Coal worker pneumoconiosis full details for md exams 15marks answer full details comprehensive answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coal worker pneumoconiosis" AND pathology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks (Robbins, Harrison's, Fishman's, Grainger & Allison, Washington Manual). I have enough to write a complete, exam-worthy 15-mark answer. Let me compose it now.
Coal Worker's Pneumoconiosis (CWP) — Comprehensive MD Exam Answer
Definition & Overview
Coal Worker's Pneumoconiosis (CWP), colloquially called "black lung disease", is a progressive fibrotic lung disease caused by chronic inhalation of coal mine dust (predominantly carbon, with variable amounts of silica, kaolin, mica, and other minerals). It is classified under the pneumoconioses — a group of lung diseases caused by inhalation of inorganic dusts with subsequent tissue reaction.
"Occupational exposure to coal dust can lead to CWP, which has enormous social, economic, and medical significance in every nation in which coal mining is an important industry." — Harrison's Principles of Internal Medicine, 22E
Epidemiology
- Simple CWP (radiographic evidence) occurs in ~10% of all coal miners and up to 50% of anthracite miners with >20 years of coal-face work
- Prevalence is lower in bituminous than anthracite coal miners (anthracite has higher silica content)
- Exposure required: typically 15–20 years
- Currently resurging in Appalachian coal miners in the USA due to increased mechanization and narrower coal veins with more silica contamination — cases of PMF are rising at an alarming rate
- The U.S. lowered permissible dust limits to 1.5 mg/m³
- Coal accounts for ~30% of global energy production, so occupational exposure remains high worldwide
Etiological Factors / Determinants of Disease
Factors influencing disease development (Robbins):
| Factor | Details |
|---|---|
| Dust concentration & duration | Higher ambient dust load, longer exposure → greater risk |
| Particle size | 1–5 µm particles are most dangerous — reach terminal airways and alveoli |
| Particle solubility | Low solubility → persists in lung parenchyma → fibrosing pneumoconiosis |
| Silica content | Contaminating crystalline silica in coal dust is the most important accelerant to PMF |
| Rank of coal | Anthracite > bituminous > lignite in risk |
| Cigarette smoking | Additive (not synergistic) with coal dust; impairs mucociliary clearance |
| Genetic predisposition | Only a minority of equally exposed workers develop disease |
| Inflammasome activation | Macrophage phagocytosis of particles activates inflammasome → IL-1β, IL-18 release |
Pathogenesis (Mechanism)
Coal dust inhalation (particles 1–5 µm)
↓
Deposition in respiratory bronchioles and alveoli
↓
Phagocytosis by alveolar macrophages
↓
Inflammasome (NLRP3) activation
↓
Release of IL-1β, IL-18, TNF-α, reactive oxygen species (ROS)
↓
Recruitment of neutrophils, lymphocytes → inflammatory cascade
↓
Fibroblast activation → collagen deposition
↓
Macrophage-laden dust particles migrate via lymphatics to
respiratory bronchioles, interstitium, hilar lymph nodes
↓
Coal macule → coal nodule (simple CWP)
↓ (if silica present or high dust load)
Coalescence → Progressive Massive Fibrosis (PMF)
Key points:
- Carbon itself is not highly fibrogenic; silica contamination drives PMF
- Studies show complicated lesions contain much more dust than simple lesions
- Tobacco smoke exacerbates all effects by impairing clearance
- Some particles reach lymph nodes → adaptive immune response → amplification of local reaction
Pathological Spectrum / Classification
CWP exists on a spectrum with three stages:
Stage 1: Anthracosis
- Most innocuous; also seen in urban dwellers and smokers
- Inhaled carbon pigment engulfed by macrophages
- Macrophages accumulate in connective tissue along pulmonary and pleural lymphatics and in hilar lymph nodes
- No cellular reaction, no fibrosis, no functional impairment
Stage 2: Simple CWP
Coal Macules (1–2 mm):
- Collections of carbon-laden macrophages (no significant collagen)
- Located adjacent to respiratory bronchioles (initial site of dust accumulation)
- Upper lobes and upper zones of lower lobes predominantly
Coal Nodules (up to a few mm):
- Macrophages + delicate network of collagen fibers
- Dilation of adjacent alveoli → centrilobular emphysema
Stage 3: Complicated CWP = Progressive Massive Fibrosis (PMF)
- Occurs on background of simple CWP; coalescence of coal nodules
- Lesions >1 cm, often multiple, up to 10 cm in diameter
- Located in upper lobes bilaterally, perihilar
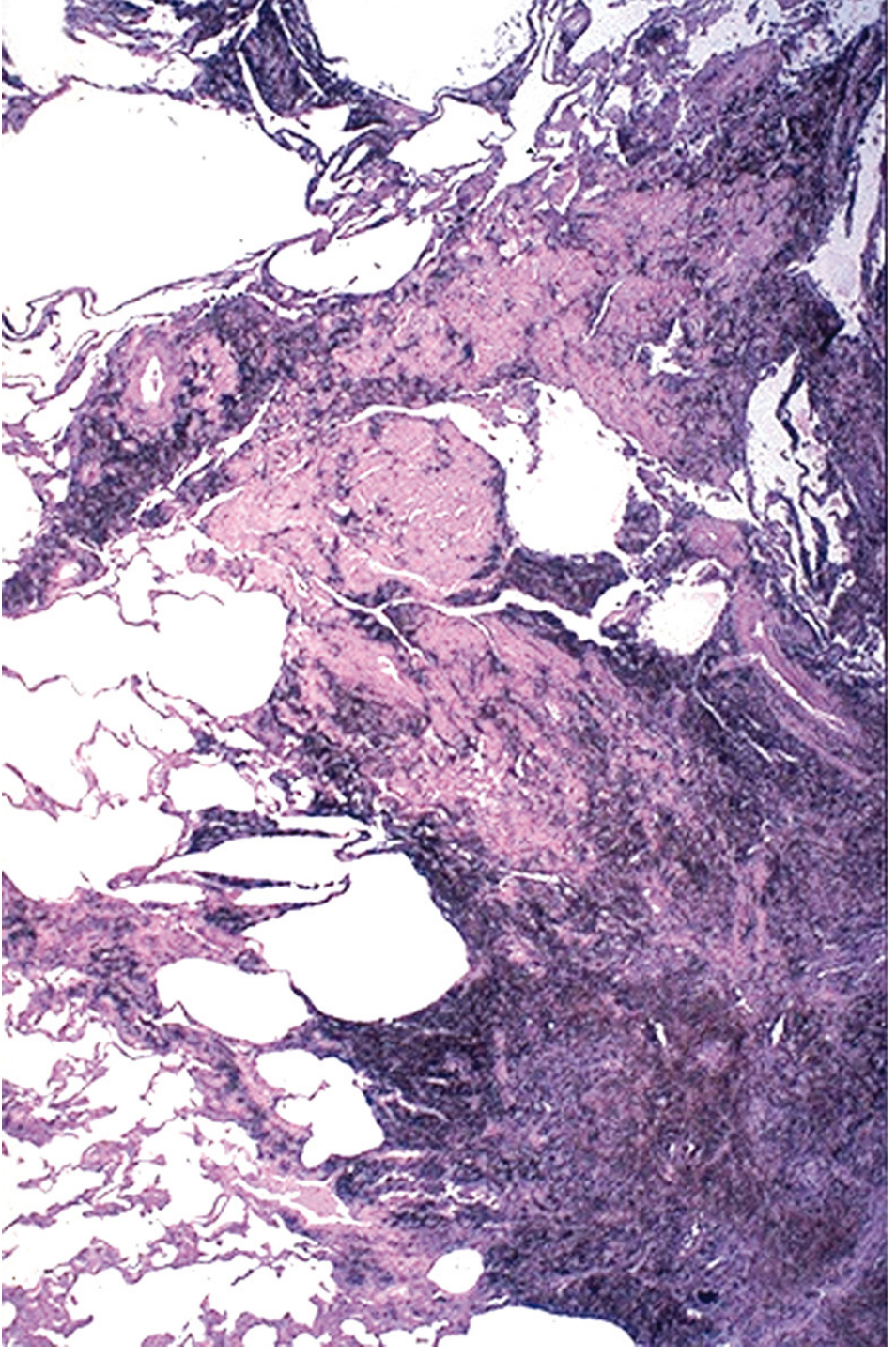
- Gross: intensely black scars with dense collagen + pigment
- Microscopy: Dense collagen + coal pigment; centers often necrotic (ischemia, not cavitation per se)
- Frank cavitation → always consider tuberculosis or atypical mycobacteria in differential
"Complicated coal workers' pneumoconiosis (progressive massive fibrosis) is characterized by intensely blackened scars 1 cm or larger, sometimes up to 10 cm in greatest diameter. The center of the lesion is often necrotic, most likely due to local ischemia." — Robbins & Cotran Pathologic Basis of Disease
Histology image — PMF in a coal worker (dense collagen + black pigment, Robbins):
Clinical Features
Simple CWP
- Usually asymptomatic; discovered incidentally on chest X-ray
- No significant pulmonary function impairment
- Miners may develop chronic bronchitis and COPD independent of CWP (coal dust itself causes this, additive to smoking)
Complicated CWP / PMF
- Progressive exertional dyspnoea → dyspnoea at rest
- Productive cough (melanoptysis — black sputum, pathognomonic)
- Cor pulmonale (right heart failure) from pulmonary hypertension
- Severe restrictive ± obstructive lung function deficits
- Premature mortality
- PMF continues to progress even after cessation of exposure — important exam point
- No significantly increased susceptibility to tuberculosis (unlike silicosis) — though monitoring is still advised
Caplan Syndrome
- First described in coal miners, subsequently also in silicosis patients
- Combination of: pneumoconiotic nodules + seropositive rheumatoid arthritis
- Also called rheumatoid pneumoconiosis
- Nodules in Caplan syndrome are larger (0.5–5 cm), appear rapidly, may cavitate, and can precede joint disease
- Immunological basis: rheumatoid factor + coal dust → exaggerated immune response
Investigations
Chest X-Ray (CXR) — ILO Classification
The International Labour Organisation (ILO) International Classification of Radiographs of Pneumoconioses is the standard tool:
| Feature | Simple CWP | Complicated CWP (PMF) |
|---|---|---|
| Opacities | Small, rounded opacities, 1–10 mm | Large opacities >1 cm (category A), >2 cm (B), >1/3 lung (C) |
| Size | p (up to 1.5 mm), q (1.5–3 mm), r (3–10 mm) | Masses >1 cm, may be bilateral |
| Distribution | Upper and mid zones, bilateral | Upper lobes, posterior, perihilar |
| Nodes | Hilar enlargement ± "eggshell" calcification | May be elevated/retracted |
| Special | Nodules smaller than silicosis | Migrate toward hila over time |
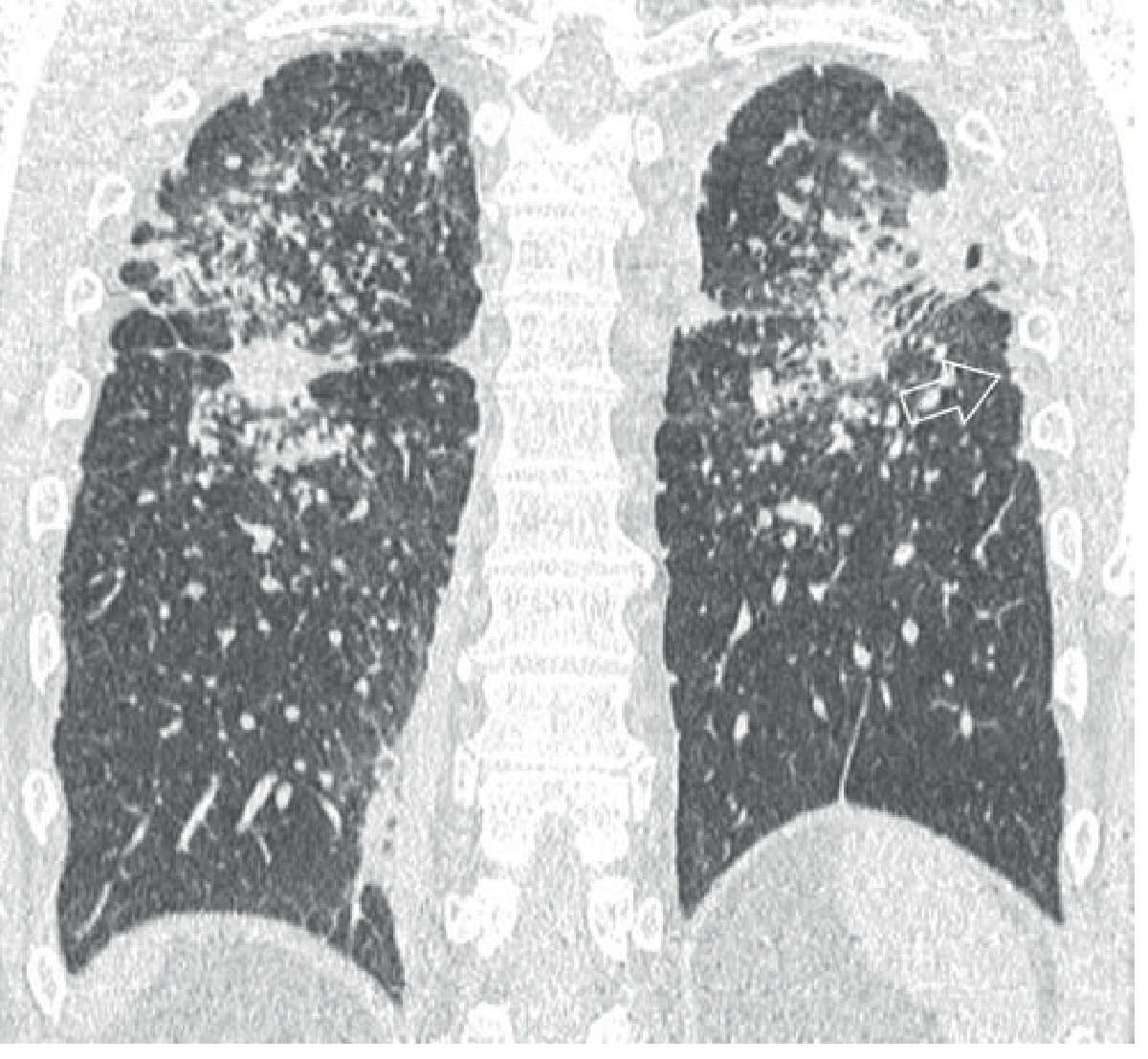
HRCT Chest (more sensitive than CXR):
- Well-defined, dense centrilobular and subpleural nodules, upper and posterior lung predominance
- Hilar and mediastinal lymph node enlargement ± calcification
- PMF: irregular upper lobe masses with surrounding emphysema; migrate toward hila
- Large PMF (>5 cm) show irregular low-attenuation regions indicating necrosis
- Peripheral traction emphysema adjacent to PMF masses — characteristic "pseudo-plaque" formation
CT image — PMF in CWP (bilateral upper lobe mass opacities with surrounding nodules and pseudo-plaques):
Pulmonary Function Tests (PFTs):
- Simple CWP: usually normal
- PMF: Restrictive pattern (↓FVC, ↓TLC) ± obstructive component
- ↓DLCO (diffusion capacity)
- Monitoring: FEV₁, FVC, FEV₁/FVC, MVV, ABG (for disability assessment)
Other:
- No specific blood tests for diagnosis
- Biopsy (rarely needed): tissue shows coal pigment + fibrosis
- CT more sensitive than CXR for early detection and monitoring
Differences: CWP vs Silicosis
| Feature | CWP | Silicosis |
|---|---|---|
| Causative dust | Coal (carbon ± silica) | Crystalline silica (quartz) |
| Nodule size on CXR | Smaller | Larger |
| PMF | Less common | More common |
| Eggshell calcification | Less common | More characteristic |
| TB susceptibility | Not significantly increased | Markedly increased |
| Lung cancer | Not increased (unless smoky coal domestic use) | Increased (IARC: probable carcinogen) |
| Autoimmune | Caplan syndrome | Rheumatoid arthritis, scleroderma |
| Pathology | Coal macules, nodules, mild collagen | Silicotic nodule — laminated/whorled collagen, birefringent particles |
Complications
- Progressive Massive Fibrosis (PMF) — occurs in <10% of simple CWP
- Cor pulmonale — pulmonary hypertension → right heart failure
- COPD / Emphysema (centrilobular) — independent of smoking
- Caplan syndrome — rheumatoid pneumoconiosis
- Respiratory failure — end-stage PMF
- Non-tuberculous mycobacterial infections (less common than silicosis)
- Melanoptysis (black sputum) — pathognomonic
Management
There is no specific curative treatment for CWP. Management is:
Primary: Dust Control (Prevention)
- Reduce coal mine dust below permissible exposure limits (1.5 mg/m³ in USA)
- Water sprays, ventilation, enclosed cabs
- Respiratory protective equipment (RPE) where engineering controls insufficient
- Dust measurement and surveillance — NIOSH Coal Workers' X-ray Surveillance Program
Secondary: Medical Surveillance
- Periodic chest radiographs (ILO classification) + PFTs for all coal miners
- Early detection → removal from exposure → prevent progression
- Workers with CWP should be transferred away from dusty environments
Tertiary: Symptomatic Treatment
| Condition | Treatment |
|---|---|
| COPD/airflow obstruction | Bronchodilators (LABA, LAMA), inhaled corticosteroids |
| Hypoxia | Supplemental oxygen (long-term O₂ therapy) |
| Pulmonary hypertension | Pulmonary vasodilators (limited evidence) |
| Cor pulmonale | Diuretics, O₂, treat underlying cause |
| Smoking | Smoking cessation (counselling + pharmacotherapy) |
| Respiratory infections | Prompt antibiotic treatment; influenza & pneumococcal vaccination |
| End-stage disease | Lung transplantation (selected cases) |
- PMF does not reverse even with dust cessation
- Whole lung lavage (used in alveolar proteinosis) has no proven benefit in CWP
Legal / Compensation:
- Black Lung Benefits Act (USA, 1972): eligibility based on radiographic evidence, PFT criteria, cor pulmonale, or total disability
- Disability criteria: Department of Labor FEV₁, FVC, MVV, ABG thresholds; presence of cor pulmonale; radiographic complicated CWP/PMF
Prevention
- Engineering controls: Dust suppression (wet drilling, ventilation, enclosed cabs)
- Administrative controls: Job rotation, reduced shift lengths in dusty environments
- Surveillance: Mandatory periodic chest X-ray and spirometry for all underground miners
- Regulatory enforcement: Strict permissible exposure limits (PEL)
- Education and training: Workers informed of risks, safe practices
- Smoking cessation: Reduces additive impairment
- Early worker removal from dusty environments on diagnosis
Key Exam Points (Summary Mnemonics)
Spectrum (ASCP):
- Anthracosis (innocuous, urban dwellers too)
- Simple CWP (macules + nodules, upper zones, centrilobular emphysema)
- Complicated CWP / PMF (>1 cm scars, upper lobes, central necrosis)
- Progresses even after dust cessation
Complications (5C):
- COPD / Emphysema
- Cor pulmonale
- Caplan syndrome
- Cavitation (consider TB/NTM)
- Carbon sputum = melanoptysis
Differences from silicosis (TB-CA):
- TB not increased in CWP (increased in silicosis)
- Cancer risk not increased in CWP (increased in silicosis)
- Anthracite > bituminous in risk
Sources
- Harrison's Principles of Internal Medicine, 22E (2025) — Ch. 300, p. 2281
- Robbins & Cotran Pathologic Basis of Disease — Ch. 15, pp. 647–648
- Fishman's Pulmonary Diseases & Disorders — Ch. 87, pp. 1545–1548
- Grainger & Allison's Diagnostic Radiology — p. 244–245
- Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.