AWMI+TPWMI
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive material. Let me compile a full, well-organized answer.
AWMI + TPWMI: Anterior Wall MI vs. True Posterior Wall MI
I. ANTERIOR WALL MYOCARDIAL INFARCTION (AWMI)
Coronary Territory
The anterior wall of the left ventricle is supplied by the left anterior descending (LAD) artery. LAD occlusion is the most common cause of AWMI and produces the largest infarcts - often leading to extensive LV dysfunction and cardiogenic shock.
ECG Criteria (STEMI)
From Tintinalli's Table 49-4:
| Subtype | ECG Changes |
|---|---|
| Anteroseptal | ST elevation in V1, V2, (± V3) |
| Anterior | ST elevation in V1, V2, V3, V4 |
| Anterolateral | ST elevation in V1-V6, I, and aVL |
| Lateral only | ST elevation in I and aVL |
Reciprocal changes: ST depression in inferior leads (II, III, aVF). ST elevation in aVR can also accompany extensive anterior STEMI and suggests proximal LAD or left main occlusion.
Sequence of ECG Changes in AWMI
- Hyperacute T waves - tall, peaked T waves in V1-V4 (earliest sign, often missed)
- ST elevation - upsloping then convex/tombstone elevation in V1-V4
- Q wave development - pathological Q waves (>0.04 s, >25% of R wave) in affected leads
- T wave inversion - after ST normalizes
- Persistent ST elevation - when present beyond 2 weeks suggests LV aneurysm / large akinetic area
Key Complications of AWMI
- Cardiogenic shock - most common cause is large anterior wall MI (LAD territory)
- LV aneurysm / thrombus - occurs most often post-anterior MI; LV thrombus warrants anticoagulation (warfarin preferred; DOACs have conflicting evidence)
- VSD (interventricular septal rupture) - more common in anterior MI than inferior
- Complete heart block - anterior MI causes block in distal His-Purkinje system → wide complex escape rhythms, poor prognosis
- New LBBB - suggests large anterior MI, worse prognosis
- Bundle branch / hemiblock - new development = extensive anterior MI
II. TRUE POSTERIOR WALL MI (TPWMI)
Coronary Territory
The true posterior wall (inferobasal LV) is supplied by the posterior descending artery (PDA), which arises from:
- The right coronary artery (RCA) in right-dominant systems (most common)
- The left circumflex (LCx) in left-dominant systems
TPWMI almost always accompanies inferior MI or inferolateral MI. It rarely occurs in isolation.
Why It's "True Posterior"
The standard 12-lead ECG does not directly face the posterior wall - V1 and V2 are the "mirror image" leads. Therefore, TPWMI produces reciprocal/mirror changes in V1-V2, not primary ST elevation.
ECG Criteria for TPWMI
From Rosen's Emergency Medicine and Tintinalli's Table 49-4:
In V1-V2 (reciprocal / mirror changes):
- Tall, wide R wave (R ≥ 0.04 s) - the mirror image of a posterior Q wave
- R/S ratio ≥ 1 in V1
- Horizontal ST depression (not upsloping)
- Upright (tall) T wave - "positive T wave" in V1-V2 during an acute event
The combination of horizontal ST depression + upright T wave in V1-V2 increases diagnostic accuracy significantly.
Posterior leads (V7, V8, V9) - direct imaging:
- Placed at the posterior chest (V7 = posterior axillary line, V8 = tip of scapula, V9 = paraspinal)
- Show ST elevation ≥ 0.5 mm, directly confirming TPWMI
- V8 and V9 have subtle ST elevation (as shown in the image below)
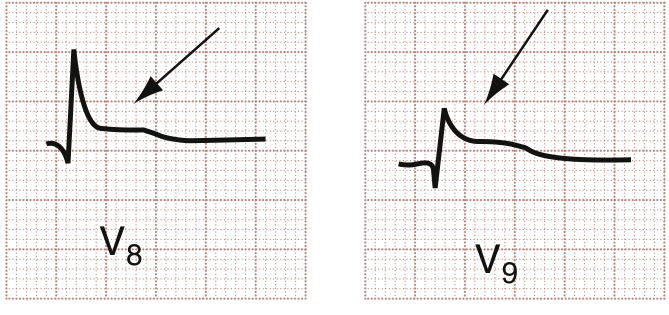
Posterior leads V8 and V9: arrows indicate ST elevation consistent with acute posterior wall MI - Rosen's Emergency Medicine
Important Clinical Notes on TPWMI
- Tall R in V1 may be delayed - emergence can lag behind the infarct because it represents a developing posterior Q wave in mirror
- Cardiac MRI evidence suggests many so-called "posterior" infarctions (with tall R in V1-V2) are actually lateral LV wall MIs - a consensus document has proposed reclassifying them as "inferobasal MI"
- Patients with inferior MI who also have ST depression in V1-V3 or ST elevation in V8-V9 have: larger infarct zones, lower ejection fractions, higher morbidity and mortality than isolated inferior MI
- Fibrinolysis indication: ST depression in ≥2 precordial leads (V1-V4) as a sign of posterior STEMI is a recognized indication for fibrinolytic therapy
III. Side-by-Side Comparison
| Feature | AWMI | TPWMI |
|---|---|---|
| Artery | LAD | PDA (from RCA or LCx) |
| Primary ECG leads | V1-V4 (± I, aVL) | No direct standard lead; V7-V9 (posterior) |
| Standard 12-lead sign | ST elevation V1-V4 | ST depression + tall R + upright T in V1-V2 |
| Pathological Q waves | V1-V4 | Not seen in standard leads (mirror R wave instead) |
| Reciprocal changes | ST depression in II, III, aVF | ST elevation appears in V7-V9 if checked |
| Key complication | Cardiogenic shock, VSD, LV thrombus, LBBB | Usually accompanies inferior MI; larger infarct zone |
| Prognosis | Worst prognosis among STEMI locations | Worse than isolated inferior MI |
| Management | Primary PCI / fibrinolysis | Primary PCI; fibrinolysis indicated for V1-V4 depression |
IV. Management Principles (Both)
- Primary PCI is the treatment of choice when available within the recommended time window (door-to-balloon ≤90 min)
- Fibrinolysis (TNK preferred - single bolus, most fibrin-specific, 80x more resistant to PAI-1 than t-PA) when PCI unavailable within time target
- TPWMI with ST depression in ≥2 precordial leads (V1-V4) qualifies as a fibrinolysis indication
- Antiplatelet + anticoagulation combined with reperfusion strategy
- Avoid nitrates in suspected RV infarction (often accompanies inferior/posterior MI) as nitrate-induced hypotension can be severe
Sources: Tintinalli's Emergency Medicine (Table 49-4, p.378) - Rosen's Emergency Medicine (Fig. 64.13, Posterior Leads section) - The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.