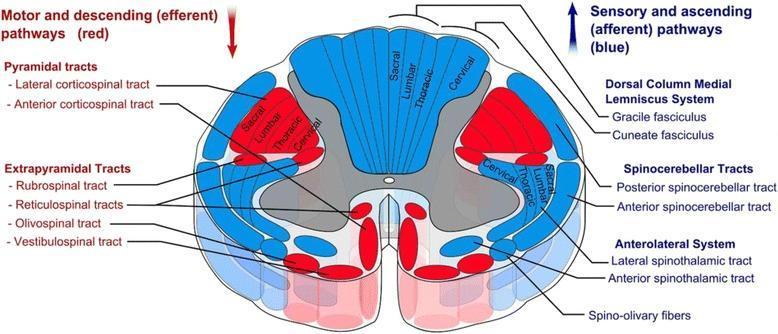
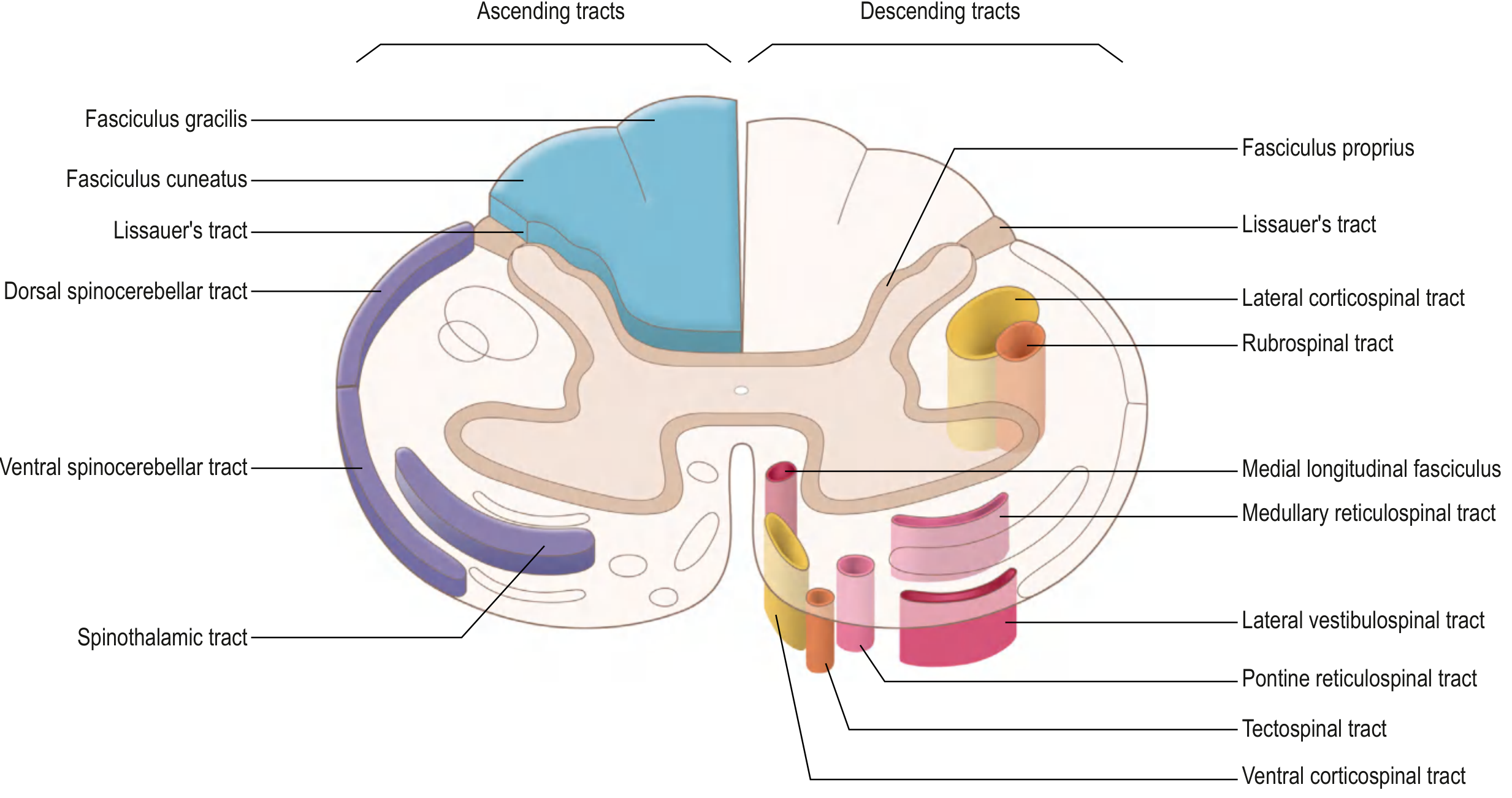
I. Lateral Motor System
Tracts located in the lateral column of the white matter; synapse on LMNs in the lateral anterior horn. Controls distal limb (fine voluntary) movements.
1. Lateral Corticospinal Tract (LCST)
The most clinically important descending tract.
| Feature | Detail |
|---|---|
| Origin | Primary motor cortex (Betz cells, layer V) |
| Course | Corona radiata → posterior limb of internal capsule → crus cerebri (midbrain) → anterior pons (small bundles) → pyramid (medulla) |
| Decussation | Pyramidal decussation at the cervicomedullary junction (~85–90% of fibers) |
| Location in cord | Lateral funiculus (lateral white matter) |
| Termination | Entire cord; predominantly cervical & lumbosacral enlargements — synapses on LMNs in lateral anterior horn |
| Function | Voluntary movement of contralateral limbs |
2. Rubrospinal Tract
| Feature | Detail |
|---|---|
| Origin | Red nucleus (magnocellular division), midbrain tegmentum |
| Decussation | Ventral tegmental decussation in midbrain |
| Location in cord | Lateral column, just anterior to LCST |
| Termination | Cervical cord only — synapse on interneurons in anterior horn |
| Function | Facilitates flexor muscles, inhibits extensor muscles of the upper limb; contralateral control |
In humans, the rubrospinal tract is rudimentary; the lateral corticospinal tract dominates.
II. Medial Motor System
Tracts located in the anterior/medial column; project bilaterally onto interneurons. Controls axial and proximal muscles (posture, balance, gait, head/neck orientation).
3. Anterior (Ventral) Corticospinal Tract
| Feature | Detail |
|---|---|
| Origin | Motor cortex (fibers that did NOT decussate at the pyramidal decussation — ~10–15%) |
| Location | Medial anterior column, ipsilateral |
| Termination | Upper thoracic cord; projects bilaterally to LMNs in medial anterior horn |
| Function | Voluntary control of axial (trunk) muscles |
4. Tectospinal Tract
| Feature | Detail |
|---|---|
| Origin | Superior colliculus, dorsal midbrain |
| Decussation | Dorsal tegmental decussation (immediately after leaving nucleus) |
| Location | Anterior column, near anterior median fissure |
| Termination | Cervical cord only — synapse on interneurons in anterior horn |
| Function | Reflex postural movements in response to visual stimuli (orienting head/neck toward visual targets) |
5. Vestibulospinal Tract (two divisions)
| Division | Origin | Decussation | Course | Termination | Function |
|---|---|---|---|---|---|
| Lateral VST | Lateral vestibular nucleus (Deiters') | None (ipsilateral) | Entire cord | Anterior horn interneurons | Facilitates extensor/antigravity muscles; inhibits flexors → maintains upright posture |
| Medial VST | Medial vestibular nucleus | Bilateral | Cervical–thoracic only | Anterior horn interneurons | Reflex head/neck stabilization |
Input: Vestibular nuclei receive signals from the inner ear (semicircular canals, otolith organs) and the cerebellum.
6. Reticulospinal Tract (two divisions)
| Division | Origin | Course | Function |
|---|---|---|---|
| Pontine (Medial) RST | Pontine reticular formation | Ipsilateral, entire cord, anterior column | Facilitates extensor tone (anti-gravity) |
| Medullary (Lateral) RST | Medullary reticular formation | Ipsilateral, entire cord, lateral column | Facilitates flexor tone; regulates voluntary movement, reflex activity, and autonomic outflow |
Summary Table
| Tract | System | Origin | Decussation | Column | Termination | Function |
|---|---|---|---|---|---|---|
| Lateral corticospinal | Lateral | Motor cortex | Pyramidal decussation (cervicomedullary) | Lateral | Entire cord | Contralateral limb movements |
| Rubrospinal | Lateral | Red nucleus (midbrain) | Ventral tegmental (midbrain) | Lateral | Cervical only | Contralateral flexion of upper limb |
| Anterior corticospinal | Medial | Motor cortex | Bilateral at cord level | Anterior | Upper thoracic | Bilateral axial/trunk control |
| Tectospinal | Medial | Superior colliculus | Dorsal tegmental (midbrain) | Anterior | Cervical only | Visual reflexes → head/neck orientation |
| Lateral vestibulospinal | Medial | Lateral vestibular nucleus | None (ipsilateral) | Anterior | Entire cord | Extensor muscle facilitation, balance |
| Medial vestibulospinal | Medial | Medial vestibular nucleus | Bilateral | Anterior | Cervical–thoracic | Head/neck stabilization |
| Pontine reticulospinal | Medial | Pontine reticular formation | Ipsilateral | Anterior | Entire cord | Extensor facilitation, gait |
| Medullary reticulospinal | Medial | Medullary reticular formation | Ipsilateral | Lateral | Entire cord | Flexor facilitation, autonomic outflow |
Key Clinical Points
- UMN lesion (above LMN) → spasticity, hyperreflexia, Babinski sign, weakness (not flaccid paralysis) — because medial motor system tracts are often spared or injured to varying degrees
- Lateral corticospinal tract lesion (e.g., hemisection = Brown-Séquard) → ipsilateral spastic paresis (because LCST already crossed at medulla)
- Anterior cord syndrome → bilateral motor loss (LCST) + pain/temp loss (spinothalamic), with preserved proprioception (posterior columns intact)
- The pyramid at the medulla = only the corticospinal fibers; "pyramidal" = corticospinal; "extrapyramidal" = all other descending tracts (rubro-, reticulo-, vestibulo-, tectospinal)
Sources: Gray's Anatomy for Students (Elsevier), Neuroanatomy through Clinical Cases 3rd Ed., Harrison's Principles of Internal Medicine 21st Ed.
Neurogenic bladder
Reading File
Finding Sources
Searching Images
neurogenic bladder classification types diagram
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative urology textbooks. Let me compile the full answer.
Neurogenic Bladder
Neurogenic bladder (NGB) is lower urinary tract (LUT) dysfunction caused by neurological disease or injury affecting the neural control of the bladder and/or urethral sphincter.
Neural Control of the Bladder (Normal Physiology)
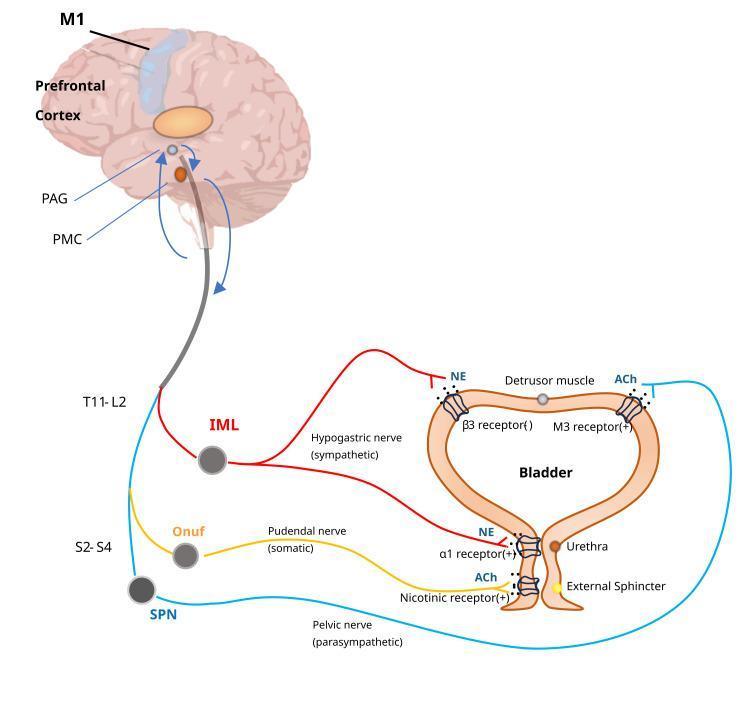
Three neural pathways govern micturition:
| Pathway | Origin | Nerve | Neurotransmitter | Effect |
|---|---|---|---|---|
| Sympathetic | T11–L2 (IML) | Hypogastric nerve | NE (norepinephrine) | Detrusor relaxation (β3); bladder neck contraction (α1) → storage |
| Parasympathetic | S2–S4 (SPN) | Pelvic nerve | ACh (M3 receptors) | Detrusor contraction → voiding |
| Somatic | S2–S4 (Onuf's nucleus) | Pudendal nerve | ACh (nicotinic) | External urethral sphincter contraction → continence |
Higher centers:
- Pontine Micturition Center (PMC) — coordinates synergistic relaxation of sphincter + detrusor contraction
- Periaqueductal gray (PAG) — relay between bladder afferents and cortex
- Prefrontal cortex / M1 — voluntary inhibition and initiation of voiding
Bladder storage pressure should remain < 40 cmH₂O to prevent upper tract damage (hydroureteronephrosis, loss of renal function).
Etiology / Causes
| Category | Examples |
|---|---|
| Spinal cord injury (SCI) | Trauma, most common cause |
| Congenital | Spina bifida (myelomeningocele) — most common congenital cause |
| Demyelinating | Multiple sclerosis |
| Neurodegenerative | Parkinson's disease, MSA |
| Cerebrovascular | Stroke, traumatic brain injury |
| Peripheral neuropathy | Diabetes mellitus (diabetic cystopathy) |
| Infectious | Varicella zoster, herpes |
| Tumors | Brain/spinal cord tumors |
| Iatrogenic | Radical pelvic surgery, radiation |
Classification by Level of Lesion
1. Suprapontine Lesions (above the brainstem)
(Stroke, TBI, brain tumors, Parkinson's disease, MS affecting cortex)
- Loss of voluntary inhibition of the voiding reflex
- Detrusor–sphincter synergy preserved (PMC intact)
- Result: Detrusor overactivity (DO) → urgency, frequency, urge incontinence
- Sphincter coordination is maintained → no dangerous high pressures
2. Suprasacral Spinal Cord Lesions (between brainstem and S2)
(SCI, MS, transverse myelitis)
- PMC and cortex are disconnected from sacral cord
- Bladder acts autonomously → Neurogenic Detrusor Overactivity (NDO)
- Detrusor–Sphincter Dyssynergia (DSD): simultaneous detrusor contraction + EUS contraction → dangerous high intravesical pressures → risk to upper tracts
- Lesions above T6: risk of Autonomic Dysreflexia (massive sympathetic discharge triggered by bladder distension — BP can spike to 200+ mmHg, with bradycardia, headache, diaphoresis)
3. Sacral / Infrasacral Lesions (S2–S4 or below)
(Cauda equina injury, spina bifida, pelvic surgery, peripheral neuropathy)
- Damage to the parasympathetic outflow (sacral parasympathetic nucleus)
- Result: Detrusor Areflexia (acontractile bladder) + flaccid external sphincter
- Overflow incontinence; large PVR volumes
- Low pressure storage — upper tracts generally safer
UMN vs. LMN Bladder (Functional Classification)
| Feature | UMN Bladder (Suprasacral) | LMN Bladder (Sacral/Infrasacral) |
|---|---|---|
| Detrusor | Overactive / hyperreflexic | Areflexic / flaccid |
| Sphincter | Spastic (DSD) | Flaccid |
| Skeletal muscle below lesion | Spastic | Flaccid |
| Residual urine | Variable (high if DSD) | High |
| Upper tract risk | High (if DSD/high pressure) | Lower |
| Sensation | Absent / abnormal | Absent / abnormal |
Hald-Bradley Classification (neurotopographic):
- Supraspinal → Suprasacral spinal → Infrasacral → Peripheral autonomic neuropathy → Muscular lesion
Key Urodynamic Findings
Assessment requires urodynamics (UDS) — correlates symptoms with pathophysiology:
| Parameter | Significance |
|---|---|
| Bladder compliance | Low compliance = dangerous high storage pressures |
| DLPP (Detrusor Leak Point Pressure) | > 40 cmH₂O = upper tract at risk |
| Detrusor Overactivity (DO) | Involuntary contractions during filling |
| DSD (Detrusor-Sphincter Dyssynergia) | EMG activity increases during detrusor contraction |
| Post-void residual (PVR) | Reflects emptying efficiency |
Lesion level → urodynamic finding:
- Above brainstem → DO (synergic)
- Between brainstem and sacrum → DO + DSD ± autonomic dysreflexia (if ≥ T6)
- Sacral lesion → detrusor areflexia
Assessment
History: Urinary symptoms (storage + voiding), neurological diagnosis, bowel function, sexual function, mobility, hand function, medications, UTI history
Physical exam: BP (for autonomic dysreflexia), abdominal exam, genital exam, rectal exam (anal tone), focused neurological exam (perianal sensation, bulbocavernosus reflex, lower limb tone)
Investigations:
- Urinalysis + culture (note: asymptomatic bacteriuria should NOT be treated)
- Serum creatinine + GFR
- Upper tract imaging (renal USS or CT urogram) — every 6–12 months in SCI, yearly in transverse myelitis
- Voiding diary, PVR measurement, uroflowmetry
- Urodynamics — recommended before surgical treatment; videourodynamics preferred in high-risk patients (SCI, spina bifida)
Management
Goals:
- Protect upper urinary tracts (keep storage pressure < 40 cmH₂O)
- Achieve social continence
- Prevent UTI, calculi, and skin breakdown
- Maintain quality of life
A. Behavioral / Conservative
- Timed voiding / habit retraining — useful with cognitive deficits
- Pelvic floor exercises / PFPT — shown effective in MS-related DO
- Fluid management, caffeine reduction
B. Bladder Emptying (Voiding Dysfunction)
- Clean Intermittent Catheterization (CIC) — gold standard; first-line for acontractile/high-PVR bladder; typically every 4–6 hours
- Indwelling catheter (urethral or suprapubic) — when CIC not feasible
C. Pharmacotherapy
| Drug | Indication | Mechanism |
|---|---|---|
| Antimuscarinics (oxybutynin, tolterodine, solifenacin, trospium, darifenacin, fesoterodine) | NDO (1st-line) | Block M2/M3 muscarinic receptors → detrusor relaxation |
| β3-agonist (mirabegron) | NDO (alternative/add-on) | Stimulates β3 receptors → detrusor relaxation |
| Desmopressin | Nocturnal polyuria / nocturnal DO | Reduces urine output; caution: hyponatremia (monitor Na⁺) |
| α-blockers (tamsulosin) | Bladder outlet resistance / DSD | Relax smooth sphincter |
| Onabotulinumtoxin A (Botox) | NDO failing anticholinergics | Blocks ACh release (SNAP-25 cleavage); also reduces C-fiber afferent input |
Botox dosing: 200–300 units intradetrusor injection → reduces incontinence episodes, increases capacity; may increase PVR requiring CIC.
D. Neuromodulation
- Sacral Neuromodulation (SNM) — stimulation of S3 sacral nerve root
- Percutaneous Tibial Nerve Stimulation (PTNS) — for OAB/DO
- Intrathecal baclofen — reduces DSD/spasticity
E. Surgical Options for DSD / Outlet Obstruction
- Sphincterotomy — incision of external urethral sphincter → reduces intravesical pressure and autonomic dysreflexia; complications: bleeding, erectile dysfunction, failure
- Botox into sphincter — alternative to surgical sphincterotomy (injections at 3, 6, 9, 12 o'clock)
- Urethral stenting
F. Reconstructive Surgery (when above measures fail)
- Bladder augmentation (enterocystoplasty) — most effective for improving storage; complications: metabolic acidosis, mucus, UTI, bladder stones, malignancy
- Mitrofanoff procedure (appendicovesicostomy) — catheterizable stoma for patients unable to catheterize urethrally
- Continent urinary diversion (Indiana pouch, Kock pouch)
- Incontinent diversion (ileal conduit)
Complications of Neurogenic Bladder
| Complication | Mechanism |
|---|---|
| Recurrent UTI / urosepsis | Stasis, catheter colonization |
| Bladder calculi | Stasis + catheter |
| Upper tract deterioration (hydronephrosis, renal failure) | Chronic high-pressure storage |
| Vesicoureteral reflux | High intravesical pressure |
| Autonomic dysreflexia | Bladder overdistension triggering massive sympathetic response (lesion ≥ T6) |
| Decubitus ulcers | Incontinence + immobility |
| Bladder malignancy | Chronic irritation, especially with augmented bladders |
Special Populations
- Spina bifida/myelomeningocele: Early urodynamic monitoring is crucial; proactive CIC + antimuscarinics; consider augmentation if high pressures persist
- Multiple sclerosis: Highly variable; lesion level changes over time; SNM beneficial; avoid antimuscarinics if impaired emptying
- Parkinson's disease: Predominantly DO, but impaired emptying also occurs; caution with antimuscarinics (worsen cognition)
- Diabetes mellitus (diabetic cystopathy): Sensory loss first → impaired awareness of filling → large-capacity, poorly contractile bladder → CIC
Sources: Smith & Tanagho's General Urology 19th Ed., Campbell-Walsh-Wein Urology, Mulholland & Greenfield's Surgery 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.