Cardiac cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer:
The Cardiac Cycle
The cardiac cycle refers to the complete sequence of mechanical and electrical events that repeats with every heartbeat. At a heart rate of 72 beats/min, one cycle lasts approximately 0.833 seconds (duration = 60 / heart rate). - Guyton and Hall Textbook of Medical Physiology
Initiation
Each cycle is triggered by a spontaneous action potential in the sinoatrial (SA) node, located in the superior lateral wall of the right atrium near the opening of the superior vena cava. The impulse travels rapidly through both atria, then passes through the AV node into the ventricles. A delay of >0.1 second at the AV node allows the atria to contract first, acting as "primer pumps" that top up the ventricles before powerful ventricular contraction begins. - Guyton & Hall
Overview Diagram (Costanzo Physiology)
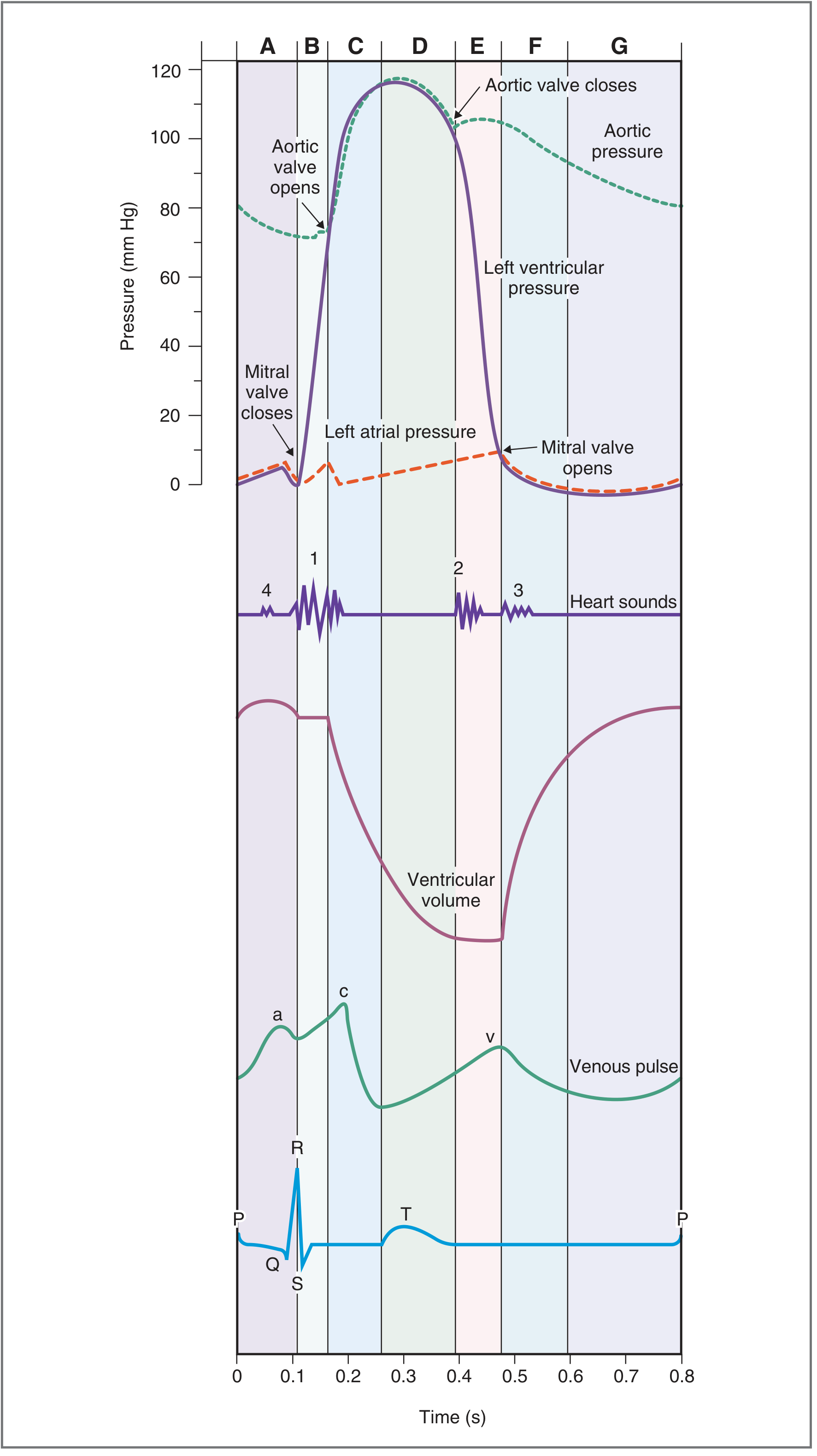
Fig. 4.25 - The cardiac cycle with all 7 phases (A-G), left ventricular/atrial/aortic pressures, ventricular volume, venous pulse, and ECG. - Costanzo Physiology 7th Edition
The Seven Phases (Costanzo Classification)
The cycle is most conveniently divided into 7 phases. Here is a complete summary:
| Phase | Name | ECG Event | Valves | Heart Sound | Key Events |
|---|---|---|---|---|---|
| A | Atrial Systole | P wave / PR interval | Mitral open | S4 (if present) | Atria contract; final ~20% of ventricular filling |
| B | Isovolumetric Ventricular Contraction | QRS complex | Mitral closes | S1 | Ventricular pressure rises sharply; all valves closed; volume constant |
| C | Rapid Ventricular Ejection | ST segment | Aortic valve opens | - | Most of stroke volume ejected; ventricular volume drops rapidly |
| D | Reduced Ventricular Ejection | T wave | - | - | Ejection slows; ventricular volume reaches minimum (ESV) |
| E | Isovolumetric Ventricular Relaxation | After T wave | Aortic valve closes | S2 | Ventricular pressure falls; all valves closed; volume constant |
| F | Rapid Ventricular Filling | - | Mitral valve opens | S3 (if present) | Ventricles fill passively; volume rises rapidly |
| G | Reduced Ventricular Filling (Diastasis) | - | - | - | Slow filling; pressure equalizes between atrium and ventricle |
Table adapted from Costanzo Physiology 7th Edition, Table 4.5
Detailed Phase-by-Phase Description
Phase A - Atrial Systole
Atrial contraction is triggered by the P wave on the ECG. The mitral valve is already open (from the previous cycle), so atrial contraction forces an additional bolus of blood into the relaxed left ventricle. This produces a small "blip" in left ventricular pressure and appears as the a wave on the jugular venous pulse (JVP). At rest, atrial contraction contributes <20% of stroke volume; during heavy exercise, this can rise to 40%. The fourth heart sound (S4), if audible, coincides with atrial contraction and reflects a stiff, non-compliant ventricle (e.g., in ventricular hypertrophy). - Costanzo; Medical Physiology (Boron & Boulpaep)
Phase B - Isovolumetric Ventricular Contraction
The QRS complex marks ventricular depolarization and the start of ventricular contraction. As left ventricular pressure rises and exceeds left atrial pressure, the mitral valve closes - generating the first heart sound (S1). S1 may be split because the mitral valve closes slightly before the tricuspid valve. All valves are now closed, so ventricular volume is constant (isovolumetric) while pressure rises steeply. - Costanzo
Phase C - Rapid Ventricular Ejection
When left ventricular pressure exceeds aortic pressure (~80 mmHg diastolic), the aortic valve opens. Blood is rapidly ejected into the aorta along the pressure gradient. Ventricular pressure rises to its maximum (~120 mmHg systolic) and aortic pressure rises in parallel. Most of the stroke volume is ejected during this brief phase. Ventricular volume falls dramatically. Simultaneously, the left atrium begins refilling from the pulmonary veins. - Costanzo
Phase D - Reduced Ventricular Ejection
The T wave on the ECG marks ventricular repolarization. Ventricular contractile force wanes, so ejection slows. Although the aortic valve is still open and blood continues to enter the aorta, blood "runs off" into the arterial tree faster than it is being added, so aortic pressure begins to fall. Ventricular volume reaches its minimum, known as end-systolic volume (ESV), which is approximately 50 mL at rest. - Costanzo; Medical Physiology
Phase E - Isovolumetric Ventricular Relaxation
When ventricular pressure falls below aortic pressure, the aortic valve closes, generating the second heart sound (S2). The aortic valve closes slightly before the pulmonic valve; during inspiration, the pulmonic valve closure is delayed (increased right ventricular filling via Frank-Starling) producing physiological splitting of S2. All valves are again closed. Ventricular pressure falls rapidly while volume remains constant. - Costanzo
Phase F - Rapid Ventricular Filling
When ventricular pressure falls below left atrial pressure, the mitral valve opens. Blood flows rapidly and passively from atrium to ventricle down the pressure gradient, increasing ventricular volume quickly. The third heart sound (S3) may be heard at the start of this phase, caused by sudden deceleration of blood filling the ventricle. S3 is normal in children and young adults; in older adults it suggests ventricular dysfunction (e.g., dilated cardiomyopathy). - Costanzo
Phase G - Reduced Ventricular Filling (Diastasis)
Filling slows as ventricular and atrial pressures equalize. Both chambers are at relatively low pressure with the mitral valve wide open, and only minimal flow occurs between them - driven by the slightly higher pressure in the pulmonary veins. This "quiet" period ends when the P wave fires and the next atrial systole begins the cycle anew. - Medical Physiology (Boron & Boulpaep)
Pressure and Volume Key Values (Left Heart at Rest)
| Parameter | Approximate Value |
|---|---|
| End-diastolic volume (EDV) | ~120-130 mL |
| End-systolic volume (ESV) | ~50 mL |
| Stroke volume (EDV - ESV) | ~70-80 mL |
| Ejection fraction (SV/EDV) | ~55-65% |
| Peak LV systolic pressure | ~120 mmHg |
| LV diastolic pressure | ~5-12 mmHg |
| Aortic diastolic pressure | ~80 mmHg |
| Duration at HR 72 bpm | ~0.83 s |
ECG-to-Mechanical Event Correlations
| ECG Event | Mechanical Correlate |
|---|---|
| P wave | Atrial depolarization → atrial contraction begins |
| PR interval | AV nodal delay (allows atrial emptying before ventricular contraction) |
| QRS complex | Ventricular depolarization → isovolumetric contraction begins |
| ST segment | Ventricular plateau (depolarized); rapid ejection occurring |
| T wave | Ventricular repolarization → ejection slowing, then aortic valve closes |
Heart Sounds Summary
| Sound | Timing | Cause | Clinical Note |
|---|---|---|---|
| S1 ("lub") | Start of ventricular systole | Closure of mitral + tricuspid valves | Heard best at apex (mitral) or lower left sternal border (tricuspid) |
| S2 ("dub") | End of ventricular systole | Closure of aortic + pulmonic valves | A2 before P2; splits with inspiration |
| S3 | Early diastole (rapid filling) | Sudden deceleration of filling blood | Normal in youth; pathological in adults (ventricular failure) |
| S4 | Late diastole (atrial kick) | Atrial contraction against stiff ventricle | Always pathological in adults; heard in LVH, hypertension |
Effect of Heart Rate on Cycle Duration
When heart rate increases, diastole is disproportionately shortened compared to systole. At 72 bpm, systole comprises ~40% of the cycle. At three times the normal rate, systole occupies ~65% of the cycle. This is why very high heart rates can impair ventricular filling and reduce cardiac output - the heart does not have enough time to fill completely. - Guyton & Hall
Jugular Venous Pulse Waves
The JVP reflects atrial pressure changes and has three upward deflections:
- a wave: atrial contraction (end of diastole)
- c wave: tricuspid valve closure / bulging into atrium at start of systole
- v wave: atrial filling against a closed tricuspid valve during ventricular systole
Sources:
- Guyton and Hall Textbook of Medical Physiology
- Costanzo Physiology, 7th Edition
- Medical Physiology (Boron & Boulpaep)
- Morgan & Mikhail's Clinical Anesthesiology, 7e
Create a visual study guide or poster diagram of the 7 cardiac cycle phases
Generating Image
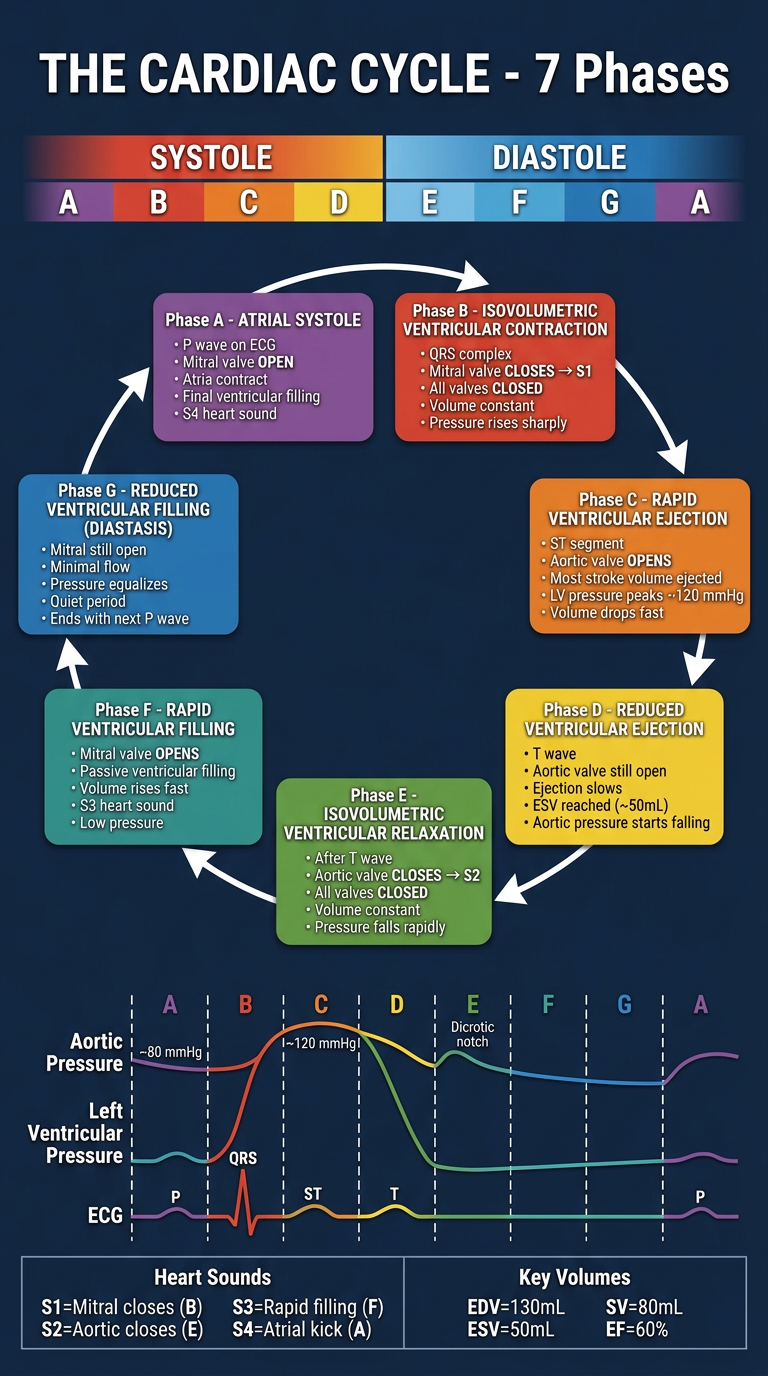
Here is your cardiac cycle study poster. It covers:
- 7 color-coded phase cards (A through G) arranged in sequential flow with phase names, ECG correlates, valve events, and key pressures/volumes
- Systole vs. Diastole division clearly marked
- Wiggers-style diagram strip at the bottom aligning aortic pressure, LV pressure, and ECG with the phases
- Heart sounds quick reference (S1-S4) and key volume values (EDV, ESV, SV, EF)
A quick recap of the flow:
- A (Atrial systole) → B (Isovolumetric contraction, S1) → C (Rapid ejection) → D (Reduced ejection) → E (Isovolumetric relaxation, S2) → F (Rapid filling, S3) → G (Diastasis) → back to A
prepare me the course of glossopharyngeal nerve using flowchart
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Generating Image
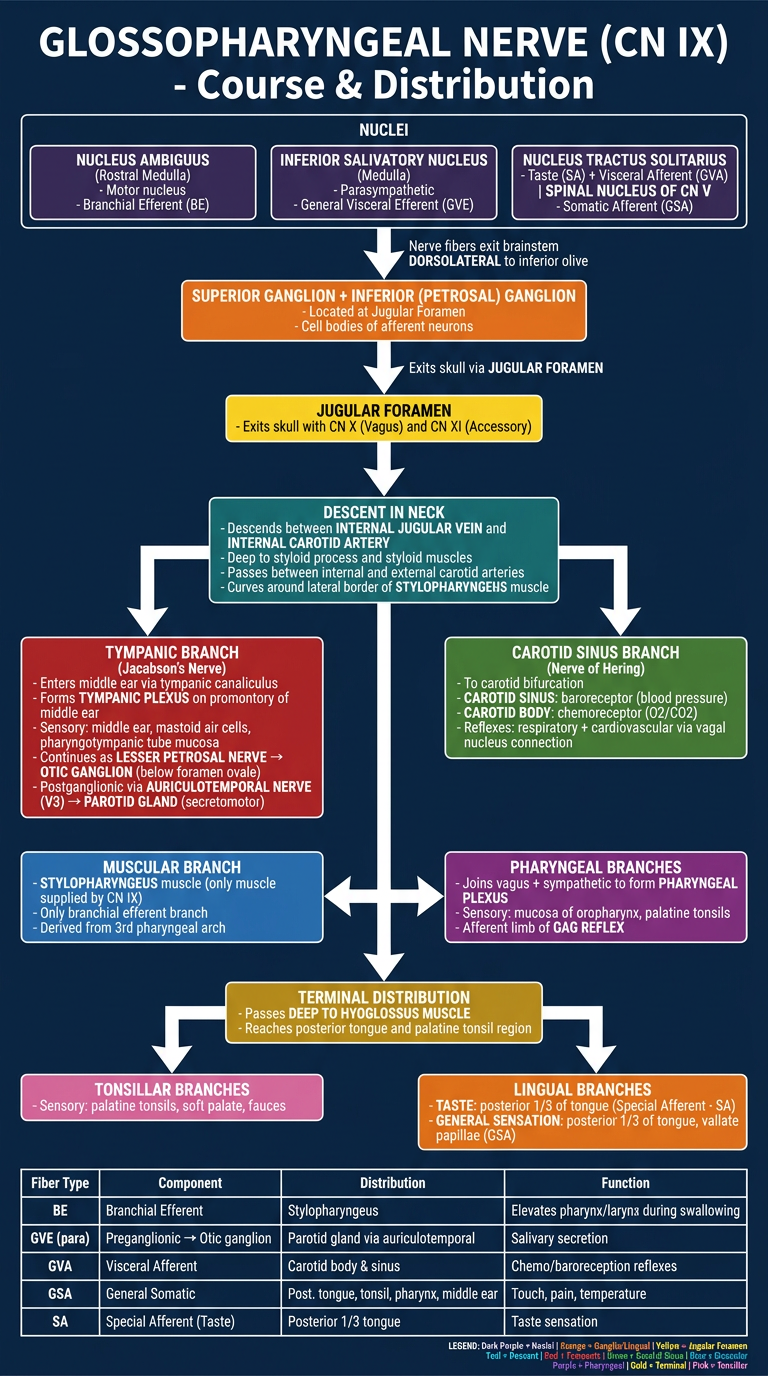
Here is your CN IX flowchart poster. Below is a full written companion to go with it:
Course of the Glossopharyngeal Nerve (CN IX)
Fiber Types (5 components)
| Fiber | Type | Function |
|---|---|---|
| BE | Branchial Efferent | Motor to stylopharyngeus |
| GVE | General Visceral Efferent (parasympathetic) | Secretomotor to parotid gland |
| GVA | General Visceral Afferent | Carotid body & sinus reflexes |
| GSA | General Somatic Afferent | Sensation - posterior tongue, tonsil, pharynx, middle ear |
| SA | Special Afferent (taste) | Taste from posterior 1/3 of tongue |
Step-by-Step Course
1. Nuclei (Medulla)
- Nucleus ambiguus (rostral) - motor origin
- Inferior salivatory nucleus - parasympathetic preganglionic origin
- Nucleus tractus solitarius - receives taste and visceral afferents
- Spinal trigeminal nucleus - receives somatic pain/temperature
2. Brainstem Exit
Fibers emerge dorsolateral to the inferior olive on the lateral medulla.
3. Ganglia
Superior ganglion and inferior (petrosal) ganglion sit at the jugular foramen - contain cell bodies of afferent neurons.
4. Jugular Foramen
Exits the skull alongside CN X (vagus) and CN XI (accessory).
5. Descent in the Neck
Passes between the internal jugular vein and internal carotid artery, deep to the styloid process. It then curves around the lateral border of the stylopharyngeus muscle, passing between the internal and external carotid arteries, before travelling deep to hyoglossus towards the tongue base.
Branches & Their Distribution
| Branch | Where Given Off | Distribution |
|---|---|---|
| Tympanic nerve (Jacobson's nerve) | At jugular foramen | Middle ear mucosa, mastoid air cells, pharyngotympanic tube; continues as lesser petrosal nerve → otic ganglion → parotid gland via auriculotemporal nerve (V3) |
| Carotid sinus branch (Nerve of Hering) | In neck | Carotid sinus (baroreceptor) and carotid body (chemoreceptor); mediates cardiorespiratory reflexes |
| Muscular branch | In neck | Stylopharyngeus - the ONLY muscle supplied by CN IX (3rd pharyngeal arch derivative) |
| Pharyngeal branches | In neck | Joins vagus + sympathetics to form pharyngeal plexus; sensory to oropharynx; afferent limb of gag reflex |
| Tonsillar branches | Terminal | Sensory to palatine tonsils, soft palate, fauces |
| Lingual branches | Terminal | Taste (SA) + general sensation (GSA) from posterior 1/3 of tongue and vallate papillae |
Key Anatomical Relationships
- Deep to styloid process and styloid muscles in the upper neck
- Between internal and external carotid arteries as it descends
- Curves around lateral border of stylopharyngeus
- Deep to hyoglossus to reach tongue base
Clinical Correlate
Glossopharyngeal neuralgia - paroxysmal stabbing pain in the posterior tongue, tonsillar fossa, pharynx, or ear, triggered by swallowing/yawning. In severe cases, simultaneous vagal compression can trigger bradycardia or asystole.
Sources: Gray's Anatomy for Students; Bradley and Daroff's Neurology in Clinical Practice; Scott-Brown's Otorhinolaryngology
preprepare the same for spinal accessory nerve and hypoglossal nerve
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Generating Image
Generating Image
prepare it a little faster
Generating Image
Generating Image
This is a shared conversation. Sign in to Orris to start your own chat.