Brachial plexus with clinical anatomy according to bdc
Brachial Plexus - Clinical Anatomy (BDC Style)
Note: B.D. Chaurasia's Human Anatomy is not in the library, but the content below is compiled from Gray's Anatomy for Students, Neuroanatomy through Clinical Cases (3rd ed.), and S. Das Manual of Clinical Surgery - all of which present brachial plexus anatomy in the same systematic style as BDC.
Overview
- R = Roots
- T = Trunks
- D = Divisions
- C = Cords
- B = Branches
Diagram of the Brachial Plexus

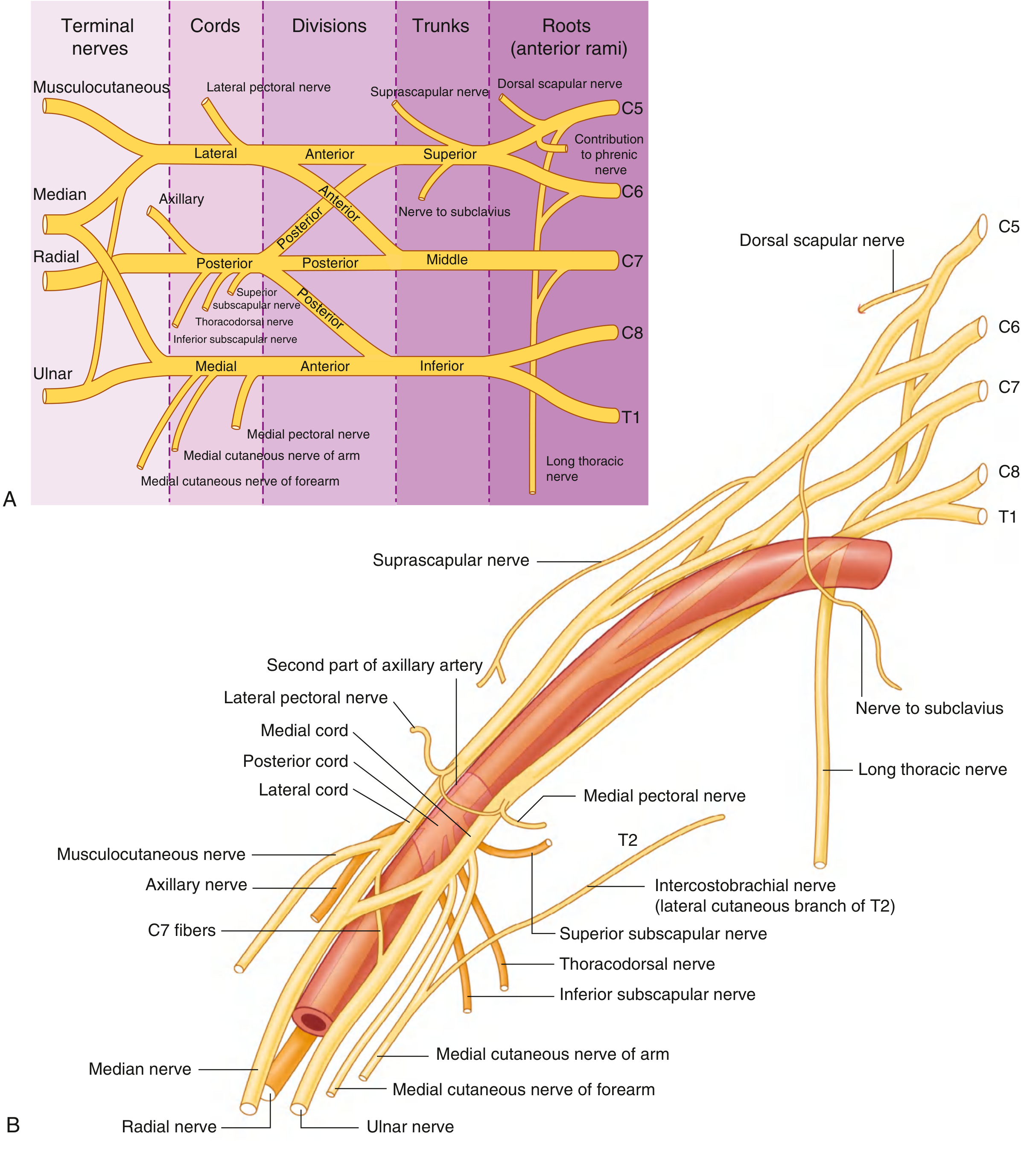
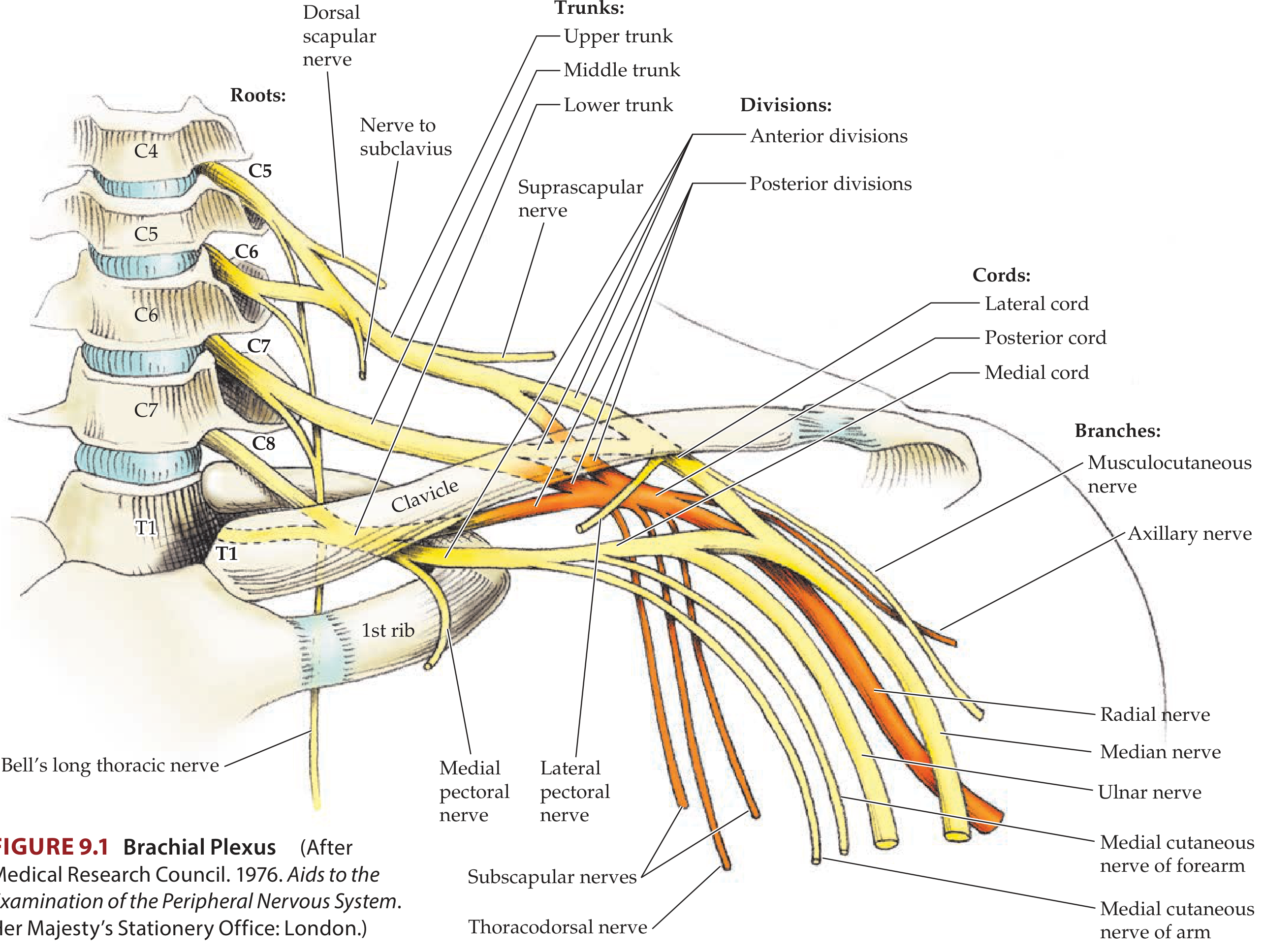
1. ROOTS (Anterior Rami)
- C5, C6, C7, C8, T1 form the roots (anterior rami)
- The roots receive gray rami communicantes from the sympathetic trunk (postganglionic sympathetic fibers)
- The roots pass between the anterior scalene and middle scalene muscles
- They lie superior and posterior to the subclavian artery in the posterior triangle of the neck
Branches from Roots:
| Nerve | Root | Supplies |
|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major, rhomboid minor |
| Long thoracic nerve (Bell's nerve) | C5, C6, C7 | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm (small contribution) |
2. TRUNKS
| Trunk | Formation | Position |
|---|---|---|
| Superior (upper) trunk | C5 + C6 | Superior position |
| Middle trunk | C7 alone | Middle position |
| Inferior (lower) trunk | C8 + T1 | Lies on rib I, posterior to subclavian artery |
Branches from Trunks:
| Nerve | Origin | Supplies |
|---|---|---|
| Suprascapular nerve | Superior trunk (C5, C6) | Supraspinatus, infraspinatus |
| Nerve to subclavius | Superior trunk (C5, C6) | Subclavius |
The trunks cross the base of the posterior triangle and are visible there along with dorsal scapular, long thoracic, nerve to subclavius, and suprascapular nerves.
3. DIVISIONS
- No peripheral nerves originate directly from the divisions
- Anterior divisions supply the anterior (flexor) compartments
- Posterior divisions supply the posterior (extensor) compartments
4. CORDS
| Cord | Formation | Position | Roots |
|---|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks | Lateral to axillary artery | C5, C6, C7 |
| Medial cord | Anterior division of inferior trunk | Medial to axillary artery | C8, T1 |
| Posterior cord | All three posterior divisions | Posterior to axillary artery | C5 to T1 |
5. BRANCHES (Terminal and Collateral)
Branches of the Lateral Cord:
| Nerve | Spinal Segments | Function |
|---|---|---|
| Lateral pectoral nerve | C5-C7 | Pectoralis major |
| Musculocutaneous nerve | C5-C7 | Biceps, brachialis, coracobrachialis (BBC); sensory: lateral forearm |
| Lateral root of median nerve | C5-C7 | Contributes to median nerve |
Branches of the Medial Cord:
| Nerve | Spinal Segments | Function |
|---|---|---|
| Medial pectoral nerve | C8, T1 | Pectoralis major and minor |
| Medial cutaneous nerve of arm | C8, T1 | Sensory: medial arm |
| Medial cutaneous nerve of forearm | C8, T1 | Sensory: medial forearm |
| Medial root of median nerve | C8, T1 | Contributes to median nerve |
| Ulnar nerve | C8, T1 | All intrinsic hand muscles except thenar + lateral 2 lumbricals; sensory: medial 1.5 fingers |
The musculocutaneous nerve, lateral root of median nerve, median nerve, medial root of median nerve, and ulnar nerve form an "M" over the third part of the axillary artery - a key landmark to identify plexus components in the axilla.
Branches of the Posterior Cord:
| Nerve | Spinal Segments | Function |
|---|---|---|
| Superior subscapular nerve | C5, C6 | Subscapularis |
| Thoracodorsal nerve | C6, C7, C8 | Latissimus dorsi |
| Inferior subscapular nerve | C5, C6 | Subscapularis, teres major |
| Axillary nerve | C5, C6 | Deltoid, teres minor; sensory: skin over deltoid (superior lateral cutaneous nerve of arm); exits axilla via quadrangular space |
| Radial nerve (largest branch) | C5-T1 | All posterior compartment muscles of arm and forearm; sensory: posterior arm, forearm, dorsolateral hand; exits via triangular interval |
Terminal Nerve Summary:
| Nerve | Cord | Roots |
|---|---|---|
| Musculocutaneous | Lateral | C5-C7 |
| Median | Lateral + Medial | C5-T1 |
| Ulnar | Medial | C8-T1 |
| Axillary | Posterior | C5-C6 |
| Radial | Posterior | C5-T1 |
6. MEDIAN NERVE - Special Note
- All forearm flexors except FCU and medial half of FDP
- Three thenar muscles (APB, FPB, opponens pollicis)
- Lateral two lumbricals
- Sensory: palmar surface of lateral 3.5 digits + lateral palm
7. CLINICAL ANATOMY (Applied)
A. ERB-DUCHENNE PARALYSIS (Upper Brachial Plexus Lesion - C5, C6)
- Adults: fall of weight on shoulder, motorcycle accident
- Neonates: difficult labour (shoulder dystocia) - most common type
B. KLUMPKE'S PARALYSIS (Lower Brachial Plexus Lesion - C8, T1)
- Adults: person falling and clutching an object, missing a foothold on a moving vehicle
- Neonates: breech presentation with arms above head
C. COMPLETE BRACHIAL PLEXUS LESION (C5-T1)
- Rare, occurs after severe accidents
- Complete paralysis of the upper limb except the upper arm (supplied by C3, C4, C5 via supraclavicular nerves)
- Complete anaesthesia of the entire limb except the upper arm
- Long thoracic nerve (to serratus anterior) and dorsal scapular nerve (to rhomboids) may escape
D. OTHER IMPORTANT CLINICAL POINTS
| Lesion | Structure Involved | Clinical Feature |
|---|---|---|
| Long thoracic nerve injury | C5-C7 roots (or nerve directly) | Winged scapula (serratus anterior paralysis) |
| Axillary nerve injury | Surgical neck of humerus fracture | Deltoid wasting, loss of shoulder abduction; sensory loss over deltoid (regimental badge area) |
| Radial nerve injury (high) | Posterior cord / spiral groove of humerus | Wrist drop, weakness of all finger/wrist/elbow extensors |
| Thoracic outlet syndrome | C8-T1 compression by cervical rib | Features of lower plexus lesion + vascular symptoms |
| Pancoast tumor (lung apex) | T1 root compression | Horner's syndrome + intrinsic hand muscle wasting |
E. RELATIONS IN THE POSTERIOR TRIANGLE (Supraclavicular Part)
- Roots pass between anterior scalene (front) and middle scalene (behind)
- Subclavian artery passes between anterior scalene and rib I (anterior to the plexus roots)
- Erb's point - where C5 and C6 roots unite = most vulnerable point in upper trunk injury; located about 2.5 cm above the clavicle at the posterior border of the sternocleidomastoid
F. RELATIONS IN THE AXILLA (Infraclavicular Part)
- Cords are named relative to the second part of the axillary artery
- The cords split into terminal branches at the lateral border of pectoralis minor
- The inferior trunk rests directly on the first rib and is compressed in a cervical rib
- Gray's Anatomy for Students, pp. 858-865 (brachial plexus, roots, trunks, cords, branches)
- Neuroanatomy through Clinical Cases, 3rd ed., pp. 382-383 (simplified schematics)
- S. Das Manual of Clinical Surgery, 13th ed., pp. 140-141 (Erb-Duchenne and Klumpke's paralysis)
Middle ear cavity according to Atlas anatomy with easy explanation
Middle Ear Cavity (Tympanic Cavity) - Atlas Anatomy
Sources: Color Atlas of Human Anatomy, Vol. 3 (Platzer/Thieme), Gray's Anatomy for Students, Shambaugh Surgery of the Ear, and Cummings Otolaryngology.
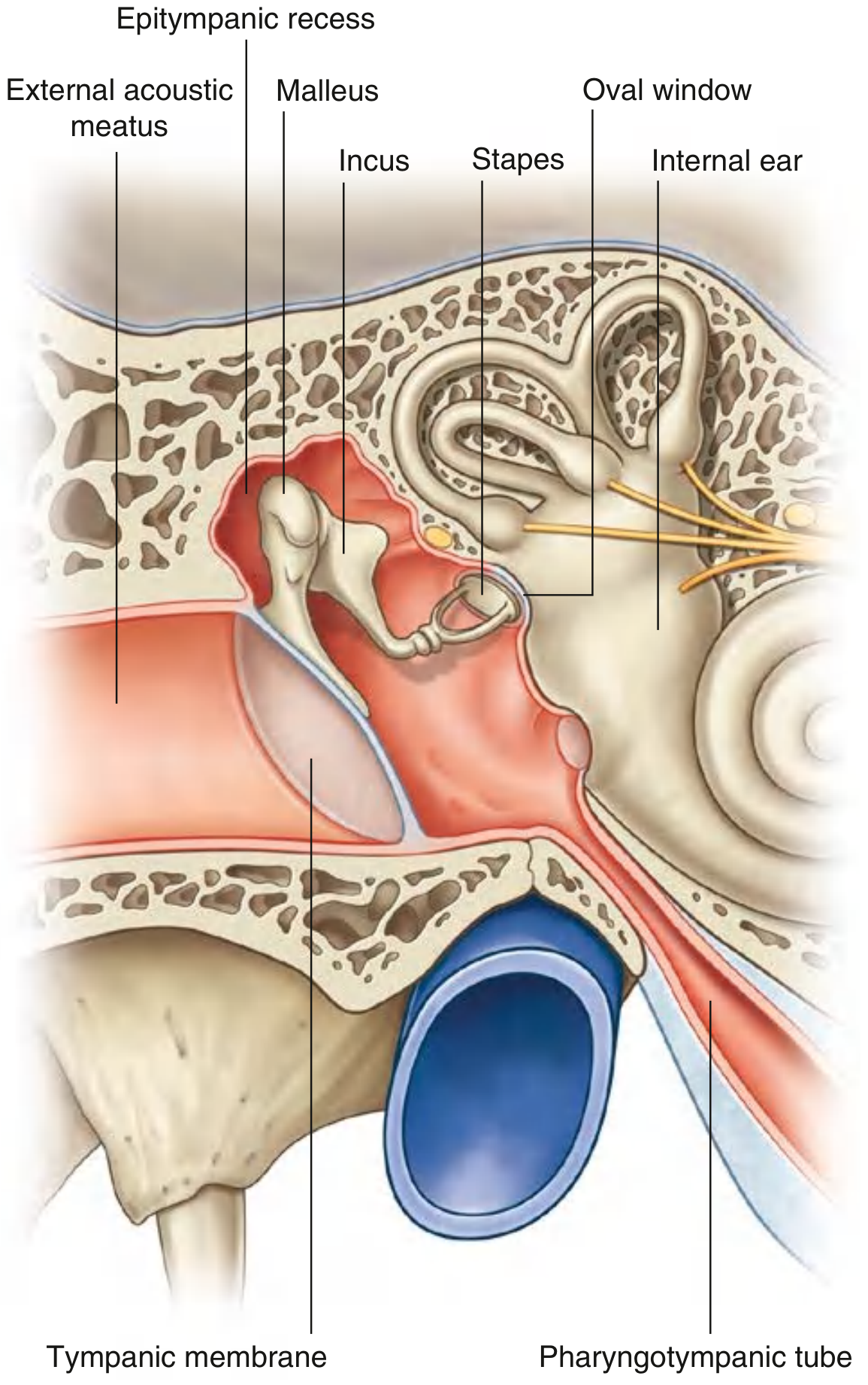
What is the Middle Ear?
- The eardrum (tympanic membrane) on the outside (lateral side)
- The inner ear (cochlea + labyrinth) on the inside (medial side)
Parts of the Middle Ear
| Compartment | Location | Also Called |
|---|---|---|
| Epitympanum (Attic) | Above the tympanic annulus | Epitympanic recess |
| Mesotympanum | At the level of the tympanic membrane | Tympanic cavity proper |
| Hypotympanum | Below the tympanic annulus | Floor region |
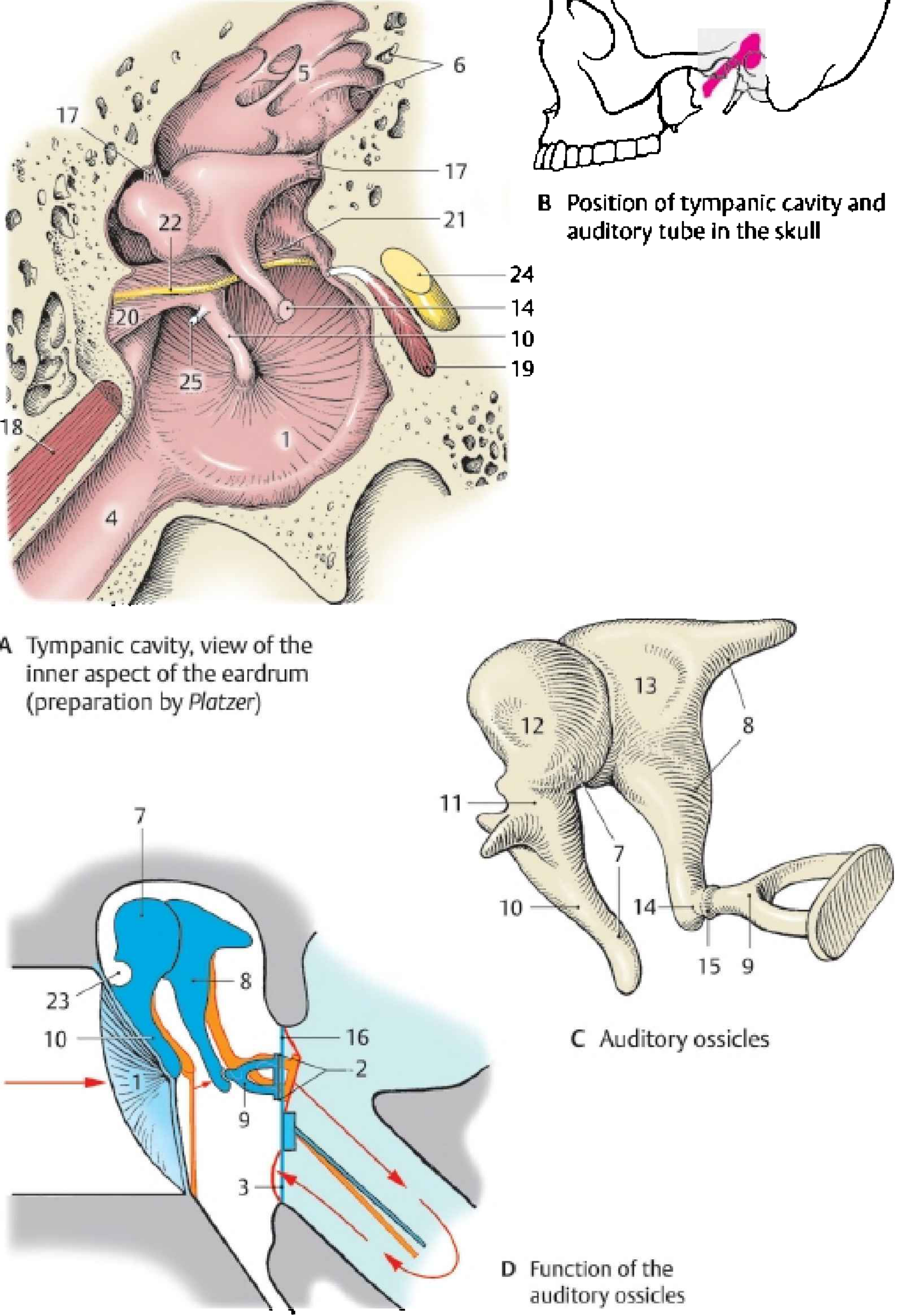
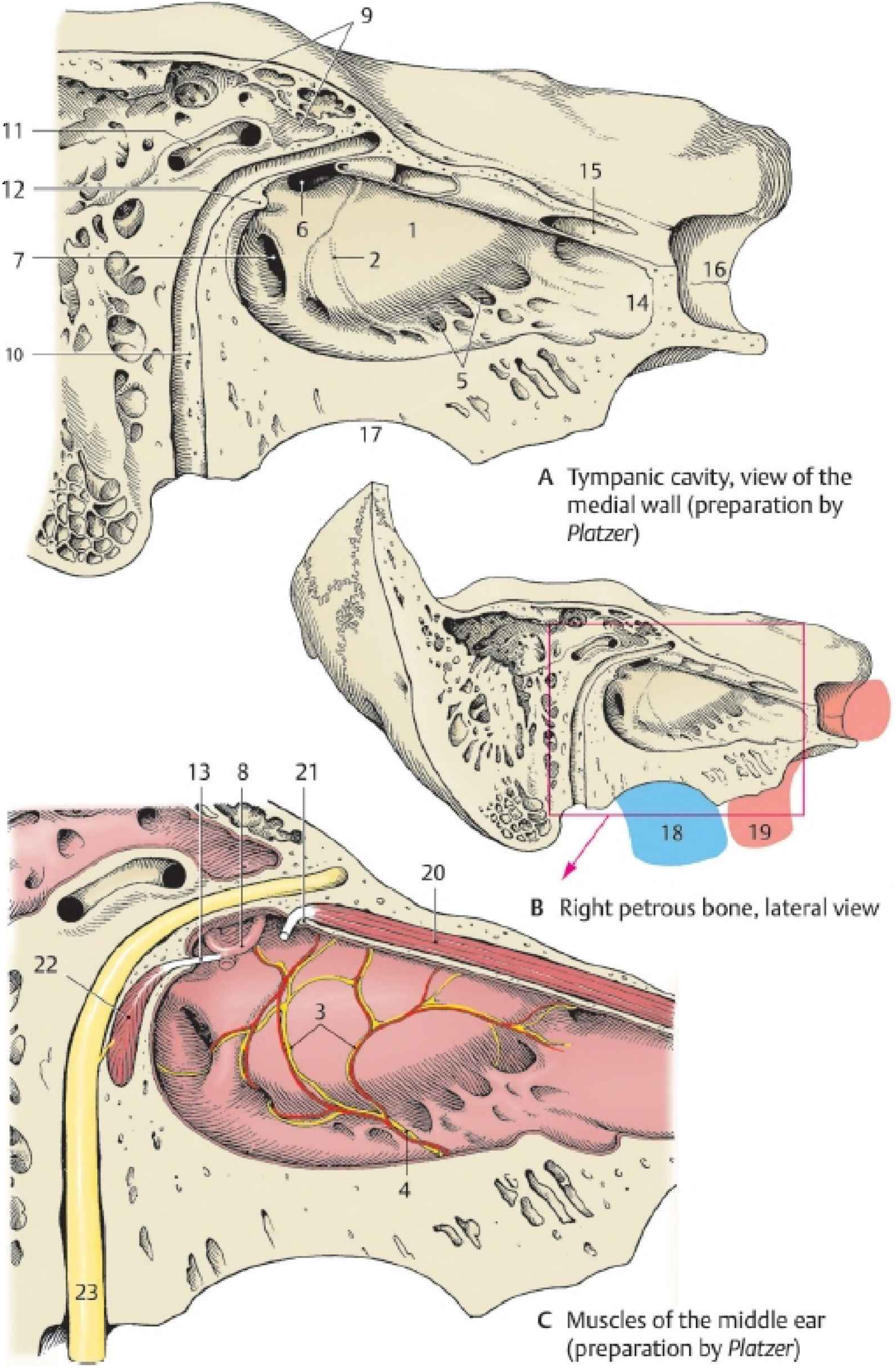
Atlas Diagrams
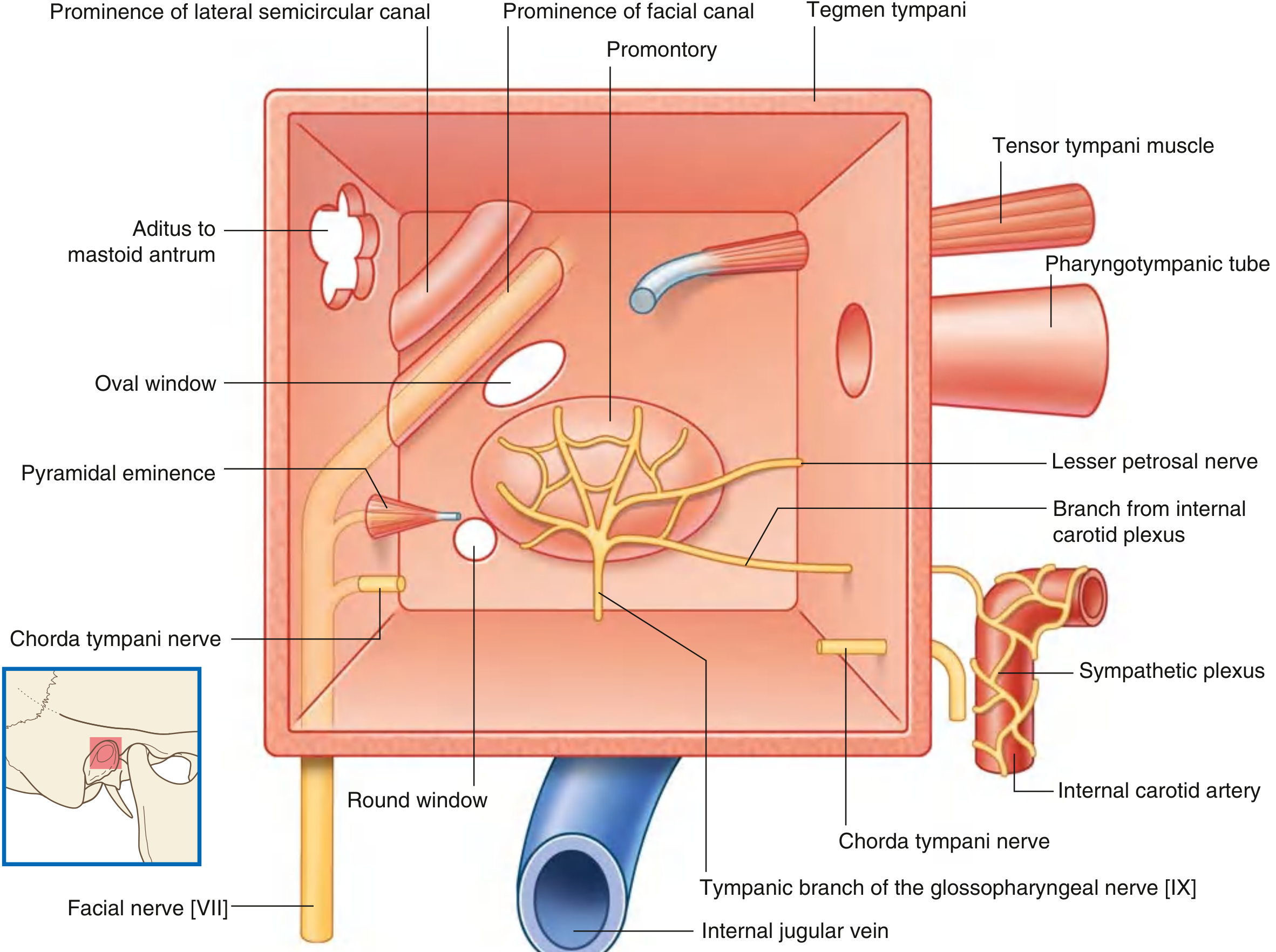

6 Walls of the Middle Ear (Easy Memory Aid: "T J M M A L")
1. ROOF - Tegmental Wall (T)
- Formed by the tegmen tympani - a very thin plate of bone on the petrous temporal bone
- Separates the middle ear from the middle cranial fossa (brain above)
- Clinical: In otitis media, pus can erode through this roof → meningitis or temporal lobe abscess
2. FLOOR - Jugular Wall (J)
- A thin layer of bone separating the cavity from the internal jugular vein (jugular bulb) below
- Near the medial border of the floor: a small aperture for the tympanic branch of CN IX (Jacobson's nerve) to enter
- Clinical: A high-riding jugular bulb can bulge through the floor
3. LATERAL WALL - Membranous Wall (M)
- Formed almost entirely by the tympanic membrane (eardrum)
- The pars tensa (main part, ~10 mm diameter) occupies most of the wall
- The pars flaccida (Shrapnell's membrane) - the small loose part above, between the anterior and posterior malleal folds, at the notch of Rivinus
- The upper portion of this wall (over the epitympanic recess) is bony
4. MEDIAL WALL - Labyrinthine Wall (M)
| Structure | What It Is |
|---|---|
| Promontory | Rounded bulge from the basal coil of the cochlea - the main landmark of the medial wall |
| Tympanic plexus | Network of nerves ON the promontory (CN IX + sympathetic fibers); gives the lesser petrosal nerve |
| Oval window (fenestra vestibuli) | Posterosuperior to promontory; closed by the stapes footplate; leads to vestibule |
| Round window (fenestra cochleae) | Posteroinferior to promontory; closed by the secondary tympanic membrane; leads to scala tympani |
| Prominence of facial canal | Ridge of bone carrying CN VII (facial nerve) in its horizontal (tympanic) segment |
| Prominence of lateral semicircular canal | Ridge above the facial canal prominence |
| Cochleariform process | Spoon-shaped process where the tensor tympani tendon hooks around to insert on malleus |
5. ANTERIOR WALL - Carotid Wall (A)
- Lower part: thin bone separating cavity from the internal carotid artery
- Superiorly, deficient because of two openings:
- Large opening for the pharyngotympanic (Eustachian) tube - equalizes pressure
- Smaller opening for the canal of tensor tympani muscle
- The chorda tympani nerve exits through this wall via the canal of Huguier (petrotympanic fissure)
6. POSTERIOR WALL - Mastoid Wall (L = posterior/back)
- Partially complete
- Key features:
- Aditus to mastoid antrum (superiorly) - the opening connecting middle ear to mastoid air cells
- Pyramidal eminence - a small bony projection through which the tendon of the stapedius muscle enters
- Facial recess - between the facial nerve and chorda tympani
- Sinus tympani - medial to the pyramidal eminence, bounded by the ponticulus (above) and subiculum (below); an important surgical landmark
Contents of the Middle Ear
A. The Three Ossicles (Auditory Bones)
| Ossicle | Meaning | Attachment | Special Feature |
|---|---|---|---|
| Malleus (hammer) | Handle (manubrium) attached to tympanic membrane; head in epitympanum | Lateral end of chain | The umbo = the most medial point of eardrum at the tip of the handle |
| Incus (anvil) | Body articulates with malleus head; long process articulates with stapes | Middle of chain | Connected by synovial joints |
| Stapes (stirrup) | Footplate sits in oval window | Medial end of chain | Smallest bone in the body |
B. Two Muscles of the Middle Ear
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Tensor tympani | Cartilaginous part of Eustachian tube; greater wing of sphenoid | Manubrium of malleus (via cochleariform process) | CN V3 (medial pterygoid nerve) | Pulls malleus medially → tenses eardrum → dampens loud sounds |
| Stapedius | Pyramidal eminence on posterior wall | Neck of stapes | CN VII (facial nerve) | Pulls stapes posteriorly → stiffens oval window → protects from loud sounds |
Clinical note from Color Atlas Vol. 3: Facial nerve palsy paralyzes the stapedius → loss of sound dampening → hyperacusis (oversensitivity/intolerance to sounds)
C. Nerves Passing Through
-
Chorda tympani nerve (branch of CN VII):
- Enters through the posterior wall, lateral to pyramidal eminence
- Crosses the middle ear running lateral to the long process of incus and medial to the neck of malleus
- Exits anteriorly through the canal of Huguier into the petrotympanic fissure
- Carries taste from anterior 2/3 of tongue + parasympathetic to sublingual and submandibular glands
- Clinical: Damaged in middle ear surgery → loss of taste on anterior tongue
-
Tympanic branch of CN IX (Jacobson's nerve):
- Enters via the floor of the tympanic cavity
- Spreads over the promontory as the tympanic plexus
- Continues as the lesser petrosal nerve → otic ganglion → parotid gland (parasympathetic)
-
Facial nerve (CN VII):
- Runs in its bony canal (fallopian canal) along the medial wall (horizontal/tympanic segment)
- NOT in free contact with the cavity but forms the "prominence of the facial canal"
- Makes two bends: 1st genu (geniculate ganglion, anterosuperior) → horizontal segment → 2nd genu (posterior to oval window) → descends in the mastoid
Communications of the Middle Ear
| Direction | Via | Leads to |
|---|---|---|
| Anteriorly | Pharyngotympanic (Eustachian) tube | Nasopharynx |
| Posterosuperiorly | Aditus to mastoid antrum | Mastoid antrum → mastoid air cells |
| Medially | Oval window | Vestibule of inner ear |
| Medially | Round window | Scala tympani of cochlea |
The Pharyngotympanic (Eustachian) Tube
- Connects middle ear to nasopharynx
- Opens on the anterior wall of the middle ear
- In adults: 1/3 bony (near middle ear) + 2/3 cartilaginous (near nasopharynx); angled downward to nasopharynx
- In children: shorter, wider, more horizontal → prone to otitis media (infections track up easily)
- Function: Equalize air pressure on both sides of the eardrum (e.g., swallowing/yawning "pops" the ear)
- Opened by tensor veli palatini and levator veli palatini muscles (CN V3 and CN X)
Clinical Points (Easy Summary)
| Condition | Anatomy Involved | Why |
|---|---|---|
| Acute Otitis Media (AOM) | Middle ear cavity | Bacteria ascend via Eustachian tube (more common in children due to horizontal tube) |
| Mastoiditis | Aditus → mastoid antrum | Mucous membrane of middle ear is continuous with mastoid cells; infection spreads posteriorly |
| Meningitis/Brain abscess | Tegmen tympani (roof) | Very thin bone; otitis media can erode it upward into the middle cranial fossa |
| Hyperacusis | Stapedius / CN VII palsy | Facial nerve palsy → stapedius paralyzed → no sound dampening |
| Otosclerosis | Stapes footplate | Abnormal bone growth fixes the stapes footplate in the oval window → conductive deafness |
| Glue ear (OME) | Middle ear + Eustachian tube | Blocked Eustachian tube → fluid accumulates → conductive hearing loss |
| Cholesteatoma | Pars flaccida / epitympanum | Keratin-filled cyst that erodes bone; typically starts at Shrapnell's membrane |
| Jugular thrombosis | Jugular wall (floor) | Infection erodes thin floor → internal jugular vein thrombosis |
- Color Atlas of Human Anatomy Vol. 3 (Nervous System & Sense Organs), pp. 514-522 (Platzer/Thieme) - all atlas diagrams
- Gray's Anatomy for Students, pp. 1098-1103 (middle ear walls, contents, pharyngotympanic tube)
- Shambaugh Surgery of the Ear, pp. 800-802 (tympanic cavity divisions, mesotympanum, chorda tympani)
Can you tell me about the paper-wise syllabus distribution for MBBS first year biochemistry according to the MPMSU?
MPMSU MBBS first year biochemistry paper wise syllabus distribution 2024
Madhya Pradesh Medical Science University MBBS biochemistry syllabus paper 1 paper 2 topics
https://api.nscbmc.ac.in/images/academics/1QaWJ.pdf
MPMSU MBBS biochemistry syllabus R-24 2024 paper 1 paper 2 topics marks distribution nscbmc
https://www.rims.edu.in/secure/wp-content/uploads/Syllabus-f…
MPMSU Jabalpur MBBS 1st year biochemistry syllabus 2024 NMC CBME paper 1 paper 2 topic wise marks
https://www.scribd.com/document/702926980/1st-MBBS-Syllabus-…
MBBS First Year Biochemistry - Paper-wise Syllabus Distribution (MPMSU)
Note: B.D. Chaurasia is not available in the library's biochemistry collection. The syllabus below is sourced directly from MPMSU's Adhoc Board of Studies document (as applicable to affiliated colleges including NSCBMC, Jabalpur) and the RIMS syllabus document used by MPMSU-affiliated institutes. The R-24 scheme (Batch 2024 onwards) follows NMC guidelines dated 12-09-2024.
Scheme of Examination - Overview
| Component | Marks | Passing Criteria |
|---|---|---|
| Theory - Paper I | 100 | Minimum 40% in theory |
| Theory - Paper II | 100 | |
| Practical (including 20 marks Viva Voce) | 100 | Minimum 40% in practical |
| Total | 300 | 50% aggregate (theory + practical combined) |
- Duration of each theory paper: 3 hours (R-24 scheme)
- Two examinations per year: Main and Supplementary
PAPER I - Topics (100 Marks)
| S.No. | Topic |
|---|---|
| 1 | Physical aspects of biochemistry (pH, buffers, water) |
| 2 | Cellular structure and functions |
| 3 | Chemistry of biomolecules |
| 4 | Transport across membranes |
| 5 | Chemistry of Carbohydrates, Lipids, Proteins, Nucleic acids |
| 6 | Radioisotopes and their application in Medicine |
| 7 | Enzymology (enzyme kinetics, inhibition, clinical applications) |
| 8 | Porphyrins (haemoglobin synthesis, porphyrias) |
| 9 | Chemistry of respiration (biological oxidation - electron transport chain, oxidative phosphorylation) |
| 10 | Acid-base balance |
| 11 | Body fluid and electrolyte balance |
| 12 | Immune system and immunochemistry |
| 13 | Organ functional tests (liver, kidney, pancreas) |
Paper I Focus: Chemistry (structure) of all biomolecules + enzymes + fundamental concepts + clinical chemistry tests
PAPER II - Topics (100 Marks)
| S.No. | Topic |
|---|---|
| 1 | Bioenergetics |
| 2 | Digestion and absorption |
| 3 | Metabolism of carbohydrates, lipids, proteins, nucleic acids, purines and pyrimidines |
| 4 | Biochemical basis of inherited disorders and their sequelae (inborn errors of metabolism) |
| 5 | Diet and nutrition including vitamins, minerals and energy metabolism |
| 6 | Hormones (chemistry, synthesis, metabolism and action) |
| 7 | Molecular biology (DNA replication, transcription, translation, genetic code) |
| 8 | Environmental health hazards |
| 9 | Cancer and carcinogenesis |
| 10 | Principles of genetic engineering and biotechnology |
| 11 | AETCOM (Attitude, Ethics and Communication module) integrated topics |
Paper II Focus: Metabolism of all biomolecules + molecular biology + applied/clinical aspects
Question Paper Format (R-24 Scheme - NMC 2024)
| Section | Type | Details | Marks |
|---|---|---|---|
| Section A | MCQ | 10 scenario-based / clinical application MCQs (1 mark each) | 10 |
| Section B | BAQ (Brief Answer Questions) | ~8-10 brief questions (includes reasoning questions) | ~20 |
| Section C | SAQ (Short Answer Questions) | Includes clinical application SAQs + integrated topic SAQs (e.g., diabetes, IHD, anaemia) | ~30 |
| Section D | LAQ (Long Answer Questions) | 1-2 structured long answer questions with defined marks distribution | ~40 |
Integrated topics examined in SAQs include: Anaemia, Ischaemic heart disease, Diabetes mellitus, Tuberculosis, Hypertension, and Thyroid disorders.
Practical Examination (100 Marks)
| S.No. | Component | Marks |
|---|---|---|
| 1 | Viva Voce | 20 |
| 2 | Long quantitative experiment (e.g., estimation of glucose, protein, urea) | ~30 |
| 3 | Urine analysis | ~20 |
| 4 | Spotting / Quality control / OSPE | ~30 |
Practicals Covered:
- Colorimetry and spectrophotometry
- Flame photometry
- Gel electrophoresis
- Chromatography (paper and TLC)
- pH measurement and buffer preparation
- Estimation of blood glucose, serum proteins, urea, creatinine, bilirubin, cholesterol
- Urine examination (normal and abnormal constituents)
- CSF sugar and protein estimation
- Liver function tests, kidney function tests
Internal Assessment (R-24 Scheme)
| Component | Marks |
|---|---|
| PCT (Progress/Class Tests) | 10 |
| 1st Sessional Exam | 20 |
| Pre-University Exam | 40 |
| SDL (Self-directed learning - library, home assignments, museum study) | 20 |
| Log Book (ECE, AETCOM) | 10 |
| Component | Marks |
|---|---|
| PCT | 10 |
| 1st Sessional Exam | 20 |
| Pre-University | 20 |
| OSPE | 10 |
| Seminar | 10 |
| Journals | 20 |
| Log Book | 10 |
Teaching Hours (Phase-I MBBS)
| Category | Hours |
|---|---|
| Large Group Teaching (Lectures) | 82 |
| SGT / Practicals / Tutorials / Seminars | 157 |
| Self-Directed Learning (SDL) | 10 |
| Total | 249 hours |
Important Points to Remember
- Paper I = Chemistry (what molecules ARE) + Enzymes + Functional tests
- Paper II = Metabolism (what molecules DO) + Molecular biology + Applied biochemistry
- Questions can be asked from any paper's topics in either paper - the distribution is a guideline, not an absolute restriction
- AETCOM topics are included in both Paper I and Paper II as short answer questions
- From R-24 batch, MCQs are scenario-based (not straight recall), reflecting the NMC's shift toward competency-based assessment
- The passing criteria is 40% separately in theory and practical, with a minimum 50% aggregate
- MPMSU Adhoc Board of Studies - NSCBMC Jabalpur document (NMC Guidelines D-11011/500/2024-AcademicCell, 12-09-2024)
- RIMS MBBS syllabus (Paper I & II biochemistry topics used by MPMSU-affiliated colleges)
- Scribd: MPMSU MBBS First Year Exam Scheme document