Tell me all about dequerian tenosynovitis , its etiology, pathogenesis, characteristics, tests, anatomy and surgical management and surgical approach and everything that need to be know.
Reading File
Finding Sources
Finding Sources
Searching the Web
de Quervain tenosynovitis etiology pathogenesis anatomy surgical management 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from Campbell's Operative Orthopaedics, Miller's Review, Rosen's Emergency Medicine, and multiple key images. Let me compile the complete, definitive answer.
De Quervain Tenosynovitis - Complete Clinical Guide
Overview
De Quervain tenosynovitis (DQT) - also called de Quervain disease - is a stenosing tenosynovitis of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons as they pass through the first dorsal extensor compartment of the wrist at the level of the radial styloid. The tendons become painfully entrapped within a thickened, constricting fibrous sheath. It is the most common tendinopathy of the wrist.
1. Anatomy
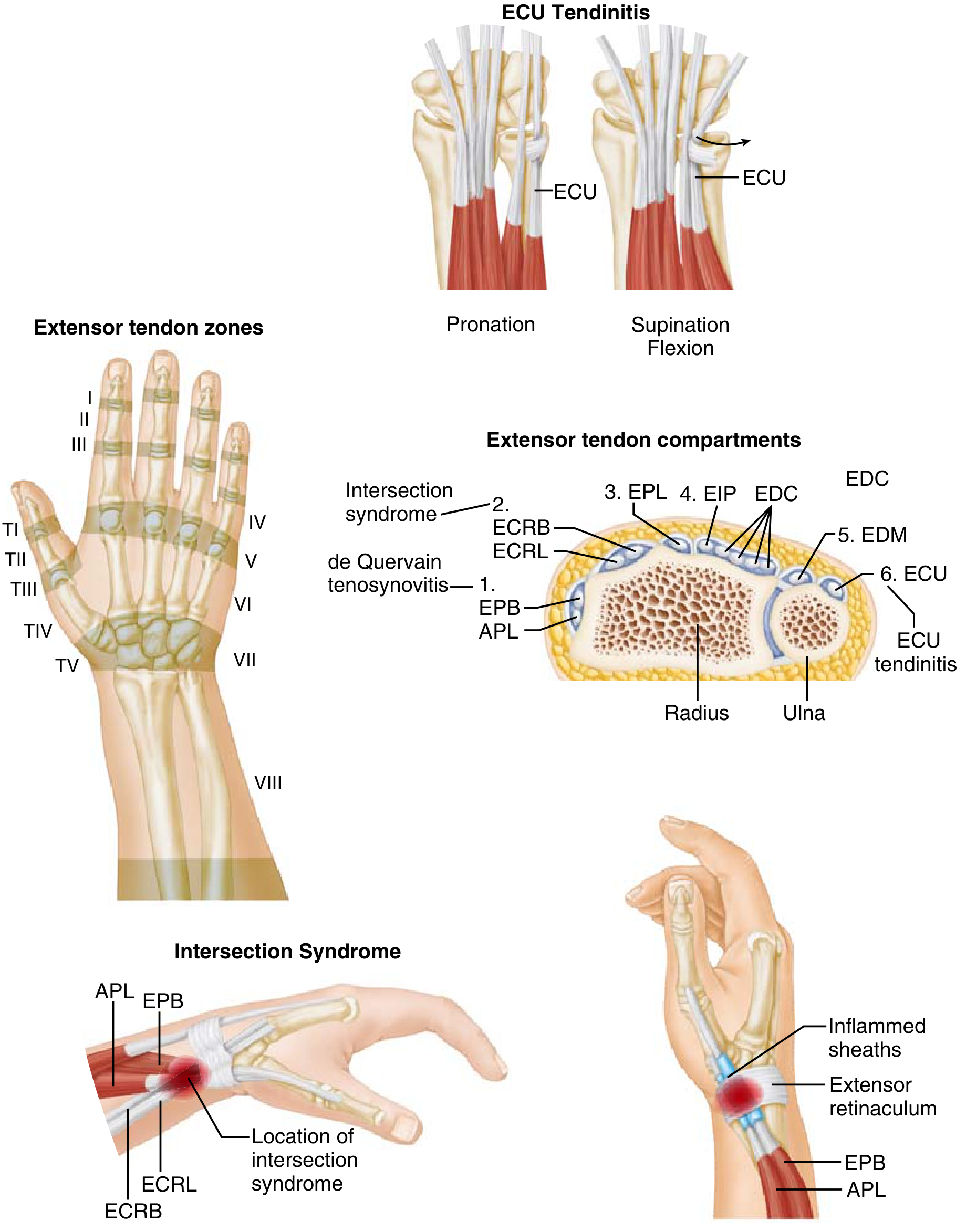
The first dorsal extensor compartment sits on the radial side of the wrist, within a fibroosseous tunnel formed by a groove in the radial styloid (floor) and the extensor retinaculum (roof).
Contents of the 1st dorsal compartment:
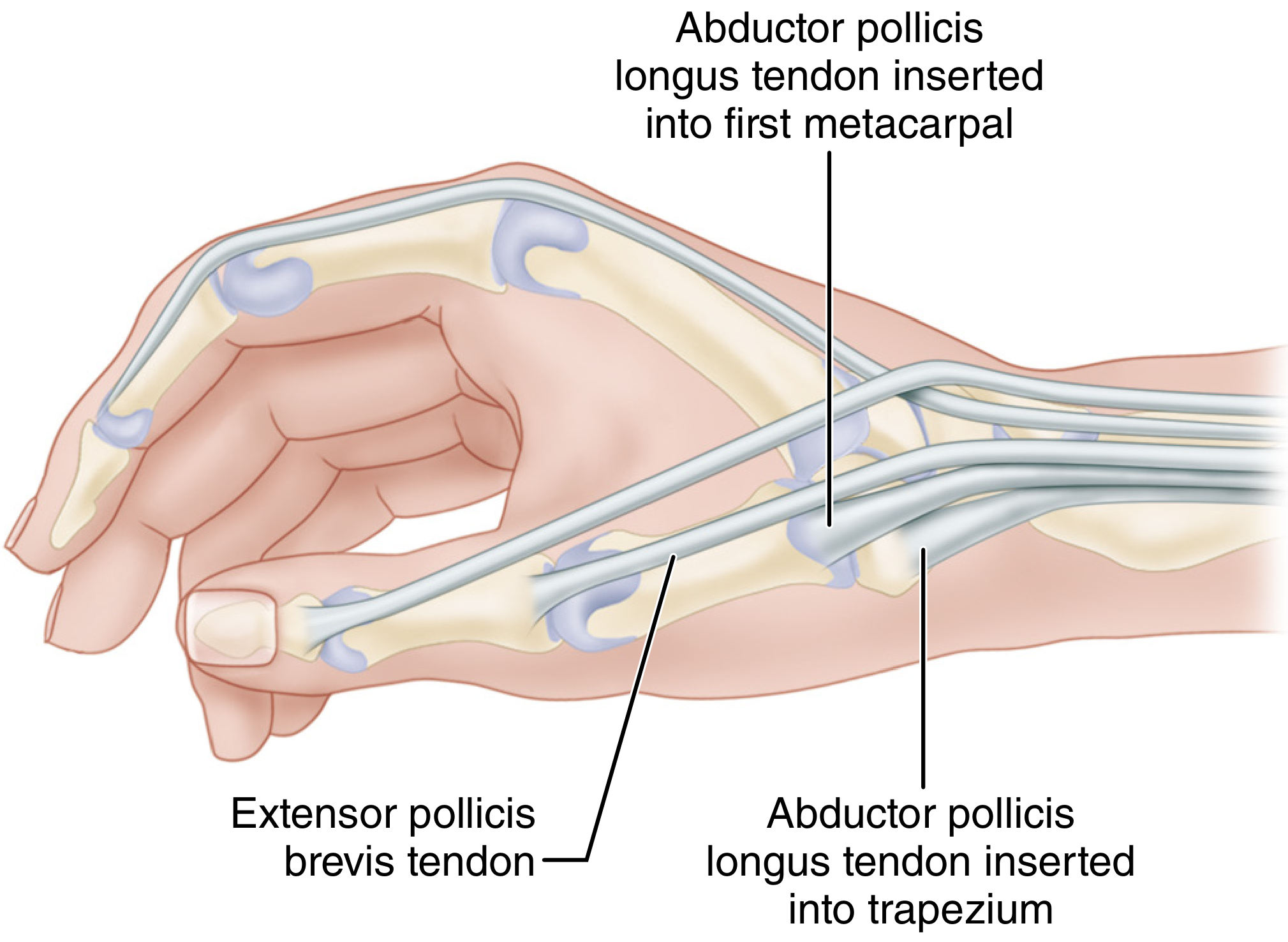
- APL (Abductor Pollicis Longus): Arises from the posterior radius, ulna, and interosseous membrane. Inserts primarily onto the base of the 1st metacarpal but commonly has multiple slips inserting into the trapezium, thenar fascia, or opponens pollicis. It is the more palmar of the two tendons.
- EPB (Extensor Pollicis Brevis): Arises from the posterior radius and interosseous membrane. Inserts onto the base of the proximal phalanx of the thumb. It is the more dorsal tendon and can be identified at surgery by its distally oriented muscle fibers (the APL has no muscular fibers in the distal portion).
Key anatomic variations (surgically critical):
- More than 50% of wrists have "aberrant" or duplicated APL slips; the APL routinely has a thenar fascial slip and may insert onto the trapezium
- The APL may have 2, 3, or even more slips within the compartment
- The EPB may occupy a separate subcompartment (septum present in ~20-34% of wrists) - this is the single most important anatomic variant because failure to release a subcompartment is the most common cause of surgical failure
- The EPB is absent in approximately 5% of wrists
Neurovascular relations:
- The superficial branch of the radial nerve (SBRN) courses superficially and just dorsally - the most feared surgical complication is iatrogenic injury to this nerve
- The lateral antebrachial cutaneous nerve lies above the cephalic vein, more superficially
- The radial artery courses dorsally just beyond the radial styloid, at risk when the floor of the compartment is explored
The relationship to the six extensor compartments:
| Compartment | Contents | Pathology |
|---|---|---|
| 1st | APL, EPB | De Quervain tenosynovitis |
| 2nd | ECRL, ECRB | Intersection syndrome |
| 3rd | EPL | Rupture (Drummer's palsy) |
| 4th | EIP, EDC | - |
| 5th | EDM | - |
| 6th | ECU | ECU tendinitis/instability |
2. Etiology
The precise cause is not fully established, but the condition is attributed to myxoid degeneration with fibrous tissue deposits and increased vascularity in the tendon sheath, rather than acute synovial inflammation. This is why the term "tendinosis" or "tendinopathy" is increasingly preferred over "tenosynovitis."
Tendons may enlarge up to five times their original size, creating a stenosing tendinopathy. (Rosen's Emergency Medicine)
Risk factors:
- Repetitive overuse: Repetitive thumb radial abduction, simultaneous thumb extension, and wrist radial-to-ulnar deviation (e.g., lifting a newborn with radially abducted thumbs)
- Sex: Women affected 6 to 10 times more frequently than men (Campbell's Operative Orthopaedics 15th Ed 2026)
- Age: Peak incidence in adults aged 30-50 years; prevalence ~1.3% in women, 0.5% in men (peak in the 40s-50s)
- Postpartum mothers ("Mommy's wrist" / "Mummy thumb"): A classic demographic - repetitive newborn lifting with wrist going from ulnar to radial deviation
- Occupational factors: Repetitive pinching, grasping, wringing motions (factory workers, musicians, racket-sport athletes, golfers)
- Rheumatoid arthritis and other inflammatory arthropathies
- Pregnancy / hormonal changes: Postulated hormonal influence, particularly in the peripartum period
- Acute wrist trauma can precipitate the condition
- Diabetes mellitus is associated
- "Texting thumb" - increasing recognition in adolescents from smartphone use
3. Pathogenesis
The pathological sequence:
- Repetitive mechanical friction/stress on the APL and EPB tendons within the narrow first dorsal compartment
- Myxoid degeneration of the extensor retinaculum and sheath - fibrous tissue deposits replace normal connective tissue
- Sheath hypertrophy and fibrosis - increased vascularity, collagen disorganization (similar to other tendinopathies; not primarily an inflammatory process)
- Relative stenosis of the fibroosseous tunnel - the enlarged, degenerated sheath compresses the tendons
- Painful tendon entrapment - tendons lose their ability to glide freely, producing pain with any thumb or wrist movement
- Cycle perpetuation - continued movement causes further friction, edema, and fibrosis
This explains why the condition is now conceptualized as a degenerative tendinopathy rather than a purely inflammatory one, and why NSAIDs alone are often insufficient.
4. Clinical Characteristics
Symptoms:
- Gradual onset of pain on the radial side of the wrist, at and just distal to the radial styloid
- Pain radiates proximally up the forearm or distally into the thumb
- Worsened by thumb movements (pinch, grip), wrist ulnar deviation
- Weakened grip strength
- Swelling over the radial styloid
- Occasional "snapping" sensation with thumb movement (crepitus)
Signs:
- Tenderness directly over the first dorsal compartment at the radial styloid - the most consistent finding
- Palpable thickening of the fibrous sheath over the radial styloid
- Swelling over the dorsoradial wrist
- Occasionally, a visible fusiform swelling of the tendon sheath
5. Diagnostic Tests
Finkelstein Test (Most Important)
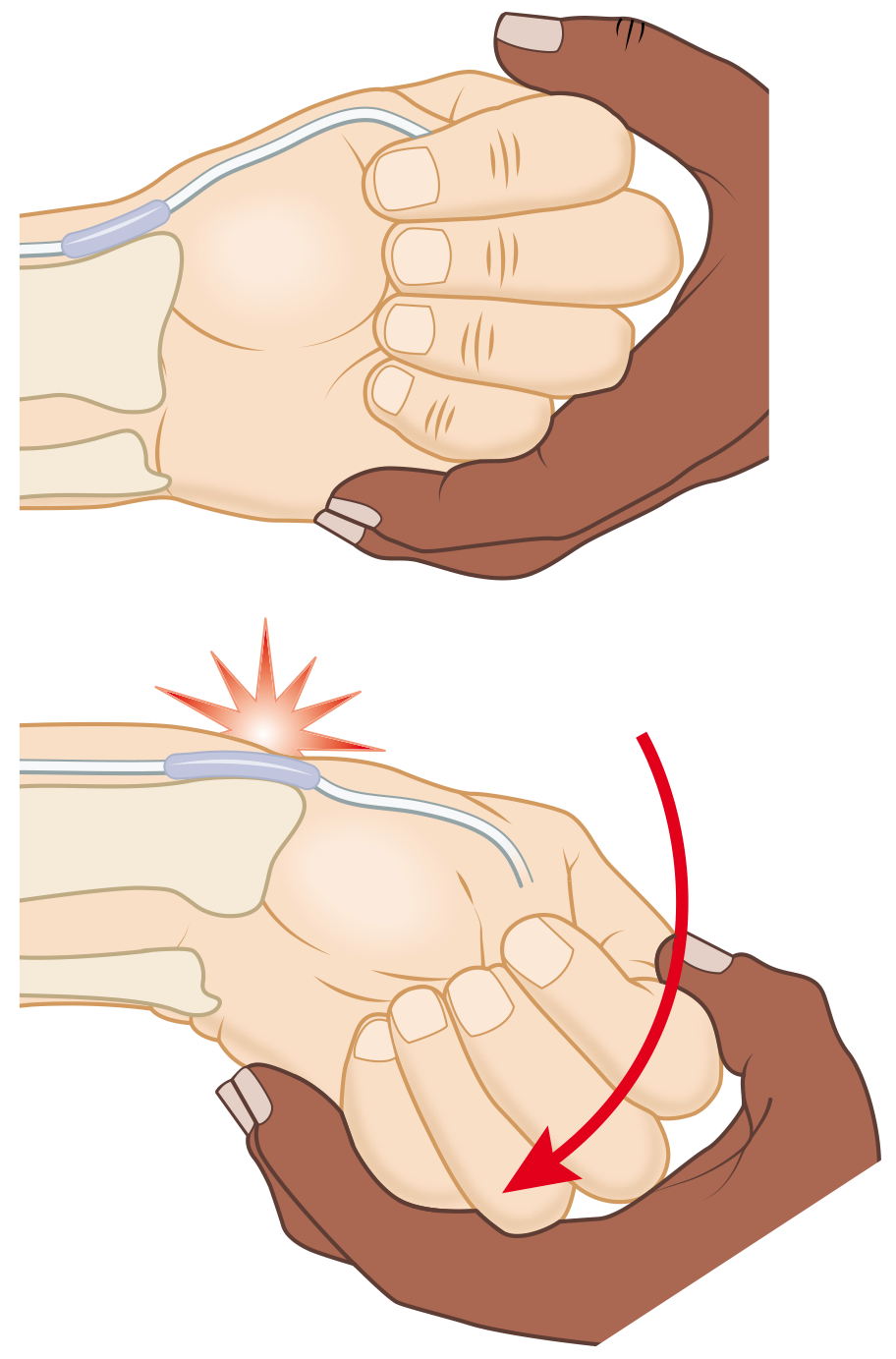
The examiner grasps the patient's thumb and rapidly deviates the hand ulnarward. This places the APL and EPB under maximum tension. A positive test reproduces sharp pain over the radial styloid.
- The Finkelstein test is considered the most pathognomonic objective sign of de Quervain disease (Campbell's)
- However, it is not fully diagnostic in isolation - patient history, occupation, radiographs, and other findings must be considered
- False positives: CMC joint arthritis, scaphoid pathology
Important distinction: The Eichhoff maneuver (patient tucks thumb inside a fist, then ulnar-deviates the wrist) is commonly performed but is slightly different - it stretches the first compartment via thumb position rather than direct traction. Both tests are used and place the compartment tendons under maximum stress.
Radial Synergy Test (newer)
A more recently described test to help confirm the diagnosis (Lee et al., 2023, Hand [N Y]).
Imaging
| Modality | Findings | Role |
|---|---|---|
| Plain X-ray | Usually normal; may show soft-tissue calcifications in first dorsal compartment; rules out osseous pathology (fracture, arthritis) | Rule out differential |
| Ultrasound (US) | Tendon sheath fluid, retinacular/tendon thickening, partial tears; can identify intracompartmental septum | Best for confirming diagnosis and guiding injection; septum detection predicts non-op failure |
| MRI | Peritendinous edema, sheath thickening; identifies septum | Used when US is equivocal or atypical presentation |
Practical note: When clinical presentation and examination are clear, imaging is not required. Ultrasound becomes important when: (1) diagnosis is uncertain after failed conservative management, (2) to guide corticosteroid injection, or (3) to detect a subcompartment septum.
Differential Diagnosis
- Basal joint (1st CMC) arthritis: Grind test (axial loading + rotation of thumb metacarpal) is positive; X-ray shows joint space narrowing
- Intersection syndrome: Pain 4-8 cm proximal to the radial styloid, at the crossing of the 1st and 2nd compartment tendons
- Scaphoid fracture/pathology: Anatomical snuffbox tenderness, history of trauma
- Wartenberg syndrome: Superficial radial nerve entrapment - dysesthesia rather than tendon-related pain
- FCR tendinitis: Volar radial wrist pain
- Trigger thumb: Tenosynovitis of the FPL within the A1 pulley
6. Management
Non-Operative Treatment (First-Line)
Step 1 - Activity Modification + Immobilization:
- Thumb spica splint (immobilizes CMC and MCP joints of the thumb, wrist in slight extension)
- Rest from offending activities
- NSAIDs (oral or topical)
Step 2 - Corticosteroid Injection:
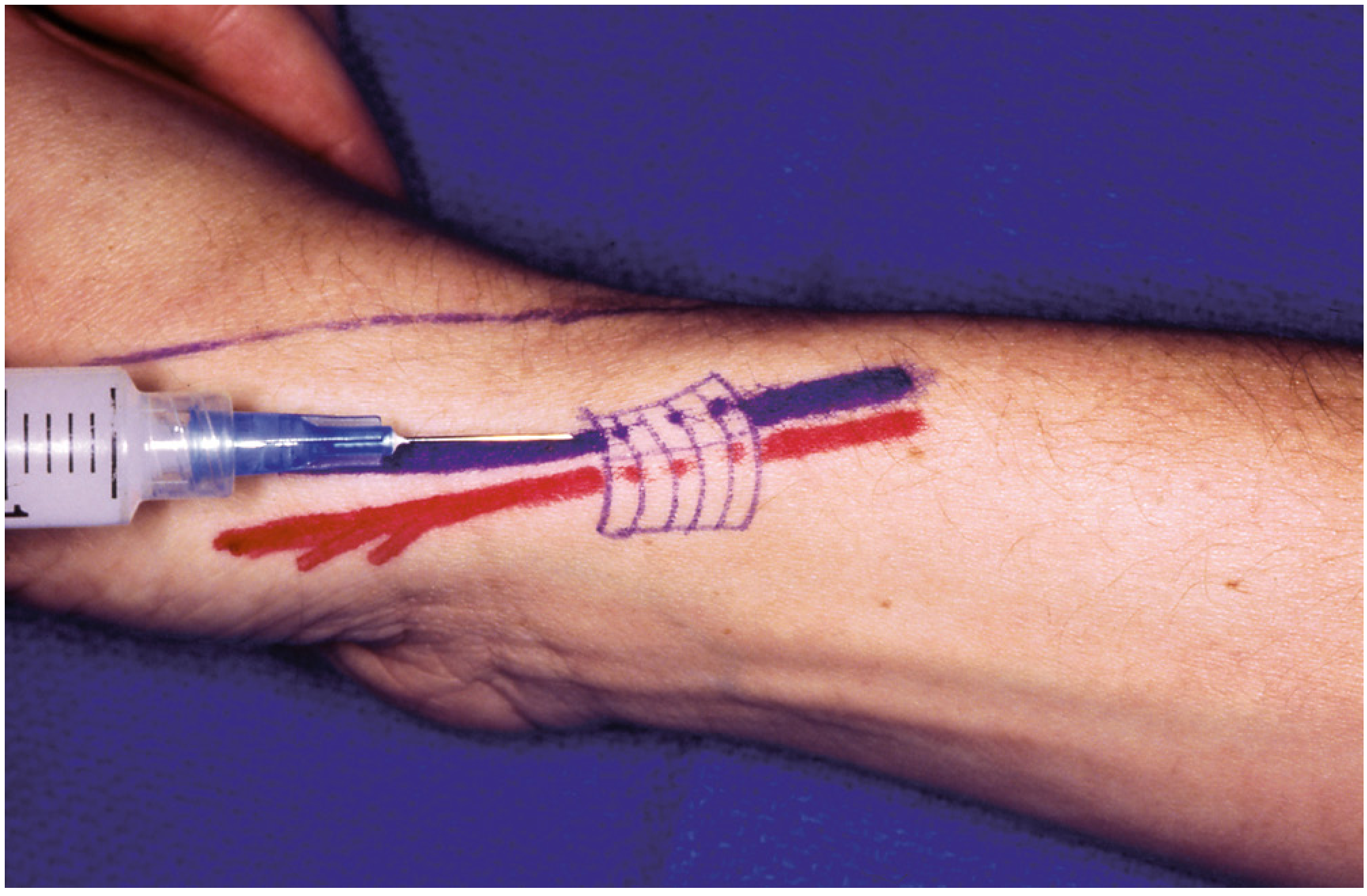
- Injection of corticosteroid into the first dorsal extensor compartment is the mainstay of non-operative treatment
- Success rate >80% with corticosteroid injection (Miller's Review of Orthopaedics)
- Preferred agent: methylprednisolone 5-10 mg (Firestein & Kelley's recommends avoiding triamcinolone due to greater risk of skin complications)
- Technique: insert needle just distal to the radial styloid near the base of the thumb, advance proximally along the tendon sheath
- Ultrasound guidance significantly improves accuracy - studies show >70% complete resolution after a single US-guided injection
- Risks: skin hypopigmentation, subcutaneous fat atrophy, tendon rupture (with repeated intratendinous injections), temporary blood sugar elevation in diabetics
- Combining corticosteroid injection with thumb spica casting for 3-4 weeks has moderate evidence for superior outcomes vs. injection alone
Contraindications to injection: infection, uncontrolled diabetes (relative), brittle bone disease, prior unfavorable response.
Emerging / Adjunct Therapies:
- Extracorporeal Shockwave Therapy (ECSWT): Ranked highest in a 2023-2024 network meta-analysis; leads in short and medium-term pain outcomes
- PRP (Platelet-Rich Plasma) injection: Used when corticosteroid fails; emerging evidence
- Ultrasound-guided tendon release / percutaneous needle tenotomy
- Acupuncture: Evidence is limited
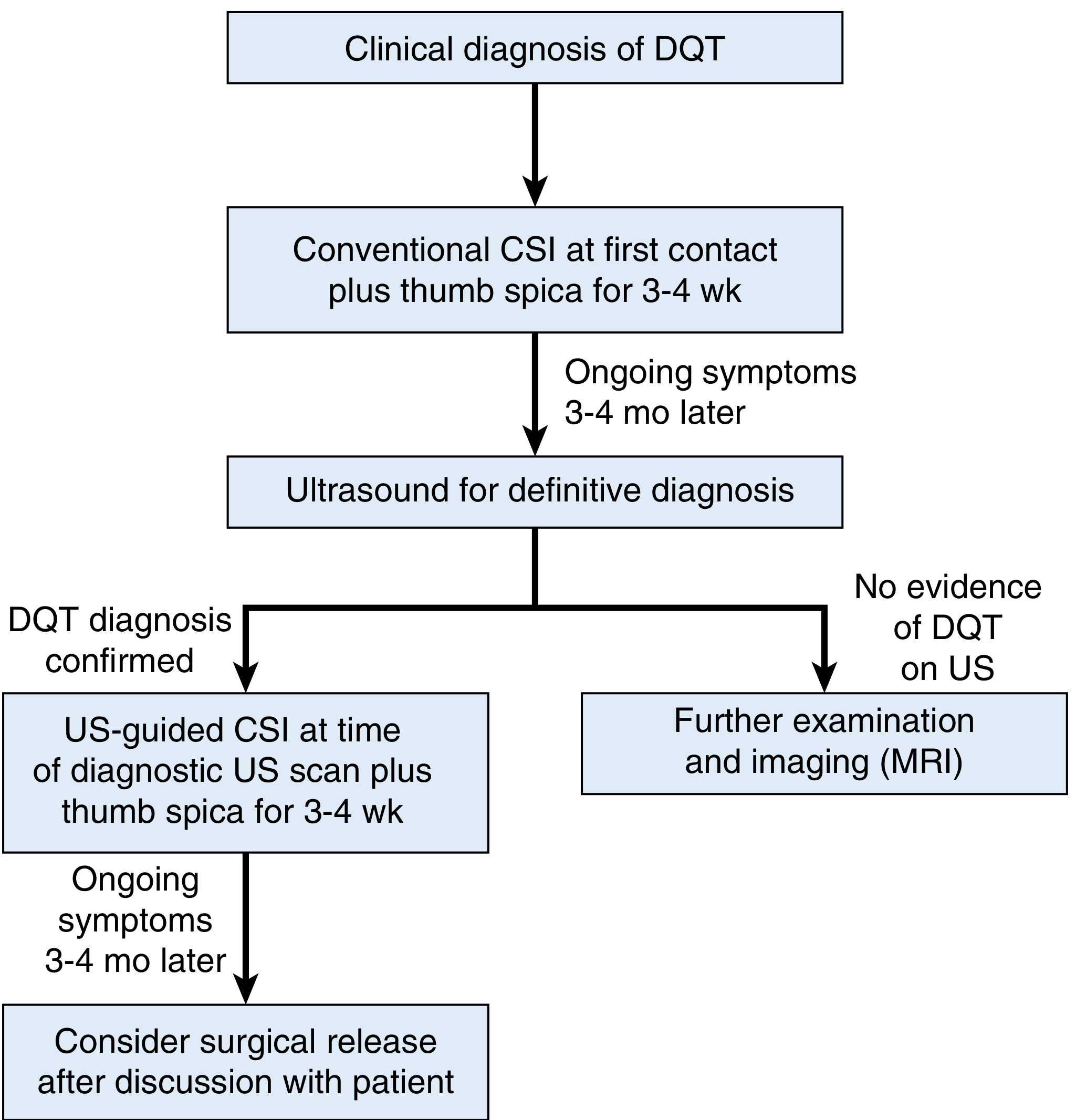
Treatment algorithm (per Campbell's/Challoumas 2023 JAMA Netw Open):
7. Surgical Management
Indication: Failure of adequate non-operative treatment (typically 2 corticosteroid injections and several months of conservative management).
Preoperative Considerations
- Counsel patient on anatomic variations (multiple APL slips, separate EPB subcompartment) and their implications
- Identify the SBRN at risk
- The presence of a subcompartmental septum (detected on US) is the most important predictor of non-operative failure and must be addressed at surgery
TECHNIQUE 81.1 - Release of the First Dorsal Compartment (Campbell's Operative Orthopaedics 15th Ed, 2026)
Setup:
- Local anesthetic with epinephrine (avoids need for tourniquet); or local anesthetic + Esmarch bandage tourniquet on the proximal forearm
- Infiltrate the skin well proximal to the area before preparation
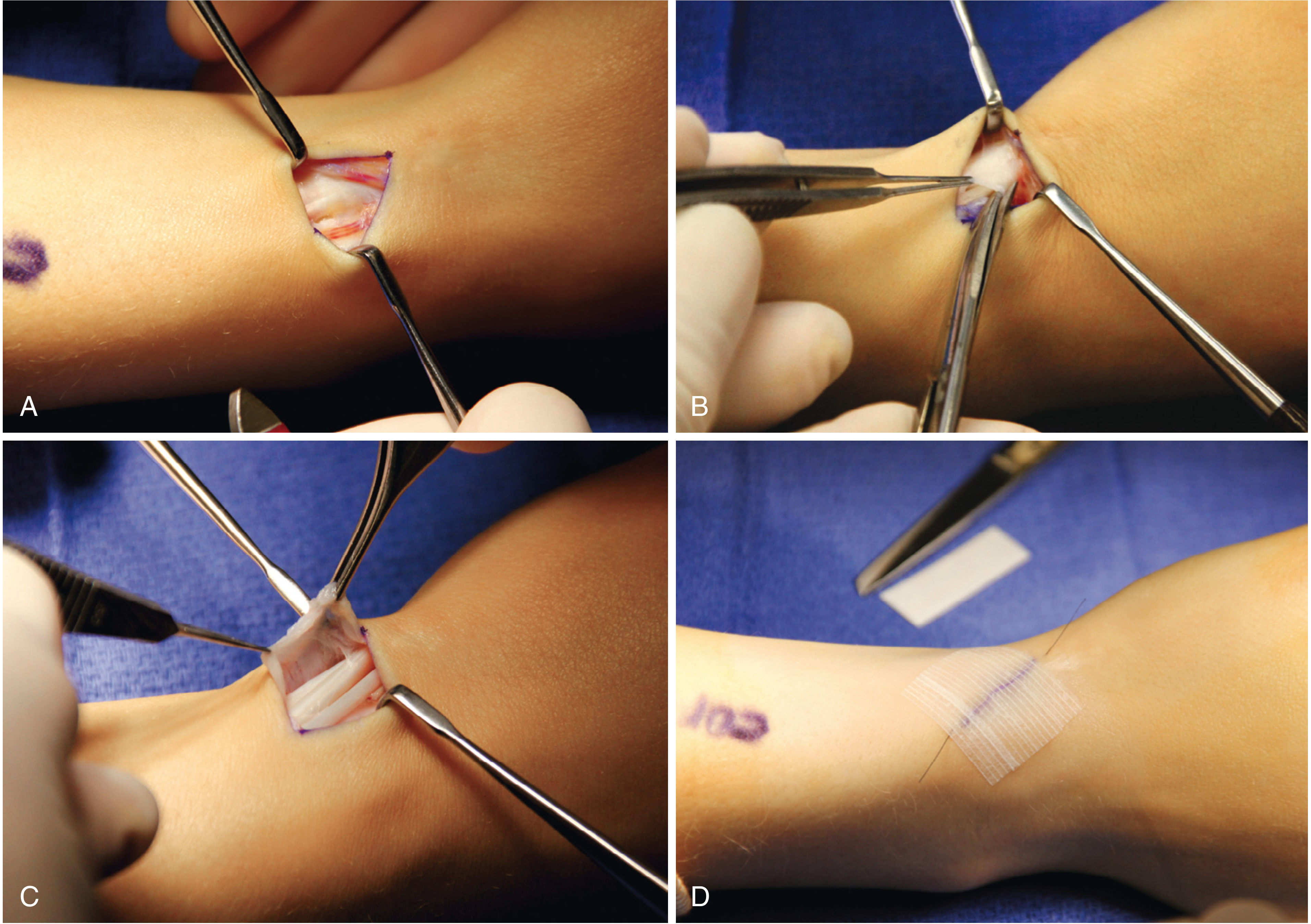
Step-by-step:
Step 1 - Skin Incision:
- Preferred: oblique incision along the EPB tendon axis over the first dorsal compartment
- Alternatives: transverse or longitudinal - all are acceptable
- Caution: Longitudinal incisions create a longer scar area where the cutaneous nerves are more subject to scar adherence
- Incise through skin only at this step
Step 2 - Subcutaneous Dissection (critical nerve-preservation step):
- Carry sharp dissection just through the dermis only - do NOT enter subcutaneous fat with the knife
- Sensory nerves to protect:
- Lateral antebrachial cutaneous nerve - lies above the cephalic vein (more superficial)
- Superficial branch of the radial nerve (SBRN) - lies more deeply in the subcutaneous fat
- After retracting skin edges, use blunt dissection in the subcutaneous fat to expose the retinaculum
Step 3 - Retinacular Exposure:
- Clearly expose the extensor retinaculum (dorsal carpal ligament) over the first dorsal compartment tendons
- Identify the first dorsal compartment tendons proximal to the stenosing area
Step 4 - Compartment Release:
- Open the first dorsal compartment on its dorsoulnar side (Fig. 81.6B and C) - opening on the ulnar side preserves a volar retinacular flap to prevent tendon subluxation
- The EPB tendon is the most dorsal and can be identified by its distally oriented muscle fibers; the APL has no muscular fibers in the distal portion
Step 5 - Inspect for Aberrant Tendons and Subcompartments:
- With thumb abducted and wrist flexed, lift the APL and EPB tendons from their groove
- If tendons cannot be easily retracted from the radial styloid, look for additional aberrant tendons and separate subcompartments
- Release the EPB first, then the APL - this sequence best reveals the presence or absence of a septum
- If no EPB is found, inspect the floor of the compartment for the footprint of the brachioradialis tendon (Y-shaped tendinous insertion); if clearly seen, complete release is confirmed
- If a septum is found and is pronounced, resect the septum
NOTE: Take care not to injure the radial artery, which courses dorsally just beyond the radial styloid.
Step 6 - Prevent Volar Subluxation:
- Make sure the volarly based retinacular flap remains over the released tendons to prevent volar tendon subluxation postoperatively (a common complication if the entire retinaculum is removed)
Step 7 - Closure:
- Close skin only (retinaculum is not repaired)
- Apply a small pressure dressing
Postoperative Care
- Early range of motion is generally encouraged
- Light activities resume within days; full return to work/sport typically within weeks
- Outcomes are generally excellent
Surgical Complications
| Complication | Notes |
|---|---|
| Iatrogenic SBRN injury | Most common and feared; causes numbness/dysesthesia on dorsoradial aspect of hand; prevented by careful blunt dissection |
| Volar tendon subluxation | APL/EPB subluxate volarly if entire retinaculum released without preserving a volar flap |
| Incomplete release | Most common cause of surgical failure; due to missed separate EPB subcompartment or additional APL slips |
| CRPS (Complex Regional Pain Syndrome) | Rare |
| Wound infection/scar hypersensitivity | Especially with longitudinal incisions |
| Tendon rupture | Very rare; from excessive manipulation |
| Recurrence | Uncommon after complete release |
8. Epidemiology Summary
| Parameter | Value |
|---|---|
| Prevalence | ~1.3% women, ~0.5% men |
| Sex ratio | Women : Men = 6-10 : 1 |
| Peak age | 30-50 years |
| Classic population | Postpartum mothers |
| Conservative treatment success | >80% with corticosteroid injection |
| Surgical success rate | Excellent; complications are uncommon when all subcompartments identified |
9. Key Points to Remember
- Pathology is degenerative (myxoid/fibrous), NOT primarily inflammatory - this is why the term tendinopathy is increasingly preferred
- Finkelstein test is the most pathognomonic sign, but not diagnostic alone
- Ultrasound is the most useful adjunct imaging - detects septum, guides injection
- Corticosteroid injection success >80% - first-line non-operative management
- The subcompartmental septum (present in ~20-34%) is the #1 predictor of non-operative failure and the most common cause of surgical failure if missed
- Surgical release is on the dorsoulnar side of the compartment to preserve a volar retinacular flap (prevents tendon subluxation)
- SBRN injury is the most feared surgical complication
- Anatomic variations are common (>50% have aberrant APL slips); always inspect for additional slips and subcompartments at surgery
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 81 (De Quervain Disease, Technique 81.1)
- Miller's Review of Orthopaedics 9th Edition (Section 5, p. 672)
- Rosen's Emergency Medicine - Concepts and Clinical Practice (De Quervain Disease section)
- Firestein & Kelley's Textbook of Rheumatology (injection technique)
- Challoumas et al., JAMA Netw Open 2023 - Management systematic review and network meta-analysis (treatment algorithm)
This is a shared conversation. Sign in to Orris to start your own chat.