Pharmcodynamics according to neet pg exam
Reading File
Finding Sources
Searching the Web
pharmacodynamics NEET PG high yield topics receptors dose response
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from the textbooks. Let me compile this into a thorough NEET PG-focused pharmacodynamics guide.
Pharmacodynamics - NEET PG High-Yield Notes
1. Definition
Pharmacodynamics = What the drug does to the body (vs. pharmacokinetics = what the body does to the drug).
It describes mechanisms of drug action, drug-receptor interactions, and dose-response relationships.
"Pharmacodynamics describes the actions of a drug on the body. Most drugs exert effects, both beneficial and harmful, by interacting with specialized target macromolecules called receptors." - Lippincott Illustrated Reviews: Pharmacology
2. Drug-Receptor Bonds (Types)
| Bond Type | Strength | Key Feature |
|---|---|---|
| Covalent | Strongest | Often irreversible (e.g., aspirin-COX, alkylating agents) |
| Electrostatic (ionic, H-bonds, van der Waals) | Intermediate | Most common type in drug-receptor interactions |
| Hydrophobic | Weakest | Important for lipid-soluble drugs |
NEET PG Key Point: Drugs forming weak bonds are MORE selective (require precise fit). Drugs forming strong covalent bonds tend to be less selective.
Classic example: Aspirin acetylates (covalent bond) COX in platelets irreversibly - effect lasts until new platelets are synthesized (7-10 days).
3. Receptor Families - The Big Four
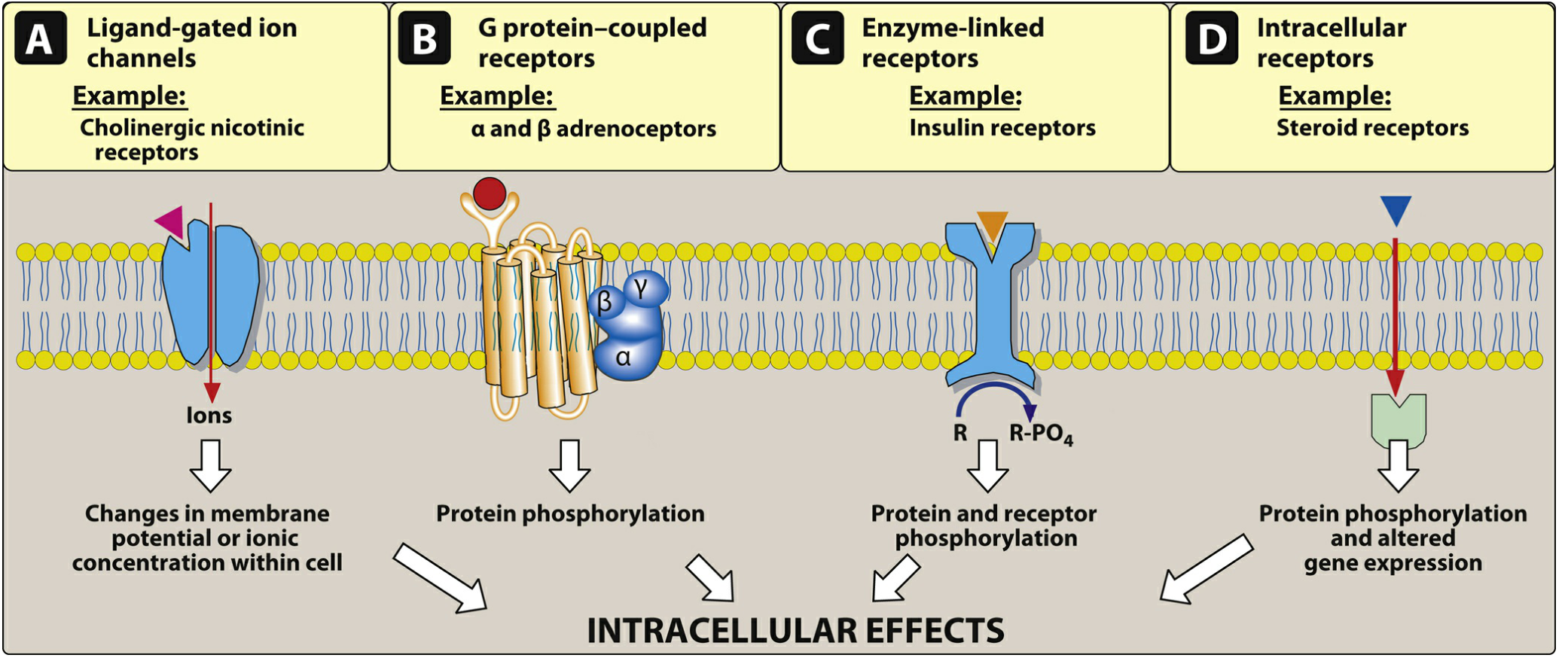
| Receptor Type | Mechanism | Onset | Examples |
|---|---|---|---|
| Type I - Ligand-gated ion channels | Ion flux directly | Milliseconds (fastest) | Nicotinic ACh receptor, GABA-A, Glycine, 5-HT3 |
| Type II - G protein-coupled receptors (GPCRs) | G protein → 2nd messenger | Seconds to minutes | Muscarinic, β-adrenergic, α-adrenergic, Opioid, Dopamine |
| Type III - Enzyme-linked receptors (RTKs) | Tyrosine kinase activation | Minutes to hours | Insulin receptor, Growth factor receptors |
| Type IV - Intracellular/nuclear receptors | Gene transcription | Hours to days (slowest) | Steroid hormones, Thyroid hormone, Vit D, Retinoids |
Memory Aid: "I Go Eat Inside" (Ion channel → G-protein → Enzyme-linked → Intracellular)
Key NEET PG facts about GPCRs:
- Gs → activates adenylyl cyclase → ↑ cAMP (e.g., β1 receptor + epinephrine)
- Gi → inhibits adenylyl cyclase → ↓ cAMP (e.g., α2, muscarinic M2)
- Gq → activates phospholipase C → ↑ IP3 + DAG → ↑ Ca²⁺ (e.g., α1, M1, M3)
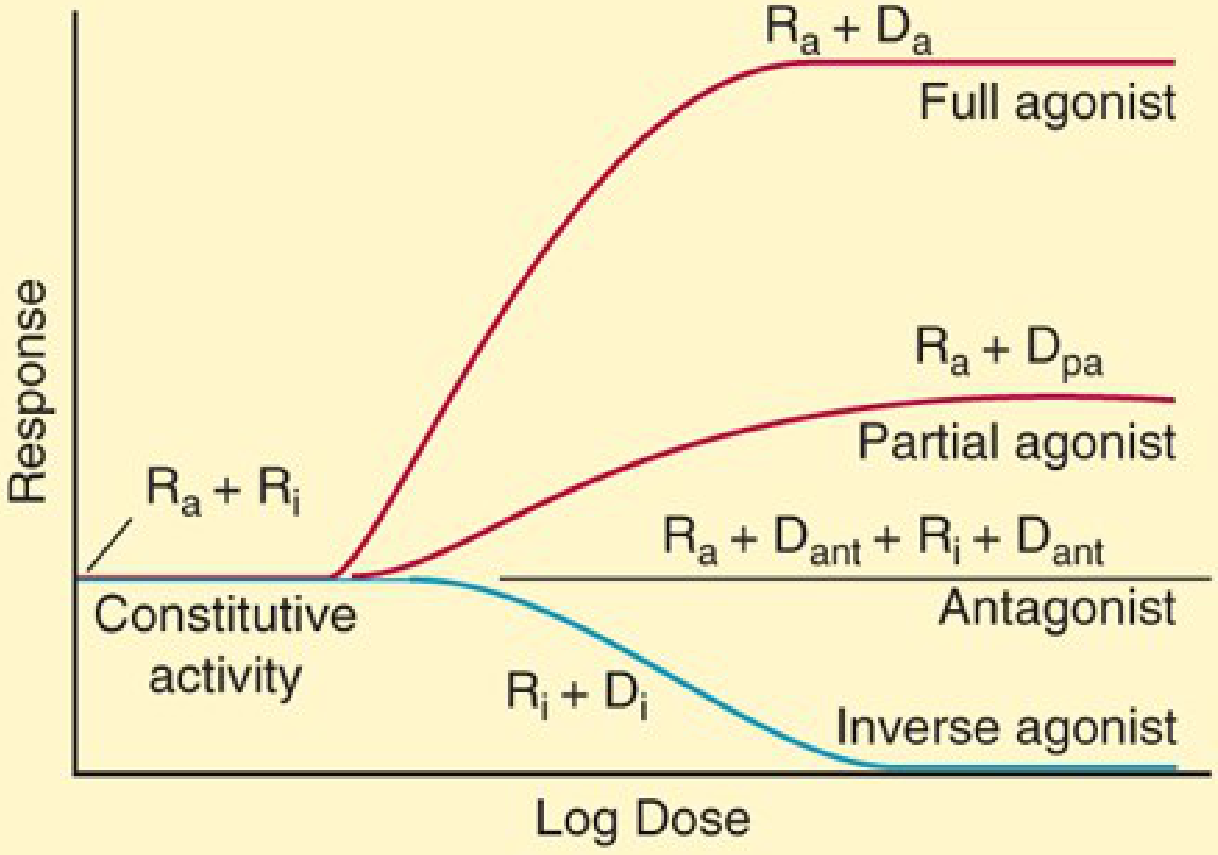
4. Receptor States and Drug Classification
Receptors exist in two states: Inactive (R) and Active (R)*
| Drug Type | Intrinsic Activity | Effect |
|---|---|---|
| Full Agonist | = 1 | Produces maximal response (Emax = 100%). Stabilizes R* |
| Partial Agonist | 0 < IA < 1 | Produces submaximal response even at full occupancy. Can act as antagonist in presence of full agonist |
| Antagonist | = 0 | No response; stabilizes R. Blocks agonist access |
| Inverse Agonist | Negative (-) | Opposite effect to agonist; stabilizes inactive R state; reduces constitutive activity |

NEET PG Classic Examples:
- Full agonist: Morphine at μ-opioid receptor, Phenylephrine at α1
- Partial agonist: Buprenorphine (μ-opioid), Pindolol (β-receptor), Buspirone (5-HT1A)
- Competitive antagonist: Atropine (muscarinic), Flumazenil (benzodiazepine receptor), Naloxone (opioid)
- Inverse agonist: Beta-carbolines at GABA-A receptor
Constitutive activity = Receptor activity even without agonist binding. Inverse agonists reduce this; standard antagonists do not.
5. Types of Antagonism
A. Competitive (Surmountable) Antagonism
- Antagonist competes reversibly at the same site as agonist
- Adding more agonist can overcome the block
- Effect on dose-response curve: Shifts curve to the RIGHT (increases EC50), but Emax is UNCHANGED
- Examples: Atropine, propranolol, naloxone, flumazenil
B. Non-competitive (Insurmountable) Antagonism
- Antagonist binds irreversibly OR at allosteric site
- Cannot be overcome by increasing agonist
- Effect on dose-response curve: REDUCES Emax (depresses the ceiling); NO rightward shift
- Examples: Phenoxybenzamine (α-blocker), alkylating agents
C. Allosteric Modulation
- Drug binds to a site different from the agonist binding site
- Can enhance OR reduce agonist effect
- Allosteric inhibition is NOT overcome by increasing agonist
"Allosteric inhibition is not usually overcome by increasing the dose of agonist." - Katzung's Basic and Clinical Pharmacology
6. Dose-Response Curves
Graded Dose-Response Curve
- Continuous range of responses in a single individual
- Used to measure potency and efficacy
Potency = Dose required to produce a given effect (measured by EC50 = concentration that produces 50% of maximal effect)
- Lower EC50 = More potent drug
- A more potent drug does NOT mean a better or safer drug
Efficacy (Emax) = Maximum response a drug can produce regardless of dose
- Reflects the drug's intrinsic activity
NEET PG Key Distinction:
- Two drugs can have the same efficacy but different potencies
- A partial agonist has LOWER efficacy than a full agonist, even if it has higher potency (lower EC50)
Quantal Dose-Response Curve
- All-or-none response in a population (responded vs. not)
- Used to determine ED50, TD50, LD50
| Parameter | Definition |
|---|---|
| ED50 | Dose effective in 50% of population |
| TD50 | Dose producing toxicity in 50% |
| LD50 | Dose lethal in 50% (animal studies) |
| Therapeutic Index (TI) | TD50 / ED50 |
"A drug with a high therapeutic index is safer than a drug with a low or narrow therapeutic index." - Schwartz's Principles of Surgery
Narrow TI drugs (high-yield for NEET PG): Digoxin, lithium, warfarin, phenytoin, theophylline, aminoglycosides, cyclosporine
7. Spare Receptors (Silent Receptors)
- Maximal effect is achieved when only a fraction of total receptors are occupied
- The remaining unoccupied receptors are "spare"
- Spare receptors increase SENSITIVITY (leftward shift of dose-response curve) but do NOT increase Emax
- They allow a rapid, amplified response at low drug concentrations
NEET PG MCQ pattern:
"A maximal effect of epinephrine is seen when only a portion of β-adrenergic receptors are occupied" = Spare receptors present ✓
8. Receptor Regulation
| Process | Trigger | Effect |
|---|---|---|
| Desensitization / Tachyphylaxis | Overactivation (chronic agonist) | Decreased response to agonist - receptor becomes uncoupled |
| Downregulation | Chronic agonist exposure | Decreased RECEPTOR NUMBER (internalization) |
| Upregulation | Chronic antagonist exposure (receptor blockade) | Increased receptor number - explains withdrawal/supersensitivity |
Clinical examples:
- Beta-blocker withdrawal → upregulated β-receptors → rebound tachycardia/angina
- Chronic opioid use → desensitization → tolerance
- Chronic levodopa in Parkinson's → downregulation → wearing off
9. Signal Transduction - Key Concepts
Signal Amplification: A single receptor binding event triggers a cascade → cellular effects last longer than the drug-receptor binding itself.
- Example: Albuterol dissociates from β2 receptor in milliseconds but bronchodilation lasts much longer due to cAMP second messenger effects
Second Messenger Systems:
- cAMP pathway (β-receptors → adenylyl cyclase → PKA)
- IP3/DAG pathway (Gq-coupled → PLC → Ca²⁺ release)
- cGMP pathway (NO → guanylyl cyclase → PKG - vasodilation)
10. Drug Affinity
- Kd (dissociation constant): Concentration of drug at which 50% of receptors are occupied
- Low Kd = High affinity (inverse relationship)
- Higher affinity → drug binds at lower concentrations
11. Quick NEET PG MCQ Traps
| Scenario | Answer |
|---|---|
| Competitive antagonist added → curve shifts right, Emax unchanged | Competitive (surmountable) antagonism |
| Drug reduces Emax regardless of agonist dose | Non-competitive (insurmountable) antagonism |
| Drug acts at the same receptor but produces OPPOSITE effect | Inverse agonist |
| Drug has partial effect alone but blocks a full agonist when given together | Partial agonist acting as partial antagonist |
| Flumazenil at benzodiazepine receptor (no intrinsic effect, reversible) | Competitive antagonist |
| Phenoxybenzamine at α-receptor (binds irreversibly) | Non-competitive antagonist |
| Chronic propranolol use stopped abruptly → rebound tachycardia | Receptor upregulation |
| Maximal effect even with partial receptor occupancy | Spare receptors present |
Sources
- Lippincott Illustrated Reviews: Pharmacology, Chapter 2 (Drug-Receptor Interactions and Pharmacodynamics)
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 1-2
- Schwartz's Principles of Surgery, 11th Edition, p. 2057
This is a shared conversation. Sign in to Orris to start your own chat.