15 most common ecg in daily practice
Reading File
Finding Sources
Searching the Web
15 most common ECG patterns daily clinical practice interpretation
Finding Sources
Finding Sources
Reading Web Page
https://tricog.com/common-ecg-patterns/?srsltid=AfmBOorEknmg…
Finding Sources
Finding Sources
Searching Images
normal sinus rhythm ECG electrocardiogram
Searching Images
atrial fibrillation ECG irregularly irregular rhythm
Searching Images
STEMI ST elevation myocardial infarction ECG
Finding Sources
Searching Images
ventricular fibrillation ECG chaotic rhythm cardiac arrest
Searching Images
left bundle branch block LBBB ECG wide QRS
Searching Images
atrial flutter sawtooth waves ECG
Searching Images
ventricular tachycardia wide complex tachycardia ECG
Searching Images
complete heart block third degree AV block ECG pacemaker rhythm
Searching Images
Wolff-Parkinson-White syndrome delta wave short PR ECG
I now have comprehensive image data and clinical knowledge to deliver a thorough, well-illustrated guide. Let me compile the full response.
15 Most Common ECGs in Daily Practice
A systematic reference covering the key ECG patterns every clinician encounters, with diagnostic features and clinical pearls.
ECG Basics — Quick Reference
| Parameter | Normal Value |
|---|---|
| Rate | 60–100 bpm |
| PR interval | 120–200 ms (3–5 small squares) |
| QRS duration | < 120 ms (< 3 small squares) |
| QT interval (corrected) | < 440 ms (men), < 460 ms (women) |
| P wave | Upright in I, II; inverted in aVR |
1. Normal Sinus Rhythm
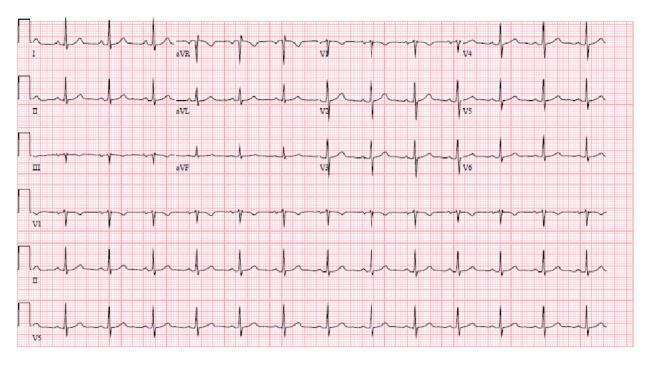
Key features:
- Rate 60–100 bpm, regular
- P wave before every QRS (upright in I and II, inverted in aVR)
- PR interval 120–200 ms, consistent
- Narrow QRS < 120 ms
- Normal R-wave progression V1→V6
Clinical significance: The baseline to compare all abnormalities against. Confirm it before calling anything "sinus."
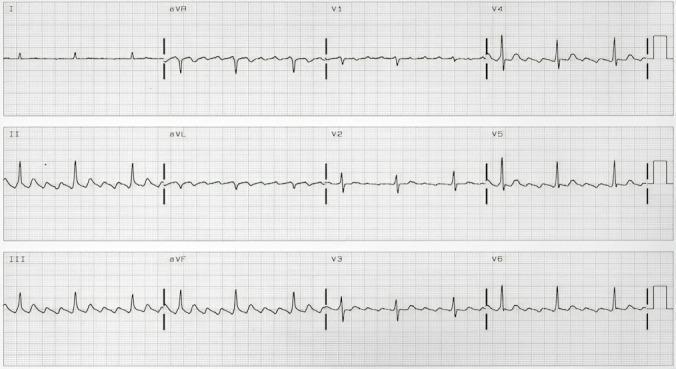
2. Atrial Fibrillation (AF)

Key features:
- Irregularly irregular R-R intervals (most important clue)
- No discrete P waves — replaced by fibrillatory (f) waves, best seen in V1 and II
- Narrow QRS (unless aberrant conduction or WPW)
- Ventricular rate typically 100–160 bpm if uncontrolled
Clinical significance: Most common sustained arrhythmia. Risk of stroke, heart failure. Requires rate/rhythm control and anticoagulation assessment (CHA₂DS₂-VASc).
"After sinus tachycardia, atrial fibrillation is the next most frequent narrow-complex tachycardia encountered in the ED." — Tintinalli's Emergency Medicine
3. Atrial Flutter
Key features:
- Sawtooth flutter waves (F-waves) at ~300 bpm, best in II, III, aVF
- Regular ventricular rhythm with fixed AV conduction ratio (usually 2:1 → ventricular rate ~150 bpm)
- Absent isoelectric baseline between flutter waves
- Narrow QRS unless aberrant
Clinical tip: A narrow-complex tachycardia at exactly 150 bpm should always raise suspicion for 2:1 flutter. Use adenosine or carotid sinus massage to unmask the flutter waves.
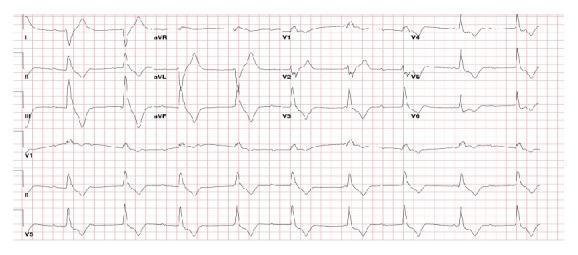
4. ST-Elevation Myocardial Infarction (STEMI)

Key features:
- New ST elevation ≥ 1 mm in ≥ 2 contiguous limb leads, OR ≥ 2 mm in ≥ 2 contiguous precordial leads
- Convex ("tombstone") or straight ST morphology
- Reciprocal ST depression in opposing leads
- Evolving Q waves, T-wave inversion over hours
Territory localization:
| Leads with STE | Territory | Culprit artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA (80%) or LCx |
| I, aVL, V5–V6 | Lateral | LCx or diagonal |
| V1–V4 + I, aVL | Anterolateral | Proximal LAD |
Clinical significance: Time-critical emergency. Activate cath lab immediately. Door-to-balloon < 90 min.
5. Sinus Tachycardia
Key features:
- Rate > 100 bpm, regular
- Normal P wave morphology preceding every QRS
- Rate gradually increases/decreases (not abrupt onset like SVT)
- Rate typically 100–150 bpm
Common causes: Pain, fever, hypovolemia, anemia, anxiety, thyrotoxicosis, pulmonary embolism, heart failure. Treat the cause, not the rate.
6. Sinus Bradycardia
Key features:
- Rate < 60 bpm, regular
- Normal P wave before every QRS
- Normal PR and QRS
Common causes: Athletic conditioning, vasovagal syncope, hypothyroidism, inferior MI (RCA → SA node), beta-blockers, sleep. Intervene only if symptomatic (dizziness, syncope, hemodynamic compromise).
7. Ventricular Tachycardia (VT)

Key features:
- Wide QRS > 120 ms at rate > 100 bpm
- Regular rhythm, monomorphic (uniform QRS shape)
- AV dissociation (P waves independent of QRS) — pathognomonic when seen
- Fusion beats and capture beats (Dressler beats) — diagnostic
- Concordance across precordial leads (all positive or all negative)
Brugada criteria: If wide-complex tachycardia of uncertain origin → treat as VT until proven otherwise. VT is far more common than SVT with aberrancy.
8. Ventricular Fibrillation (VF)

Key features:
- Chaotic, irregular, disorganized waveform
- No identifiable P waves, QRS complexes, or T waves
- Variable amplitude oscillations (coarse vs. fine VF)
- Patient is pulseless/unresponsive
Clinical significance: Cardiac arrest. Immediate defibrillation + CPR. Shockable rhythm alongside pulseless VT.
9. Left Bundle Branch Block (LBBB)

Key features:
- QRS > 120 ms
- Broad, notched ("M-shaped") R waves in I, aVL, V5, V6
- Deep QS or rS in V1 (no septal q in lateral leads)
- Discordant ST-T changes (T-wave opposite to QRS)
- New LBBB in the context of chest pain = treat as STEMI equivalent
Sgarbossa criteria help identify MI in the context of LBBB:
- Concordant STE ≥ 1 mm (5 points)
- Concordant ST depression ≥ 1 mm in V1–V3 (3 points)
- Discordant STE ≥ 5 mm (2 points) — score ≥ 3 is specific for MI
10. Right Bundle Branch Block (RBBB)
Key features:
- QRS > 120 ms
- RSR' ("bunny ears") in V1–V2
- Wide, slurred S waves in I, aVL, V5–V6
- T-wave inversion in V1–V3 (secondary repolarization change — normal)
- Incomplete RBBB: same pattern but QRS 100–120 ms
Clinical significance: Can be normal variant. New RBBB with anterior STE suggests proximal LAD occlusion (Sgarbossa). Also seen in pulmonary embolism (S₁Q₃T₃ + RBBB).
11. Complete (Third-Degree) AV Block
Key features:
- Complete AV dissociation — P waves and QRS complexes march independently
- Atrial rate faster than ventricular rate
- Regular escape rhythm (junctional: narrow QRS ~40–60 bpm; ventricular: wide QRS ~20–40 bpm)
- No conducted beats
Clinical significance: Requires urgent transvenous pacing or permanent pacemaker. Causes: inferior MI (often transient), anterior MI (severe, requires PPM), Lyme disease, digoxin toxicity, fibrosis.
12. Wolff-Parkinson-White (WPW) Syndrome

Key features:
- Short PR interval < 120 ms
- Delta wave — slurred initial upstroke of QRS
- Widened QRS (pseudo-bundle branch block morphology)
- Secondary ST-T changes ("pseudoinfarction" Q waves in inferior leads)
Clinical significance: Risk of sudden death if AF develops (rapid conduction via accessory pathway → VF). Never use AV nodal blocking agents (adenosine, verapamil, diltiazem, digoxin) in WPW + AF — this accelerates accessory pathway conduction. Use procainamide or electrical cardioversion.
13. Supraventricular Tachycardia (SVT — AVNRT/AVRT)
Key features:
- Abrupt onset/termination ("paroxysmal")
- Rate 150–250 bpm, perfectly regular
- Narrow QRS (usually)
- P waves absent, buried in QRS, or immediately after QRS (retrograde P waves — "pseudo-R'" in V1, "pseudo-S" in inferior leads)
- No delta wave (differentiates from WPW)
Treatment: Vagal maneuvers → IV adenosine (6 mg rapid push) → verapamil or diltiazem if refractory. Cardiovert if hemodynamically unstable.
14. First-Degree AV Block + Mobitz I/II (Second-Degree AV Block)
First-degree AV block:
- PR interval > 200 ms, every P conducts → benign, no treatment
Mobitz I (Wenckebach):
- Progressive PR lengthening → dropped QRS → cycle repeats
- Usually at AV node level; benign; seen in inferior MI, athletes, high vagal tone
Mobitz II:
- Constant PR interval → sudden non-conducted P wave (no warning)
- Below AV node (His-Purkinje); more dangerous
- May progress to complete heart block → pacemaker consideration
2:1 AV block: Every other P wave blocked; cannot differentiate Mobitz I vs II from single rhythm strip — need longer recording.
15. Pulmonary Embolism Pattern (S₁Q₃T₃ + Sinus Tachycardia)
Classic ECG features of PE:
- Sinus tachycardia — most common finding
- S₁Q₃T₃ — S wave in I, Q wave and T-wave inversion in III
- New RBBB (complete or incomplete)
- Right axis deviation
- T-wave inversions in V1–V4 (right heart strain)
- New AF
Caveat: The S₁Q₃T₃ pattern appears in only ~20% of PE cases. A normal ECG does NOT exclude PE. Sinus tachycardia alone in the right clinical context warrants CT-PA.
Quick Summary Table
| # | Pattern | Rate | Rhythm | Key Feature | Action |
|---|---|---|---|---|---|
| 1 | Normal Sinus Rhythm | 60–100 | Regular | P before every QRS | Baseline |
| 2 | Atrial Fibrillation | Variable | Irregularly irregular | No P waves | Anticoagulate; rate/rhythm control |
| 3 | Atrial Flutter | ~150 (2:1) | Regular | Sawtooth F-waves | Rate control; cardioversion |
| 4 | STEMI | Variable | Usually regular | ST elevation + reciprocal changes | Activate cath lab |
| 5 | Sinus Tachycardia | > 100 | Regular | Normal P wave | Treat cause |
| 6 | Sinus Bradycardia | < 60 | Regular | Normal P wave | Treat if symptomatic |
| 7 | Ventricular Tachycardia | > 100 | Regular | Wide QRS, AV dissociation | ACLS; defibrillate if pulseless |
| 8 | Ventricular Fibrillation | — | Chaotic | No QRS | CPR + defibrillate immediately |
| 9 | LBBB | Variable | Regular | QRS > 120ms, M-waves V5–V6 | New = STEMI equivalent |
| 10 | RBBB | Variable | Regular | RSR' in V1, S in V5–V6 | Rule out PE, anterior STEMI |
| 11 | Complete Heart Block | Atria fast, ventricles slow | Both regular, independent | AV dissociation | Urgent pacing |
| 12 | WPW | Variable | Variable | Short PR, delta wave | Avoid AV blockers in AF |
| 13 | SVT | 150–250 | Regular | Abrupt onset, narrow complex | Vagal → adenosine |
| 14 | 2nd-degree AV block | Variable | Irregular | Dropped beats | Monitor; PPM for Mobitz II |
| 15 | PE Pattern | Usually tachycardia | Regular | S₁Q₃T₃, RBBB, RV strain | CT-PA to confirm |
Key clinical rules to internalize:
- Wide-complex tachycardia → always assume VT first
- Irregularly irregular rhythm → AF until proven otherwise
- HR ~150 → rule out 2:1 flutter
- Short PR + delta wave → WPW — never give AV nodal blockers in tachycardia
- New LBBB + chest pain → manage as STEMI
This is a shared conversation. Sign in to Orris to start your own chat.