suggest new materials or recent advances in materials used in conservative dentistry and endodontics for my poster presentation for my conference
new materials conservative dentistry endodontics
recent advances new materials conservative dentistry endodontics 2024 2025
PMID: 38021683
bioceramics MTA biodentine pulp capping endodontics
bulk fill composite resin dental restoration
https://pmc.ncbi.nlm.nih.gov/articles/PMC12101867
regenerative endodontics stem cells scaffolds revascularization
nanotechnology nanoparticles dental restorative materials
glass ionomer cement resin modified bioactive dental
Recent Advances in Materials - Conservative Dentistry & Endodontics
Poster Presentation Guide (2023-2026)
1. SMART MATERIALS - The New Era
- Smart composites - release ions or antibacterial agents in response to caries-producing acidic pH
- Amorphous calcium phosphate (ACP)-releasing pit and fissure sealants - remineralize enamel on demand; recharge with fluoride over time
- Resin-modified glass ionomers (RMGICs) - exhibit sustained fluoride release and recharge, bioactive, considered "smart" in fluoride responsiveness
- Smart ceramics - zirconia-reinforced materials with improved fracture toughness and optical mimicry of natural tooth
2. CALCIUM SILICATE-BASED BIOCERAMICS
- MTA (Mineral Trioxide Aggregate) - gold standard for pulp capping, perforation repair, apexification
- Biodentine (tricalcium silicate) - faster setting (12 min), superior handling, used as dentine substitute
- Bioceramic sealers (e.g., TotalFill BC Sealer, BioRoot RCS, Well-Root ST) - hydrophilic, dimensionally stable, antibacterial, excellent biocompatibility
- Pre-mixed bioceramic putties - injectable, no mixing, used for root-end filling and perforation repair
- Biocompatibility + bioactivity (stimulate cementum/dentin bridge)
- Antibacterial via high pH (12-13)
- Hydrophilic - sets in moist environment
- Ion release supports remineralization
3. NANOTECHNOLOGY IN RESTORATIVE DENTISTRY & ENDODONTICS
- Nanocomposites - filler particles <100 nm; superior polish, wear resistance, strength vs. hybrid composites
- Nano-hydroxyapatite (n-HA) - remineralizes dentin, used in bonding agents and sealers; promotes pulp protection
- Nano-glass ionomers - improved mechanical and esthetic properties
- Nanosilver fluoride - antimicrobial; arrests caries, explored as cavity liner (Thimmaiah et al., PMID 39372529)
- Zinc oxide nanoparticles (ZnO-NPs) - added to sealers/irrigation solutions for enhanced antibacterial effect
4. BIOACTIVE RESTORATIVE MATERIALS
- Activa BioACTIVE - releases calcium, phosphate, and fluoride; resin-ionomer hybrid; shock-absorbing resin component
- EQUIA Forte - encapsulated glass ionomer with enhanced wear resistance and ion release
- Cention N (alkaline filler) - releases calcium, fluoride, and hydroxyl ions; self-adhesive; alkaline pH reduces secondary caries risk
5. BULK-FILL COMPOSITES
- Flowable bulk-fill (e.g., SDR Plus, SureFil SDR flow+) - used as base, covered with conventional composite
- Sculptable/packable bulk-fill (e.g., Tetric PowerFill, Filtek One Bulk Fill, Omnichroma Flow Bulk) - single increment to full cavity depth
- Universal bulk-fill (e.g., Venus Bulk Fill, G-aenial Universal Injectable)
- Omnichroma - structural color technology; single shade matches any tooth by light scattering; reduces shade selection error
- Ionic-releasing bulk fills - combine fluoride or calcium release with bulk placement
- pH-triggered smart resin systems that release remineralizing ions at low pH (Pintor et al., PMID 39709999)
6. REGENERATIVE ENDODONTICS
- Revascularization/REP (Regenerative Endodontic Procedures) - blood clot scaffold, platelet-rich plasma (PRP), platelet-rich fibrin (PRF) scaffold; stimulates root development in immature necrotic teeth
- Cell homing strategies - scaffolds + growth factors recruit endogenous stem cells without need for transplantation (Kim & Kim, Cells, PMID 39936992; Beco et al., Medicina, PMID 41752774)
- Exosome-based therapy - dental stem cell-derived exosomes as cell-free regenerative agents (Ahmad et al., Int Endod J, PMID 40497413) - the newest frontier
- 3D bioprinting scaffolds - custom scaffold geometries with growth factor loading
- Calcium silicate putties (MTA, Biodentine) as coronal barriers
- Hydroxyapatite scaffolds
- Platelet concentrates (PRF, PRP)
7. ADHESIVE & BONDING SYSTEM ADVANCES
- Universal adhesives (e.g., Scotchbond Universal Plus, Clearfil Universal Bond Quick 2) - used in self-etch, etch-and-rinse, or selective-etch mode; simplified technique, excellent bond strength
- Ceramic primer advances - improved silane technology for zirconia bonding
- MDP monomer (10-methacryloyloxydecyl dihydrogen phosphate) - key ingredient for bonding to zirconia, dentin, and metal; present in leading universal adhesives
- Nano-filled adhesives - improved penetration of dentinal tubules
8. ENDODONTIC SEALER INNOVATIONS
| Sealer Type | Examples | Advantage |
|---|---|---|
| Bioceramic (calcium silicate) | TotalFill BC, BioRoot RCS | Bioactive, antibacterial, dimensional stability |
| Resin-based (epoxy) | AH Plus Bioceramic | Combines resin strength + bioceramic activity |
| Silicone-based | GuttaFlow Bioseal | Flexible, accommodates thermal changes |
| MTA-based | MTA Fillapex | Biocompatible, antibacterial via high pH |
9. PROPOLIS-MODIFIED MATERIALS
10. DIGITAL & AI-ASSISTED MATERIALS SELECTION
- AI-aided shade matching for composite selection
- CBCT-guided access preparation reducing unnecessary dentin removal
- CAD/CAM ceramics with improved fit and strength (e.g., lithium disilicate, zirconia-reinforced lithium silicate)
Suggested Poster Structure
- Title - "Smart, Bioactive, and Nano: The New Generation of Materials in Conservative Dentistry and Endodontics"
- Introduction - Brief overview; the shift from inert to bioactive/intelligent materials
- Smart Materials - Table: stimulus - material - response
- Calcium Silicate Bioceramics - Mechanism + clinical indications; comparison table (MTA vs Biodentine vs BC sealers)
- Nanomaterials - Types and properties; nanocomposites vs. nano-HA
- Bulk-Fill Composites - Advantages, types, latest products
- Regenerative Endodontics - Flowchart of approaches (blood clot → PRF → cell homing → exosomes)
- Conclusion - Future direction: exosomes, 3D bioprinting, AI integration
- Key References - 6-8 most impactful (listed below)
Top References for Your Poster
- Loya PR et al. (2023). "Be Smart and Active in Conservative Dentistry and Endodontics." Cureus. PMID 38021683
- Silva EJNL et al. (2025). "Meta-analysis of calcium silicate-based cements and calcium hydroxide as promoters of hard tissue bridge formation." Int Endod J. PMID 39988950
- Marciano MA et al. (2026). "Applications of Nanomaterials in Restorative Dentistry and Endodontics." Materials (Basel). PMID 42451865
- Ahmad P et al. (2025). "Dental stem cell-derived exosomes in regenerative endodontics." Int Endod J. PMID 40497413
- Fernandes JB et al. (2023). "Bioactive vs. non-bioactive materials in permanent teeth." Clin Oral Investig. PMID 38153565
- Zailai A et al. (2026). "Bioactive and Smart Materials in Preventing Secondary Caries." Cureus. PMID 41585617
- Aga N et al. (2025). "Efficacy of Stem Cells in Endodontic Regeneration." J Evid Based Dent Pract. PMID 40335194
- Wang X et al. (2023). "Clinical application of calcium silicate-based bioceramics in endodontics." J Transl Med. PMID 38007432
give materials used in root canal treatment
root canal treatment materials irrigants obturation sealers
sodium hypochlorite EDTA chlorhexidine root canal irrigation
gutta percha root canal obturation sealer endodontics
materials used in root canal treatment complete list irrigants medicaments obturation sealers
https://www.ncbi.nlm.nih.gov/books/NBK587367
Materials Used in Root Canal Treatment (RCT)
PHASE 1: PRE-OPERATIVE / ISOLATION MATERIALS
| Material | Purpose |
|---|---|
| Rubber dam (latex / nitrile) | Mandatory isolation; prevents contamination, protects airway from instruments and irrigants |
| Rubber dam clamps (stainless steel) | Anchor dam to tooth |
| Local anesthetic (lidocaine 2%, articaine 4%) | Pulpal anesthesia |
| Temporary restorative material (IRM, Cavit, GIC) | Seal between appointments |
PHASE 2: ACCESS CAVITY PREPARATION
| Material/Instrument | Notes |
|---|---|
| Carbide burs (round, tapered fissure) | Initial access through enamel/dentin |
| Endo-Z bur / safe-ended burs | Lateral wall refinement without floor perforation |
| Sodium hypochlorite or saline | Irrigant during access and initial exploration |
| EDTA gel (RC-Prep, File-Eze) | Lubricant for canal scouting; EDTA chelates calcium to soften dentin |
PHASE 3: BIOMECHANICAL PREPARATION (BMP) - INSTRUMENTS
- Stainless steel hand files (K-files, H-files, reamers) - ISO sizes 6-140
- NiTi rotary files (ProTaper Gold, WaveOne Gold, Reciproc Blue, HyFlex EDM) - heat-treated alloys with superior flexibility
- Gates-Glidden drills - coronal flaring
- Apex locators - electronic working length determination
- Barbed broaches - pulp extirpation
PHASE 4: IRRIGANTS (Chemical Debridement)
A. Primary Irrigant
- Concentration: 0.5% - 5.25% (most widely used: 2.5-5.25%)
- Gold standard irrigant
- Actions: dissolves organic tissue (unique among irrigants), broad-spectrum antibacterial, biofilm disruption
- Limitation: does not remove inorganic smear layer, cytotoxic if extruded beyond apex
- A 2024 systematic review (Fiorillo et al., J Craniofac Surg, PMID 39418527) documents NaOCl accidents and clinical management
B. Chelating Agents (Smear Layer Removal)
- Used as 17% solution or gel
- Removes inorganic smear layer, opens dentinal tubules
- Used sequentially with NaOCl: NaOCl first → EDTA → NaOCl again (never mix directly - precipitate forms)
- Standard final irrigation protocol per expert consensus (Int J Oral Sci, PMC10907616): NaOCl (2.5-5.25%) × 1 min → EDTA (17%) × 1 min → NaOCl × 30 sec
- Biopure MTAD; combines smear layer removal + antibacterial effect
- Contains doxycycline, citric acid, Tween 80
- Emerging chelator; comparable to EDTA, less cytotoxic; a 2025 scoping review (Kapur et al., BMC Oral Health, PMID 41361750) supports its potential
C. Secondary / Final Irrigants
| Agent | Concentration | Use |
|---|---|---|
| Chlorhexidine (CHX) | 2% | Final irrigant in severely infected canals; excellent substantivity (persists 12 weeks); anti-E. faecalis; never mix with NaOCl (forms para-chloroaniline precipitate) |
| QMix | - | Mixture of EDTA + CHX; removes smear layer + antibacterial in one step |
| Saline (0.9% NaCl) | - | Flushing between irrigants; no antibacterial effect alone |
| Distilled water | - | Separating CHX from NaOCl |
| 95% Ethanol | - | Final rinse to dry canal; reduces surface tension, aids sealer penetration |
| Hydrogen peroxide (H₂O₂) | 3% | Historically used; no longer recommended routinely (weak activity vs. E. faecalis) |
D. Irrigation Activation Techniques
- Passive Ultrasonic Irrigation (PUI) - most evidence-supported activation method
- Sonic activation (EndoActivator, EDDY)
- Laser-assisted irrigation (Erbium:YAG, diode)
- Negative pressure irrigation (EndoVac) - draws irrigant apically, reduces extrusion risk
- XP-endo Finisher file - thermomechanical agitation
PHASE 5: INTRACANAL MEDICAMENTS (Between Appointments)
A. Calcium Hydroxide Ca(OH)₂ - THE STANDARD
- Most widely used intracanal medicament
- Mechanism: high pH (12.5-12.8) kills bacteria, denatures proteins, promotes periapical healing
- Brands: Ultracal XS, Metapaste, Calcipex
- Placement: 1-2 weeks between visits; removed by irrigation (NaviTip FX, XP-Finisher) before obturation
- A 2026 systematic review (de Oliveira et al., Odontology, PMID 40517172) confirms Ca(OH)₂ promotes dentin growth factor release
B. Antibiotic Pastes
- Metronidazole + Ciprofloxacin + Minocycline
- Used in regenerative endodontics for immature necrotic teeth
- Modified TAP (mTAP): minocycline replaced by amoxicillin or cefaclor (to avoid crown staining)
- Metronidazole + Ciprofloxacin (no minocycline)
- Preferred in regenerative endodontics to prevent tooth discoloration
C. Older/Less-Used Medicaments (Historical)
| Medicament | Reason Declined |
|---|---|
| Formocresol (formaldehyde + cresol) | Cytotoxic, carcinogenic concerns; replaced by Ca(OH)₂ |
| Camphorated Monochlorophenol (CMCP) | Cytotoxic; no longer recommended |
| Ledermix paste (triamcinolone + demeclocycline) | Reduces post-op pain but antibiotic resistance concerns |
| Iodoform pastes (Metapex, Vitapex = Ca(OH)₂ + iodoform) | Used in primary teeth; slowly resorbable |
PHASE 6: OBTURATION MATERIALS
A. Core Material - GUTTA-PERCHA (GP)
- Composition: ~20% gutta-percha (trans-polyisoprene), ~60-75% zinc oxide, barium sulfate (radiopaque), wax/resins
- Forms: standardized ISO-sized cones, accessory cones (fine-fine, fine, medium-fine)
- Thermoplastic at 60-65°C - used in warm vertical compaction techniques
- Properties: biocompatible, dimensionally stable, radiopaque, retrievable, insoluble in tissue fluids
| Type | Description |
|---|---|
| Conventional/standardized GP cones | ISO-matched to master file size; cold lateral compaction |
| Thermoplasticized GP (Obtura III, Calamus) | Injected at ~160°C into canal; used in warm vertical compaction |
| Carrier-based GP (Thermafil, GuttaCore) | GP coated on plastic/GP carrier; single-step warm obturation |
| GP + bioceramic-coated cones (GuttaCore Bioceramic, TotalFill GP) | Coated with bioceramic for enhanced apical seal |
B. Root Canal Sealers
1. Zinc Oxide Eugenol (ZOE) Sealers
- Examples: Grossman's sealer, Tubliseal, Roth's sealer
- Oldest class; proven long-term record
- Eugenol is anti-inflammatory and antibacterial
- Disadvantages: soluble, shrinks on setting, cytotoxic initially, stains dentin
- Pulp Canal Sealer (Kerr): zinc oxide + eugenol + silver particles
2. Calcium Hydroxide-Based Sealers
- Examples: Sealapex, Apexit Plus
- Releases Ca(OH)₂ slowly; biocompatible, promotes hard tissue
- Poor dimensional stability, soluble long-term
3. Resin-Based Sealers
- AH Plus (Dentsply Sirona) - epoxy resin + diamine; current benchmark resin sealer
- Excellent adhesion to dentin, low solubility, long setting time (good for complex canals)
- AH Plus Bioceramic Sealer (newer version): resin + bioceramic particles combined
- RealSeal (Resilon): resilon core + resilon sealer; aimed for "monoblock" - not proven superior to GP
- MetaSEAL: dual-cure resin sealer; excellent bond strength
4. Glass Ionomer-Based Sealers
- Examples: Ketac-Endo (3M)
- Chemically bonds to dentin; fluoride release
- Limited use due to brittleness and difficult removal
5. Bioceramic Sealers (Most Rapidly Growing Category)
- Examples: TotalFill BC Sealer (FKG), BioRoot RCS (Septodont), Well-Root ST, EndoSequence BC Sealer, iRoot SP
- Composition: calcium silicate (MTA-related chemistry), calcium phosphate
- Mechanism: hydrophilic - uses moisture in dentinal tubules to set; expands slightly on setting (better seal)
- pH: 12.8 (antibacterial), releases calcium and hydroxyl ions
- Biocompatible - promotes cementum and bone deposition at the apex
- Premixed, syringe delivery - no mixing required
- Used with single-cone technique (hydraulic obturation)
- A 2024 meta-analysis (Zamparini et al., Int Endod J, PMID 38606520) finds premixed bioceramic sealers comparable to standard sealers in treatment outcomes with less post-obturation pain
- A 2026 meta-analysis (Mushtaq et al., Sci Rep, PMID 41872366) confirms no significant difference in success rate between filling techniques/materials but bioceramic sealers show better biocompatibility
6. Silicone-Based Sealers
- GuttaFlow Bioseal (Coltene): combines GP powder in polydimethylsiloxane sealer; flowable at room temp; dimensional stability; biocompatible
C. Obturation Techniques and Associated Materials
| Technique | Materials Used |
|---|---|
| Cold Lateral Compaction | Standardized GP master cone + accessory cones + sealer + finger spreaders |
| Warm Vertical Compaction (Schilder) | GP + sealer + heated pluggers (Touch'n Heat, System B) |
| Continuous Wave (Elements, Calamus) | Thermoplasticized GP + sealer + pluggers |
| Carrier-based (Thermafil) | Carrier + GP + sealer |
| Single Cone / Hydraulic | Single-matched GP cone + bioceramic sealer (preferred with BC sealers) |
| Injectable Thermoplasticized GP (Obtura III) | Hot GP + sealer |
PHASE 7: PERFORATION REPAIR / SPECIAL INDICATIONS
| Material | Indication |
|---|---|
| MTA (ProRoot MTA, Angelus MTA) | Perforation repair, open apices (apexification), root-end filling, pulp capping |
| Biodentine (tricalcium silicate) | Faster-setting MTA alternative; perforation repair, deep caries lining, pulpotomy |
| Calcium Enriched Mixture (CEM) | Iranian bioceramic; pulp capping and apexification |
| Bioceramic putties (TotalFill BC RRM Putty) | Root-end filling, perforation repair; premixed, no mixing needed |
PHASE 8: CORONAL SEAL / RESTORATION
| Material | Use |
|---|---|
| IRM (Intermediate Restorative Material) | Temporary seal between visits (zinc oxide + polymer) |
| Cavit | Temporary seal; self-sealing with moisture |
| Glass Ionomer Cement (GIC) | Base/liner over canal orifices before permanent restoration |
| Composite resin | Permanent coronal restoration in anterior teeth |
| Amalgam | Posterior teeth (declining use) |
| Post and core (fiber post + composite, cast metal post) | When insufficient tooth structure remains |
| Full coverage crown | Recommended for posterior endodontically treated teeth |
QUICK SUMMARY TABLE
| Stage | Key Materials |
|---|---|
| Irrigation | NaOCl (0.5-5.25%), EDTA 17%, CHX 2%, QMix, MTAD |
| Smear layer removal | EDTA, MTAD, Maleic acid 7% |
| Intracanal medicament | Calcium hydroxide, TAP/DAP (in REP) |
| Core filling | Gutta-percha (cold/warm/carrier-based) |
| Sealer | ZOE / Ca(OH)₂ / Resin (AH Plus) / Bioceramic (TotalFill BC) / GIC / Silicone |
| Special repair | MTA, Biodentine, Bioceramic putty |
| Coronal seal | GIC + composite or crown |
Key Evidence Sources
- Expert consensus on irrigation and intracanal medication (2024) - PMC10907616
- Zamparini et al. (2024) - Bioceramic sealers meta-analysis. Int Endod J. PMID 38606520
- Mushtaq et al. (2026) - Filling techniques/materials systematic review. Sci Rep. PMID 41872366
- Pirani & Camilleri (2023) - Root canal filling materials review. Int Endod J. PMID 35735776
- StatPearls - Endodontic materials for obturation
write about SealBio in endodontics in 1000 words pointwise for my poster prseentation
SealBio endodontics obturation biological
SealBio endodontics technique concept biological obturation Carollo
https://pmc.ncbi.nlm.nih.gov/articles/PMC3482744
SealBio non-obturation regenerative endodontic mature teeth Shah
SealBio endodontics procedure steps advantages disadvantages clinical studies 2020 2025
PMID: 31708612
https://www.giornaleitalianoendodonzia.it/gie/article/view/4…
SealBio in Endodontics
A Novel Non-Obturation Regenerative Endodontic Technique
1. INTRODUCTION & BACKGROUND
- Root canal treatment (RCT) has traditionally relied on filling the cleaned canal with gutta-percha and sealer - a practice in use for over 150 years
- The fundamental question this challenges: Is obturation truly necessary if the canal is completely disinfected?
- Sabeti et al. demonstrated no significant difference in periapical healing in teeth with and without obturation when complete disinfection was achieved and a tight coronal seal was maintained
- This observation laid the biological foundation for SealBio
- Classic teaching by Tronstad had already proposed the concept of "Biological Obturation" as a future possibility
- Metzger & Abramowitz argued that endodontics should move beyond mechanistic cleaning/shaping and embrace biologically-driven healing concepts
2. DEFINITION & CONCEPT
- SealBio (Seal = apical seal; Bio = biological) is a novel, non-obturation endodontic treatment protocol based on regenerative and tissue engineering principles
- Developed and described by Dr. Naseem Shah et al. (2012), published in the Journal of Conservative Dentistry (PMC3482744)
- It was originally conceived for mature, non-vital permanent teeth with pulpal/periapical pathology - a population traditionally excluded from regenerative protocols
- The core philosophy: replace the inert obturating material with a living, regenerated biological barrier at the apex formed by the patient's own tissues and stem cells
- The canal is NOT filled with gutta-percha; instead, the apical seal is achieved by biologically induced tissue formation
- The coronal seal is achieved with calcium sulphate-based cement (not traditional restorative)
3. BIOLOGICAL RATIONALE & MECHANISM
- Multiple stem cell populations reside in the periapical region:
- Periodontal ligament stem cells (SCPDL)
- Dental pulp stem cells (DPSC)
- Bone marrow mesenchymal stem cells (BMMSC)
- Stem cells from apical papilla (SCAP)
- In revascularization (regenerative endodontics for immature teeth), bleeding into the canal creates a fibrin clot scaffold → stem cells seed into it → differentiate → deposit mineralized tissue
- SealBio hypothesizes the same mechanism can occur at the apical foramen of mature teeth when bleeding is intentionally induced by over-instrumentation
- The blood clot at the apex acts as a natural scaffold for stem cell seeding, proliferation, and differentiation
- This leads to cementum-like or bone-like tissue deposition at the foramen - creating a biological, living apical seal
- Triple antibiotic paste (metronidazole + ciprofloxacin + tetracycline) is used between appointments to eliminate resistant microorganisms, including Enterococcus faecalis, ensuring a sterile environment for regeneration
4. STEP-BY-STEP PROTOCOL
- Standard access opening and canal negotiation
- Crown-down cleaning and shaping technique
- Copious irrigation with 2.5% sodium hypochlorite throughout
- Triple Antibiotic Paste (TAP): metronidazole + ciprofloxacin + tetracycline placed for 1-2 appointments (depending on severity of infection/periapical status)
- Goal: eliminate all residual bacteria and reduce microbial load to zero before inducing bleeding
- At the obturation appointment, canals enlarged with instruments 2-4 sizes larger than the Master Apical File (MAF) at working length
- Removes loose apical debris from the apical third, deltas, and accessory canals
- Disrupts bacterial niches that escape standard instrumentation
- Larger K-files used to widen the cemental portion of the canal at the apex
- Ensures smooth passage for subsequent over-instrumentation
- Also facilitates thorough cleaning of the cemental canal wall
- Files are deliberately passed beyond the apex into the periapical region
- Purpose: induce bleeding from the periapical tissues into the canal
- The blood fills the apical portion and forms a fibrin clot scaffold
- The blood clot is allowed to stabilize at the level of the cemento-enamel junction or apical third
- This clot serves as the scaffolding matrix for stem cell migration and tissue regeneration
- Calcium sulphate cement (e.g., Cavit - zinc sulphate based) is condensed into the coronal third of root canal using hand pluggers
- Canal orifices are sealed with GIC (glass ionomer cement)
- Immediate permanent coronal restoration placed
- Immediate post-treatment radiograph taken
- Clinical and radiographic review at 6, 12, and 18 months
- CBCT used when available to measure: lesion size, bone and cementum density (in Hounsfield Units), and periapical index (CBCT-PAI)
5. CLINICAL EVIDENCE & OUTCOMES
- Shah et al. (2012): Original case series; SealBio was favorable in resolving periapical infection clinically and radiographically; CBCT showed improved bone density and lesion reduction
- Jha, Virdi & Nain (2019) - Int J Clin Pediatr Dent (PMID 31708612): Randomized comparative trial, 30 patients, 18-month follow-up:
- SealBio vs. conventional gutta-percha obturation
- No statistically significant difference in periapical healing (PAI scores) between the two groups
- SealBio required significantly less chair time than conventional obturation
- Both groups showed equally favorable outcomes at 18 months
- 2024 Systematic Review (Cernera et al., Giornale Italiano di Endodonzia):
- 4 studies included; reported success rates of 97-100% with SealBio technique
- Limitation: all included studies had high risk of bias
- Conclusion: SealBio does not yet provide sufficient evidence to replace the standard protocol; well-conducted RCTs are needed
- US Patent granted for the SealBio technique (US9180072B2), confirming its novelty
6. ADVANTAGES
- Eliminates the need for obturation materials - no gutta-percha, no sealer required
- Less technique sensitive compared to warm vertical compaction and carrier-based obturation
- Reduced chair time - significantly faster at the obturation appointment
- Cost effective - eliminates expensive gutta-percha, sealer, and obturation devices
- Biologically superior - living tissue replaces inert material at the apex
- Ideal for severely curved canals where conventional obturation is technically challenging
- Post space readily available - canal is left empty; fiber post placement is straightforward if needed later
- No risk of material extrusion - avoids post-obturation pain and periapical cytotoxicity from overfilled sealers
- Environmentally friendly - reduces chemical materials used per procedure
- Retreatment simplified - calcium sulphate sealer (Cavit) is easily removable
7. DISADVANTAGES & LIMITATIONS
- Intentional over-instrumentation may cause acute exacerbation post-operatively (Phoenix abscess flare-up)
- Risk of apical debris extrusion into periapical tissues during apical clearing/over-instrumentation (highlighted in the 2024 systematic review)
- Limited clinical evidence: only 4 studies published to date; all with high risk of bias
- Patient selection is critical - not suitable for teeth with incomplete apices, open apices, or those requiring immediate post-endodontic prosthetic use
- Success depends entirely on the host's regenerative capacity - older patients, immunocompromised individuals, or those with systemic disease may have compromised healing
- The type of tissue deposited at the apex (cementum, bone, or connective tissue) cannot be controlled or predicted
- No standardized protocol - variability in over-instrumentation extent, clot management, and coronal seal materials across studies
- Cannot be used where the canal must be filled for immediate prosthetic reasons (e.g., cast post and core)
- Long-term data beyond 18 months are currently lacking
8. INDICATIONS & CONTRAINDICATIONS
| Indications | Contraindications |
|---|---|
| Non-vital mature permanent teeth | Immature open apex teeth (use REP instead) |
| Teeth with apical periodontitis | Teeth requiring immediate post placement |
| Severely curved/calcified canals | Immunocompromised patients |
| Single-visit or two-visit RCT cases | Teeth with vertical root fractures |
| Cases where operator prefers bio-based approach | Retreatment of previously obturated teeth (relative) |
9. COMPARISON WITH CONVENTIONAL RCT
| Feature | Conventional RCT | SealBio |
|---|---|---|
| Apical seal material | Gutta-percha + sealer | Biological tissue (clot → regeneration) |
| Obturation needed | Yes | No |
| Chair time | Longer | Shorter |
| Technique sensitivity | High (warm compaction) | Moderate |
| Cost | Higher | Lower |
| Retreatability | Moderate | Easy |
| Evidence level | Strong (decades of data) | Limited (case series/1 RCT) |
| Biological outcome | Inert seal | Living tissue formation |
10. FUTURE PERSPECTIVES
- SealBio represents the convergence of regenerative dentistry and conventional endodontics
- Future research needs: large-scale RCTs, histological confirmation of tissue type at the apex, and CBCT-based outcome studies
- Could be enhanced by addition of growth factors (BMP-2, TGF-β) or PRF/PRP scaffolds to further stimulate tissue regeneration
- May integrate with bioceramic coronal barriers (MTA, Biodentine) instead of calcium sulphate for a more robust coronal seal
- The technique challenges the dogma of obturation and opens a new era of "Biological Endodontics"
KEY REFERENCES
- Shah N et al. (2012). "SealBio: A novel, non-obturation endodontic treatment." J Conserv Dent. PMC3482744
- Jha P, Virdi MS et al. (2019). "Regenerative Approach for RCT of Mature Permanent Teeth." Int J Clin Pediatr Dent. PMID 31708612
- Cernera M et al. (2024). "Novel non-obturation based concept of regeneration: Apical debris extrusion." Giornale Italiano di Endodonzia. 38(2).
- Sabeti MA et al. - Periapical healing with/without obturation after disinfection (foundational evidence supporting SealBio)
Create a visual flowchart diagram of SealBio steps for poster display
A clean, professional medical/dental poster flowchart titled "SealBio Protocol: Step-by-Step" showing the following sequential steps connected by downward arrows in a vertical flowchart layout: Step 1 - ACCESS & INITIAL DEBRIDEMENT: Icon of tooth with access opening. Text: "Crown-down technique | Irrigation with 2.5% NaOCl" Step 2 - INTRACANAL MEDICAMENT: Icon of syringe/paste. Text: "Triple Antibiotic Paste (TAP) | Metronidazole + Ciprofloxacin + Tetracycline | 1-2 appointments" Step 3 - APICAL CLEARING: Icon of file in canal. Text: "Enlarge 2-4 sizes larger than MAF | Removes apical debris, deltas & accessory canals" Step 4 - APICAL FORAMEN WIDENING: Icon of enlarged apex. Text: "Larger K-files at apex | Cleans cemental canal wall | Prepares for over-instrumentation" Step 5 - INTENTIONAL OVER-INSTRUMENTATION: Icon of file going beyond apex with blood drop. Text: "Files pass BEYOND apex | Induces periapical BLEEDING | Blood clot = biological scaffold" Step 6 - CLOT STABILIZATION: Icon of blood clot at apex. Text: "Fibrin clot forms at apex | Stem cells (SCAP, DPSC, PDL) seed into clot | Mineralized tissue deposition begins" Step 7 - CORONAL SEAL: Icon of canal with top seal. Text: "Calcium sulphate cement (Cavit) | Condensed into coronal 1/3 | GIC over canal orifices | Permanent restoration placed" Step 8 - FOLLOW-UP: Icon of X-ray/radiograph. Text: "Clinical & radiographic review | 6, 12, 18 months | CBCT evaluation of periapical healing" Design: White background with a teal/dark blue color scheme. Each step in a rounded rectangle box with a step number circle on the left. Arrows in teal connecting each box. A legend at the bottom: "MAF = Master Apical File | TAP = Triple Antibiotic Paste | SCAP = Stem Cells from Apical Papilla". Small note at bottom: "No gutta-percha. No sealer. Biologically sealed." Poster-quality, high resolution, clean academic style.
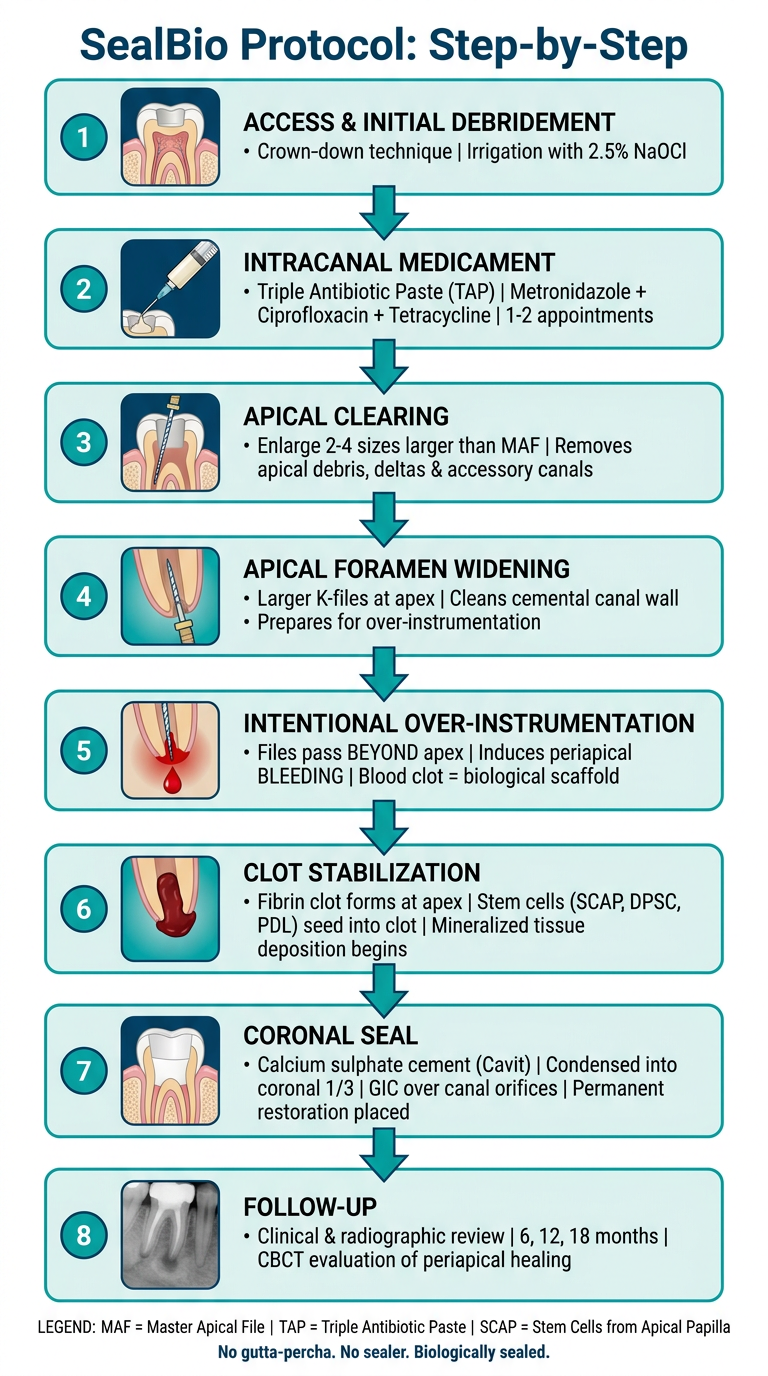
- Access & Initial Debridement - crown-down + NaOCl irrigation
- Triple Antibiotic Paste - TAP placement for 1-2 appointments
- Apical Clearing - enlargement 2-4 sizes beyond MAF
- Apical Foramen Widening - K-files to clean cemental wall
- Intentional Over-Instrumentation - induces periapical bleeding (the key step)
- Clot Stabilization - fibrin scaffold + stem cell seeding
- Coronal Seal - Cavit + GIC + permanent restoration
- Follow-Up - radiographic/CBCT review at 6, 12, 18 months
- You can right-click and save the image at full resolution
- Place this flowchart centrally on your poster as the visual anchor
- Pair it with the comparison table (SealBio vs. Conventional RCT) from the previous write-up for maximum impact
- The tagline at the bottom - "No gutta-percha. No sealer. Biologically sealed." - works well as a poster headline
SWEEPS Laser Technology in 1000 words pointwise
SWEEPS laser endodontics irrigation photoacoustic
SWEEPS laser technology endodontics shock wave enhanced emission photoacoustic streaming Fotona mechanism
PMID: 35267110
PMID: 37599293
PMID: 35443216
SWEEPS Er:YAG laser smear layer removal biofilm disinfection root canal
https://pmc.ncbi.nlm.nih.gov/articles/PMC10557991
PMID: 40136729
PMID: 38484867
PMID: 38004605
SWEEPS vs PIPS vs ultrasonic irrigation comparison clinical outcomes 2023 2024 2025
SWEEPS Laser Technology in Endodontics
Shock Wave Enhanced Emission Photoacoustic Streaming
1. INTRODUCTION & BACKGROUND
- Effective disinfection of the root canal system remains the greatest challenge in endodontics - conventional needle irrigation (CNI) consistently fails to reach lateral canals, isthmuses, apical deltas, and dentinal tubules
- Laser-assisted irrigation has evolved over three generations: direct laser ablation → PIPS (Photon-Induced Photoacoustic Streaming) → SWEEPS (Shock Wave Enhanced Emission Photoacoustic Streaming)
- SWEEPS represents the third-generation, most advanced laser irrigation modality, developed by Fotona (Ljubljana, Slovenia), commercially introduced around 2017
- It is available exclusively on Fotona's LightWalker and SkyPulse laser platforms, powered by the proprietary ASP (Adaptive Structured Pulse) technology
- SWEEPS is not a direct tissue ablation technique - it is purely an irrigant activation system that dramatically amplifies the cleaning power of existing irrigants
- A 2025 systematic review (Fiegler-Rudol et al., Dent J, PMID 40136729) confirms Er:YAG laser-activated irrigation including SWEEPS significantly improves root canal disinfection over conventional and ultrasonic methods
2. FULL FORM & DEFINITION
-
S - Shock Wave
-
W - Enhanced
-
E - Emission
-
E - (Photoacoustic)
-
P - Photoacoustic
-
S - Streaming
-
SWEEPS is defined as: "A laser irrigation activation technique that uses synchronized pairs of ultra-short Er:YAG laser pulses to generate sequenced cavitation bubbles, producing amplified photoacoustic shock waves that drive irrigant streaming throughout the entire root canal system"
3. LASER SYSTEM & EQUIPMENT
- Laser type: Er:YAG (Erbium: Yttrium-Aluminium-Garnet)
- Wavelength: 2940 nm - peak absorption wavelength of water; maximum efficiency in aqueous irrigants
- Platform: Fotona LightWalker AT / LightWalker ATA / SkyPulse laser systems
- Technology engine: ASP (Adaptive Structured Pulse) - Fotona's proprietary 3rd generation pulse generation technology; the ONLY method capable of generating the SWEEPS process
- Delivery tip: Fotona's specially designed radial-firing Er:YAG endodontic fiber tip, placed in the pulp chamber only - does NOT enter the canal
- Pulse duration: Super-short pulses (SSP mode); pulse duration in microseconds
- Energy per pulse: Very low (minimizes thermal effects)
- Repetition rate: Low Hz, synchronized dual-pulse delivery
4. MECHANISM OF ACTION - HOW SWEEPS WORKS
- The first ultra-short Er:YAG laser pulse is fired into the liquid irrigant in the pulp chamber
- The 2940 nm wavelength is instantly absorbed by water in the irrigant
- A primary cavitation bubble rapidly expands to its maximum volume within the fluid
- Before the primary bubble collapses, a second laser pulse is fired at a precisely calculated time - just before the collapse phase of the first bubble
- This optimal timing is only achievable through ASP technology and is what distinguishes SWEEPS from PIPS
- The rapidly expanding second bubble exerts intense pressure on the collapsing primary bubble
- This accelerates the collapse of the primary bubble far beyond what occurs naturally
- The accelerated collapse generates amplified primary shock waves - significantly more powerful than those produced by PIPS
- The primary shock waves propagate through the irrigant into the canal system
- They trigger secondary cavitation bubbles to form and collapse along the entire length and width of the canal
- This creates a cascade of secondary shock waves propagating into lateral canals, anastomoses, isthmus areas, and dentinal tubules - areas completely inaccessible to mechanical instrumentation
- The combination of shock waves and bubble dynamics drives intense turbulent fluid motion (streaming) throughout the 3D root canal system
- This carries the irrigant into all anatomical spaces, maximizing disinfection, debris removal, smear layer elimination, and biofilm disruption
- The tip stays in the pulp chamber - no direct contact with canal walls needed; this is of particular importance in thin-walled canals
5. COMPARISON: SWEEPS vs. PIPS vs. ULTRASONIC IRRIGATION (PUI)
| Feature | Conventional Needle | PUI (Ultrasonic) | PIPS | SWEEPS |
|---|---|---|---|---|
| Mechanism | Fluid flow only | Acoustic streaming | Single pulse photoacoustic | Dual-pulse amplified photoacoustic |
| Pulse type | None | Ultrasonic vibration | Single Er:YAG pulse | Synchronized dual Er:YAG pulses |
| Bubble dynamics | None | Cavitation | Single bubble cycle | Accelerated collapse + cascade |
| Shock wave intensity | None | Moderate | Moderate | High (amplified) |
| Canal tip placement | 2-3mm from apex | In canal | In pulp chamber | In pulp chamber |
| Lateral canal penetration | Poor | Moderate | Good | Superior |
| Isthmus debridement | Poor | Moderate | Good | Superior |
| Thermal risk | None | Low | Low | Very low (minimal energy/pulse) |
| Post-op pain | Highest | Moderate | Low | Lowest |
- An RCT by Erkan et al. (2022) (PMID 35267110) - 200 patients, 5 groups: SWEEPS and PIPS had the lowest postoperative pain at all time points (8h, 24h, 48h, 7 days) compared to PUI, sonic (EDDY), and manual dynamic activation (MDA); the MDA group had the highest pain scores
- Mittal et al. (2023) - RCT confirmed pain reduction in descending order: SWEEPS > PIPS > PUI > conventional needle irrigation
6. CLINICAL EVIDENCE
A. Debridement of Isthmus Areas
- Bago et al. (2023) (PMID 37599293) - 41 lower molars with root canal isthmuses: SWEEPS removed significantly more residual pulp tissue from the isthmus than both UAI (p=0.003) and conventional needle irrigation (p=0.014); UAI and NI showed similar but lower efficiency - confirming SWEEPS superiority in the most anatomically challenging areas
B. Reduction of NaOCl Concentration Required
- Lei et al. (2022) (PMID 35443216) - 48 bovine root canals infected with E. faecalis: SWEEPS-activated low-concentration NaOCl (0.5%, 1.0%) achieved antibacterial reduction equivalent to high-concentration NaOCl without activation; low-concentration SWEEPS = high-concentration conventional irrigation - clinically significant for reducing NaOCl toxicity risks
C. Antibacterial Efficacy vs. E. faecalis Biofilm
- Ensafi et al. (2022) (PMID 36162755) - SWEEPS vs. antimicrobial photodynamic therapy (aPDT) with curcumin: both showed significant reduction of E. faecalis biofilm; combination with aPDT potentiates the antimicrobial effect
- Shahi Ardakani et al. (2023) (PMID 38004605) - SWEEPS + aPDT (riboflavin + blue diode laser) combination was highly effective in reducing E. faecalis CFU count, supporting SWEEPS as a synergistic adjunct to other antimicrobial techniques
D. Sealer Penetration into Dentinal Tubules
- Koruk et al. (2022) (PMID 35917520) - laser-activated irrigation techniques including SWEEPS significantly improved sealer penetration depth into dentinal tubules compared to conventional needle irrigation, improving obturation quality
E. Post-Operative Pain - Systematic Review
- McGillivray & Dutta (2024) (PMID 38484867) - systematic review of 6 RCTs confirms laser-activated irrigation reduces post-endodontic pain (PEP) in the first 48 hours post-treatment; laser systems (PIPS/SWEEPS) outperformed other activation methods
F. Er:YAG Systematic Review (2025)
- Fiegler-Rudol et al. (2025) (PMID 40136729) - PRISMA systematic review of 15 studies (2015-2025): ALL studies found Er:YAG laser activation (PIPS and SWEEPS) significantly improved disinfection over conventional or ultrasonic methods; SWEEPS yielded superior bacterial reduction especially apically and enabled lower NaOCl concentrations
7. ADVANTAGES OF SWEEPS
- Superior 3D disinfection - reaches lateral canals, accessory canals, isthmuses, and dentinal tubules that instruments and conventional irrigation cannot reach
- Tip stays in pulp chamber - no risk of ledging, transportation, or perforation; no special canal enlargement needed
- Non-thermal - minimal thermal energy per pulse; safe for surrounding periodontal tissues
- Allows lower NaOCl concentrations - same antimicrobial effect with 0.5-1% NaOCl as conventional 5.25%; reduces risk of NaOCl accidents, apical extrusion damage, and patient discomfort
- Superior smear layer removal - opens dentinal tubules for better sealer penetration and obturation quality
- Lowest post-operative pain of all irrigation activation methods - proven in multiple RCTs
- Non-contact technique - no direct canal contact; ideal for calcified, narrow, curved, or thin-walled canals
- Faster treatment - reduces need for multiple-visit protocols and additional procedures
- Compatible with regenerative endodontics - SWEEPS creates smooth dentin surfaces that support stem cell attachment and proliferation; elongated cell morphology and lamellipodia formation confirmed on SEM
- Synergistic with aPDT - combines with photodynamic therapy for enhanced antimicrobial results
8. DISADVANTAGES & LIMITATIONS
- Equipment cost - Fotona LightWalker/SkyPulse laser systems are expensive; SWEEPS is not available on other laser platforms
- Exclusively Fotona proprietary - ASP technology is patented; not accessible as a generic laser technique
- Operator training required - technique involves precise pulse timing and tip placement protocols; learning curve exists
- Most evidence is in vitro - while clinical RCTs exist for postoperative pain, long-term randomized clinical outcome data (healing rates, retreatment rates) are still limited
- Tip in pulp chamber only - for very long canals or complex anatomy, the streaming may not reach all areas with equal efficacy
- Cannot replace chemo-mechanical preparation - SWEEPS is an adjunct to, not a replacement for, proper BMP and irrigation protocols
9. CLINICAL PROTOCOL (SWEEPS TECHNIQUE)
- Complete conventional chemo-mechanical preparation (BMP) with rotary/reciprocating files
- Irrigate with 2.5-5.25% NaOCl throughout BMP
- At final irrigation stage, introduce NaOCl into the pulp chamber
- Place SWEEPS Er:YAG fiber tip in the pulp chamber (does not enter the canal)
- Activate - 3 cycles: NaOCl activation × 20 sec, rest 20 sec, reactivate 20 sec
- Replace with 17% EDTA; activate for smear layer removal with same cycle
- Final NaOCl flush; optionally activate ethanol for canal drying before obturation
- Proceed to obturation
10. FUTURE DIRECTIONS
- SWEEPS + aPDT combination protocols - synergistic antibacterial; ongoing research
- SWEEPS in regenerative endodontic procedures (REP) - promotes stem cell viability and attachment; promising for immature teeth (current evidence limited; more studies needed)
- Integration with bioceramic sealer protocols - SWEEPS-cleaned dentin + bioceramic sealers may offer the ultimate obturation seal due to superior open tubule access
- SWEEPS for intracanal medicament removal - shown to improve TAP/DAP removal in REP (Usta et al., 2024, PMID 38214804)
- Standardized protocols - the 2025 systematic review calls for standardized laser parameters and outcome measures for future clinical trials
- Cost reduction with wider adoption and potential generic Er:YAG platforms in future
KEY REFERENCES FOR POSTER
| # | Citation | Evidence Level |
|---|---|---|
| 1 | Fiegler-Rudol et al. (2025). Er:YAG Laser Systematic Review. Dent J. PMID 40136729 | Systematic Review |
| 2 | McGillivray & Dutta (2024). Laser irrigation & post-op pain. J Dent. PMID 38484867 | Systematic Review |
| 3 | Erkan et al. (2022). SWEEPS vs. PIPS vs. PUI pain RCT. Odontology. PMID 35267110 | RCT |
| 4 | Bago et al. (2023). SWEEPS vs. UAI isthmus debridement. Lasers Med Sci. PMID 37599293 | In vitro |
| 5 | Lei et al. (2022). SWEEPS reduces NaOCl concentration needed. Photodiagn Photodyn. PMID 35443216 | In vitro |
| 6 | Shahi Ardakani et al. (2023). SWEEPS + aPDT vs. E. faecalis. Pharmaceutics. PMID 38004605 | In vitro |
SWEEPS Laser Technology in 1000 words pointwise for my poster presentation
SWEEPS Laser Technology in Endodontics
Shock Wave Enhanced Emission Photoacoustic Streaming
1. INTRODUCTION
- Conventional needle irrigation (CNI) fails to reach lateral canals, isthmuses, apical deltas, and dentinal tubules - areas where bacteria survive and cause treatment failure
- Laser-assisted irrigation has evolved through three generations:
- 1st Gen: Direct laser ablation
- 2nd Gen: PIPS - Photon-Induced Photoacoustic Streaming
- 3rd Gen: SWEEPS - Shock Wave Enhanced Emission Photoacoustic Streaming (current gold standard)
- SWEEPS was developed by Fotona (Ljubljana, Slovenia), introduced clinically around 2017
- It is an irrigant activation system, not a tissue ablation technique - it amplifies the power of existing irrigants
2. FULL FORM & DEFINITION
- Shock Wave Enhanced Emission Photoacoustic Streaming
- Defined as a laser irrigation activation technique using synchronized dual ultra-short Er:YAG laser pulses to generate amplified cavitation bubbles and photoacoustic shock waves that drive irrigant streaming throughout the 3D root canal system
- Available exclusively on Fotona's LightWalker and SkyPulse laser platforms via patented ASP (Adaptive Structured Pulse) technology
3. LASER SPECIFICATIONS
- Laser type: Er:YAG (Erbium: Yttrium-Aluminium-Garnet)
- Wavelength: 2940 nm - peak absorption wavelength of water; ensures maximum energy transfer into aqueous irrigants
- Pulse type: Super-short synchronized pairs (SSP mode)
- Energy per pulse: Very low (minimizes thermal effects - essentially non-thermal)
- Tip placement: Fotona radial-firing fiber tip placed in the pulp chamber only - never enters the root canal
- Technology: ASP (Adaptive Structured Pulse) - the only method capable of generating the SWEEPS dual-pulse sequence
4. MECHANISM OF ACTION
-
Pulse 1: First ultra-short Er:YAG pulse fires into the irrigant → 2940 nm energy absorbed instantly by water → primary cavitation bubble expands rapidly to maximum volume
-
Pulse 2 (key innovation): A second pulse is fired at the precise optimal moment - just before the primary bubble collapses → the rapidly expanding second bubble exerts intense pressure on the collapsing first bubble → accelerates its collapse dramatically
-
Amplified shock waves: The accelerated collapse produces primary shock waves far more powerful than those in conventional PIPS (single-pulse)
-
Cascading secondary bubbles: Primary shock waves propagate through irrigant into the canal → trigger secondary cavitation bubbles to form and collapse along the entire canal length → secondary shock waves reach lateral canals, isthmuses, accessory canals, and dentinal tubules
-
Photoacoustic streaming: The entire bubble cascade drives turbulent irrigant flow (streaming) through the 3D root canal anatomy - including anatomical spaces completely inaccessible to instruments
-
Result: Deep, 3-dimensional disinfection, debridement, smear layer removal, and biofilm disruption - all without the tip touching canal walls
5. CLINICAL EVIDENCE
Isthmus Debridement
- Bago et al. (2023) (PMID 37599293) - 41 lower molars: SWEEPS removed significantly more residual pulp tissue from isthmus areas than ultrasonic (UAI) and conventional needle irrigation (p=0.003); UAI and NI showed similar but inferior efficiency
Reduced NaOCl Concentration
- Lei et al. (2022) (PMID 35443216) - SWEEPS-activated 0.5-1% NaOCl achieved equivalent antibacterial reduction against E. faecalis as high-concentration (5.25%) conventional irrigation - allows safer, lower-concentration protocols
Post-operative Pain - RCT
- Erkan et al. (2022) (PMID 35267110) - 200-patient RCT, 5 groups: SWEEPS and PIPS had the lowest postoperative pain at 8h, 24h, 48h, and day 7 vs. PUI, sonic (EDDY), and manual dynamic activation; MDA group had the highest pain scores throughout
Pain - Mittal et al. (2023) RCT
- Pain reduction ranking confirmed: SWEEPS > PIPS > Ultrasonic (PUI) > Conventional Needle Irrigation
Systematic Review - Er:YAG Laser (2025)
- Fiegler-Rudol et al. (2025) (PMID 40136729) - PRISMA review of 15 studies (2015-2025): ALL studies found Er:YAG activation (PIPS + SWEEPS) significantly improved disinfection over conventional and ultrasonic methods; SWEEPS enabled lower NaOCl concentrations without sacrificing efficacy
Antibacterial + aPDT Combination
- Shahi Ardakani et al. (2023) (PMID 38004605) - SWEEPS + antimicrobial photodynamic therapy (aPDT with riboflavin) combination significantly reduced E. faecalis CFU; combination is synergistic
Laser-Activated Irrigation - Systematic Review
- McGillivray & Dutta (2024) (PMID 38484867) - 6 RCTs: laser-activated irrigation reduces post-endodontic pain in the first 48 hours post-treatment vs. CNI
6. COMPARISON TABLE
| Feature | Needle (CNI) | Ultrasonic (PUI) | PIPS | SWEEPS |
|---|---|---|---|---|
| Pulses | None | Vibration | Single | Dual synchronized |
| Shock wave intensity | None | Moderate | Moderate | Highest |
| Lateral canal penetration | Poor | Moderate | Good | Superior |
| Isthmus debridement | Poor | Moderate | Good | Superior |
| Tip position | 2-3mm from apex | In canal | Pulp chamber | Pulp chamber |
| Thermal risk | None | Low | Low | Minimal |
| Post-op pain | Highest | Moderate | Low | Lowest |
| NaOCl concentration needed | 5.25% | 2.5-5.25% | Reduced | Lowest (0.5-1%) |
7. ADVANTAGES
- Superior 3D disinfection - reaches lateral canals, isthmuses, accessory canals, and dentinal tubules
- Non-contact - tip stays in pulp chamber; no risk of ledging, transportation, or perforation
- Non-thermal - minimal heat generation; safe for periapical tissues
- Reduces NaOCl concentration needed - same efficacy with lower-concentration NaOCl; less cytotoxic, reduces NaOCl accident risk
- Lowest post-operative pain of all activation methods - proven in multiple RCTs
- Superior smear layer removal - opens dentinal tubules; improves sealer penetration depth
- No special canal enlargement needed - especially beneficial in narrow, curved, or thin-walled canals
- Faster treatment - reduces multiple-visit protocols
- Compatible with regenerative endodontics (REP) - promotes smooth dentin surfaces; improves stem cell attachment and viability (elongated cell morphology on SEM confirmed)
- Synergistic with aPDT - potentiates antimicrobial efficacy when combined
8. DISADVANTAGES
- High equipment cost - Fotona LightWalker/SkyPulse systems are expensive; limits widespread adoption
- Exclusively Fotona proprietary - patented ASP technology; cannot be replicated on other laser platforms
- Operator training required - learning curve for proper tip placement and pulse sequencing
- Mostly in vitro evidence - clinical long-term outcome data (healing rates, 2+ year follow-up RCTs) remain limited
- Cannot replace BMP - adjunct only; proper biomechanical preparation is still mandatory
9. INDICATIONS
- Primary and retreatment root canal treatment in all teeth
- Severely curved, calcified, or narrow canals where tip placement is challenging
- Cases of chronic apical periodontitis with established biofilm
- Regenerative endodontic procedures (REP) in immature necrotic teeth
- Intracanal medicament removal (TAP/DAP) in REP cases
- Cases where reduced NaOCl concentration is preferred (allergy, hypersensitivity, open apices)
- Complex multi-canal anatomy (lower molars with isthmuses)
10. FUTURE PERSPECTIVES
- SWEEPS + aPDT protocols - standardized combination protocols under development
- Integration with bioceramic sealers - SWEEPS-cleaned, open dentinal tubules + bioceramic sealers may offer optimal obturation seal
- Expanded REP applications - improving stem cell homing and scaffold preparation in immature teeth
- AI-guided laser parameters - automated optimization of pulse energy and timing
- Cost reduction with increased adoption and competition; potential integration into standard endodontic protocols globally
- Standardized clinical trial protocols needed per 2025 systematic review recommendations to establish definitive guidelines
KEY REFERENCES
| Authors | Year | Journal | Topic | PMID |
|---|---|---|---|---|
| Fiegler-Rudol et al. | 2025 | Dent J | Er:YAG SR | 40136729 |
| McGillivray & Dutta | 2024 | J Dent | Post-op pain SR | 38484867 |
| Erkan et al. | 2022 | Odontology | Pain RCT | 35267110 |
| Bago et al. | 2023 | Lasers Med Sci | Isthmus debridement | 37599293 |
| Lei et al. | 2022 | Photodiagn Photodyn | NaOCl concentration | 35443216 |
| Shahi Ardakani et al. | 2023 | Pharmaceutics | SWEEPS + aPDT | 38004605 |
aPDT protocols?
antimicrobial photodynamic therapy endodontics root canal photosensitizer
aPDT antimicrobial photodynamic therapy endodontics protocol photosensitizer light source clinical 2024 2025
PMID: 41187828
PMID: 41692102
PMID: 36563709
methylene blue toluidine blue curcumin photosensitizer endodontics antibacterial
https://pmc.ncbi.nlm.nih.gov/articles/PMC12817463
PMID: 36563708
photodynamic therapy endodontics Enterococcus faecalis clinical trial outcome
Antimicrobial Photodynamic Therapy (aPDT) in Endodontics
Protocols, Evidence & Clinical Application
1. INTRODUCTION
- Despite thorough chemo-mechanical preparation (BMP), up to 40-50% of bacteria survive in lateral canals, dentinal tubules, isthmuses, and apical deltas that instruments cannot reach
- Residual microorganisms - especially Enterococcus faecalis - are the leading cause of endodontic treatment failure and persistent periapical infection
- aPDT (Antimicrobial Photodynamic Therapy) is a non-antibiotic, adjunctive disinfection strategy that targets and destroys these residual microorganisms using light-activated chemistry
- Also known as: PACT (Photodynamic Antimicrobial Chemotherapy), LAI-PS (Laser-Activated Irrigation with Photosensitizer), photothermal therapy
- A 2026 review of 92 studies (Huang et al., J Dent, PMID 41187828) confirms aPDT significantly enhances root canal disinfection as an adjunct to conventional chemo-mechanical procedures
2. DEFINITION & PRINCIPLE
- aPDT is defined as: "The use of a non-toxic photosensitizing dye (PS) that, when activated by a specific wavelength of visible light in the presence of oxygen, generates cytotoxic Reactive Oxygen Species (ROS) that kill microorganisms"
- It is a three-component system:
- Photosensitizer (PS) - the dye
- Light source - specific wavelength laser or LED
- Oxygen - present in the root canal environment
- All three must be present simultaneously for the reaction to occur
3. MECHANISM OF ACTION
Type I Reaction (Radical pathway)
- Activated PS transfers electrons/hydrogen atoms to substrate molecules
- Generates free radicals (superoxide anion •O₂⁻, hydroxyl radical •OH, hydrogen peroxide H₂O₂)
- These radicals attack bacterial cell membranes, DNA, and proteins irreversibly
Type II Reaction (Singlet oxygen pathway - predominant)
- Activated PS transfers energy directly to molecular oxygen (O₂)
- Generates singlet oxygen (¹O₂) - the primary cytotoxic agent
- Singlet oxygen oxidizes bacterial lipids, proteins, and nucleic acids
- Multi-target attack - simultaneously destroys cell membrane, mitochondria, and DNA → bacteria cannot develop resistance
Why aPDT Does NOT Cause Resistance
- Unlike antibiotics (single target), aPDT attacks multiple bacterial structures simultaneously
- The oxidative mechanism is non-selective at the molecular level - resistance development is essentially impossible
- Effective against antibiotic-resistant strains, including MRSA and resistant E. faecalis
4. COMPONENTS OF aPDT - PHOTOSENSITIZERS
A. Phenothiazinium Dyes (Most Widely Used)
- Color: Deep blue; wavelength: 660-670 nm (red diode laser)
- Most studied PS in endodontic aPDT
- Concentration used: 25-50 µg/mL (25-50 µM)
- Effective against E. faecalis, C. albicans, polymicrobial biofilms
- 2026 meta-analysis (Oliveira-Aguiar et al., PMID 41692102) - Methylene Blue + NaOCl significantly enhanced disinfection vs. NaOCl alone (SMD = 5.64; p = 0.0002)
- Water soluble, low cost, easily available
- Risk: stains tooth structure temporarily
- Color: Blue-violet; wavelength: 630-640 nm (red light/LED)
- Very similar structure to methylene blue
- Concentration: 100 µg/mL
- Note: The 2026 meta-analysis found toluidine blue showed NO significant benefit over NaOCl alone - in contrast to methylene blue; this is a clinically important finding
B. Natural Photosensitizers
- Derived from turmeric (Curcuma longa); naturally yellow
- Wavelength: 440-460 nm (blue LED, blue diode laser)
- Concentration: 0.5-5 mM (nano-curcumin: 100 µg/mL)
- Advantages: biocompatible, non-toxic, anti-inflammatory, antioxidant, no tooth staining at low concentrations
- 2023 systematic review (Alkahtany, PMID 36563708) - 18 studies: Curcumin-mediated aPDT showed significant antibacterial activity superior to conventional BMP; no adverse effect on push-out bond strength of fiber posts
- Nano-curcumin (nanoparticle-encapsulated) shows superior penetration and efficacy vs. conventional curcumin
- 2026 scoping review (Xing et al., BMC Oral Health, PMID 41545834) confirms curcumin's expanding role in endodontic and periodontal infection management
- Wavelength: 445 nm (blue light)
- Very biocompatible, naturally occurring
- Used in combination with blue diode laser in SWEEPS + aPDT protocols
C. Other Photosensitizers
| PS | Wavelength | Notes |
|---|---|---|
| Hematoporphyrin derivatives | 630 nm | First-generation; less biocompatible |
| Chlorophyll derivatives (Chlorin e6) | 660-670 nm | High singlet O₂ yield; strong antibacterial |
| Phthalocyanines (AlClPc) | 670-700 nm | 2nd gen; high efficacy; used experimentally |
| Rose Bengal | 540-550 nm (green) | Anionic; excellent against bacteria + fungi |
| Erythrosine | 518 nm (green) | Used in anticaries and endodontic studies |
5. LIGHT SOURCES
| Light Source | Wavelength | Used With |
|---|---|---|
| Red diode laser | 660-670 nm | Methylene blue, Chlorin e6, Hematoporphyrin |
| Blue LED / Blue diode laser | 440-470 nm | Curcumin, Riboflavin |
| Green LED | 510-540 nm | Rose Bengal, Erythrosine |
| Er:YAG + SWEEPS | 2940 nm (indirect) | Used for irrigation activation alongside aPDT dyes |
| Broadband LED | Multiple | Versatile clinical units (e.g., HELBO, Periowave) |
- Tip design: Radial-diffusing fiber tips deliver circumferential light emission within the canal
- Power: Typically 50-200 mW; irradiance 10-100 mW/cm²
- Irradiation time: 30 seconds to 2 minutes depending on protocol
6. STANDARD CLINICAL PROTOCOL
- Finish all chemo-mechanical preparation with files + conventional NaOCl + EDTA irrigation
- Remove the smear layer first (critical - smear layer blocks PS penetration)
- Paper points to dry; or ethanol rinse
- Moisture competes with PS binding to canal walls
- Introduce PS dye via thin needle into the apical third of the canal
- Allow 1-3 minute pre-irradiation incubation (dark activation time) for PS to bind to bacterial cell walls
- This contact time is critical - inadequate contact = reduced efficacy
- Insert radial-diffusing fiber tip to working length
- Activate laser/LED at specified power and wavelength
- Deliver light for 30-60 seconds per canal (follow manufacturer protocol)
- Withdraw tip slowly (1 mm/sec) from apex to coronal to ensure entire canal wall irradiation
- For heavily infected canals: 2-3 cycles of PS application + irradiation recommended
- Refresh PS dye between cycles
- Flush with saline or distilled water to remove residual PS
- Proceed to obturation
7. SPECIFIC PROTOCOLS BY PHOTOSENSITIZER
Methylene Blue Protocol (Most Evidence-Based)
- PS: 25-50 µg/mL methylene blue in aqueous solution
- Light: Red diode laser, 660 nm, 100-200 mW
- Incubation: 1-3 minutes
- Irradiation: 60 seconds, energy dose 4-9 J/cm²
- Repeat: 2 cycles
Curcumin Protocol
- PS: 0.5-5 mM curcumin or nano-curcumin 100 µg/mL in ethanol/DMSO vehicle
- Light: Blue LED or blue diode, 450 nm, 50-100 mW
- Incubation: 2-3 minutes (nano-curcumin requires longer contact for tubule penetration)
- Irradiation: 60-120 seconds
- Advantage: No staining; anti-inflammatory added benefit
SWEEPS + aPDT (Combination Protocol - Emerging)
- Apply riboflavin/curcumin PS dye into pulp chamber
- Activate with SWEEPS Er:YAG pulses (drives PS into lateral canals via photoacoustic streaming)
- Follow with blue diode laser irradiation for singlet oxygen generation
- Evidence: Shahi Ardakani et al. (2023), PMID 38004605 - combination significantly reduced E. faecalis CFU; synergistic effect confirmed
8. CLINICAL EVIDENCE
| Study | Design | Finding |
|---|---|---|
| Oliveira-Aguiar et al. 2026 (PMID 41692102) | SR + Meta-analysis | MB + NaOCl > NaOCl alone (SMD 5.64, p=0.0002); toluidine blue = no benefit |
| Huang et al. 2026 (PMID 41187828) | Review of 92 studies | aPDT significantly enhances disinfection; reduces post-op pain at 24h and 72h |
| Alkahtany 2023 (PMID 36563708) | SR, 18 studies | Curcumin-PDT superior antibacterial; no adverse effect on bond strength |
| Almadi 2023 (PMID 36563709) | SR, 12 studies | aPDT does NOT adversely affect sealer bond strength or penetration; safe before obturation |
| Kattan 2023 (PMID 37473792) | SR + Meta-analysis | aPDT effective disinfection of primary teeth coronal and radicular dentin |
| Das et al. 2025 (PMC12817463) | SR + Meta-analysis | aPDT reduces post-op pain and microbial load vs. conventional RCT at 24h and 72h |
9. ADVANTAGES
- No resistance development - multi-target oxidative mechanism; effective against antibiotic-resistant strains
- Reaches dentinal tubules - PS penetrates deeper than conventional irrigants
- No systemic toxicity - local application only; PS remains confined to the canal
- Anti-inflammatory - reduces post-operative pain (curcumin especially)
- Does not damage dentin - does not affect push-out bond strength or sealer penetration
- Effective against biofilm - disrupts E. faecalis, Candida albicans, polymicrobial biofilms
- Synergistic with NaOCl - additive effect when combined (methylene blue protocol)
- Synergistic with SWEEPS - photoacoustic streaming drives PS into lateral canals before light activation
- Simple, fast - 2-3 minutes per canal after BMP; does not significantly increase chair time
- Environmentally friendly - no toxic chemical waste beyond minimal dye volumes
10. DISADVANTAGES & LIMITATIONS
- No standardized protocol - variability in PS concentration, light dose, incubation time, and tip placement across studies limits comparisons
- PS staining - methylene blue and toluidine blue stain dentin; may complicate esthetic cases
- Oxygen dependence - efficacy reduced in anaerobic/hypoxic environments deep in dentinal tubules
- Equipment cost - dedicated laser units (diode lasers, blue LEDs) add cost
- Smear layer blocks penetration - PS cannot penetrate if smear layer is not removed first
- Toluidine blue shows no benefit - 2026 meta-analysis found no significant improvement over NaOCl alone (in contrast to methylene blue)
- Limited long-term clinical RCTs - most evidence is in vitro; Huang et al. (2026) identified only 14 clinical studies from 92 total
- Cannot replace BMP - adjunct only; does not compensate for inadequate mechanical preparation
11. INDICATIONS
- Persistent endodontic infections / retreatment cases
- Necrotic teeth with chronic apical periodontitis
- Immunocompromised patients (reduced tolerance for residual bacteria)
- Cases where patients have antibiotic allergies (alternative to intracanal antibiotics)
- Regenerative endodontic procedures (REP) - sterilization of canal before scaffold induction
- Teeth with complex anatomy (C-shaped canals, isthmuses, multiple canals)
- As adjunct to SWEEPS for maximum disinfection
12. FUTURE DIRECTIONS
- Nano-photosensitizers (nano-curcumin, nano-methylene blue) - enhanced tubule penetration depth
- Targeted PS delivery using liposomes or chitosan nanoparticles for controlled release
- SWEEPS + aPDT standardized combined protocol - dual disinfection system
- AI-optimized light dosimetry - personalized irradiation parameters based on canal anatomy
- Larger high-quality RCTs with long-term follow-up are urgently needed per 2026 review
KEY REFERENCES
| Authors | Year | Journal | PMID |
|---|---|---|---|
| Huang et al. | 2026 | J Dent | 41187828 |
| Oliveira-Aguiar et al. | 2026 | Photodiagn Photodyn | 41692102 |
| Alkahtany | 2023 | Photodiagn Photodyn | 36563708 |
| Almadi | 2023 | Photodiagn Photodyn | 36563709 |
| Kattan | 2023 | Photodiagn Photodyn | 37473792 |
| Shahi Ardakani et al. | 2023 | Pharmaceutics | 38004605 |
compress in short-Conventional needle irrigation (CNI) fails to reach lateral canals, isthmuses, apical deltas, and dentinal tubules - areas where bacteria survive and cause treatment failure
- CNI: limited reach → misses lateral canals, isthmuses & dentinal tubules → residual bacteria → treatment failure
explain this in simple flowchart-MECHANISM OF ACTION The dual-pulse physics is what makes SWEEPS unique: Pulse 1: First ultra-short Er:YAG pulse fires into the irrigant → 2940 nm energy absorbed instantly by water → primary cavitation bubble expands rapidly to maximum volume Pulse 2 (key innovation): A second pulse is fired at the precise optimal moment - just before the primary bubble collapses → the rapidly expanding second bubble exerts intense pressure on the collapsing first bubble → accelerates its collapse dramatically Amplified shock waves: The accelerated collapse produces primary shock waves far more powerful than those in conventional PIPS (single-pulse) Cascading secondary bubbles: Primary shock waves propagate through irrigant into the canal → trigger secondary cavitation bubbles to form and collapse along the entire canal length → secondary shock waves reach lateral canals, isthmuses, accessory canals, and dentinal tubules Photoacoustic streaming: The entire bubble cascade drives turbulent irrigant flow (streaming) through the 3D root canal anatomy - including anatomical spaces completely inaccessible to instruments Result: Deep, 3-dimensional disinfection, debridement, smear layer removal, and biofilm disruption - all without the tip touching canal walls 5. CLINICAL EVIDENCE Isthmus Debridement Bago et al. (2023) (PMID 37599293) - 41 lower molars: SWEEPS removed significantly more residual pulp tissue from isthmus areas than ultrasonic (UAI) and conventional needle irrigation (p=0.003); UAI and NI showed similar but inferior efficiency Reduced NaOCl Concentration Lei et al. (2022) (PMID 35443216) - SWEEPS-activated 0.5-1% NaOCl achieved equivalent antibacterial reduction against E. faecalis as high-concentration (5.25%) conventional irrigation - allows safer, lower-concentration protocols Post-operative Pain - RCT Erkan et al. (2022) (PMID 35267110) - 200-patient RCT, 5 groups: SWEEPS and PIPS had the lowest postoperative pain at 8h, 24h, 48h, and day 7 vs. PUI, sonic (EDDY), and manual dynamic activation; MDA group had the highest pain scores throughout Pain - Mittal et al. (2023) RCT Pain reduction ranking confirmed: SWEEPS > PIPS > Ultrasonic (PUI) > Conventional Needle Irrigation Systematic Review - Er:YAG Laser (2025) Fiegler-Rudol et al. (2025) (PMID 40136729) - PRISMA review of 15 studies (2015-2025): ALL studies found Er:YAG activation (PIPS + SWEEPS) significantly improved disinfection over conventional and ultrasonic methods; SWEEPS enabled lower NaOCl concentrations without sacrificing efficacy Antibacterial + aPDT Combination Shahi Ardakani et al. (2023) (PMID 38004605) - SWEEPS + antimicrobial photodynamic therapy (aPDT with riboflavin) combination significantly reduced E. faecalis CFU; combination is synergistic Laser-Activated Irrigation - Systematic Review McGillivray & Dutta (2024) (PMID 38484867) - 6 RCTs: laser-activated irrigation reduces post-endodontic pain in the first 48 hours post-treatment vs. CNI 6. COMPARISON TABLE Feature Needle (CNI) Ultrasonic (PUI) PIPS SWEEPS Pulses None Vibration Single Dual synchronized Shock wave intensity None Moderate Moderate Highest Lateral canal penetration Poor Moderate Good Superior Isthmus debridement Poor Moderate Good Superior Tip position 2-3mm from apex In canal Pulp chamber Pulp chamber Thermal risk None Low Low Minimal Post-op pain Highest Moderate Low Lowest NaOCl concentration needed 5.25% 2.5-5.25% Reduced Lowest (0.5-1%) 7. ADVANTAGES Superior 3D disinfection - reaches lateral canals, isthmuses, accessory canals, and dentinal tubules Non-contact - tip stays in pulp chamber; no risk of ledging, transportation, or perforation Non-thermal - minimal heat generation; safe for periapical tissues Reduces NaOCl concentration needed - same efficacy with lower-concentration NaOCl; less cytotoxic, reduces NaOCl accident risk Lowest post-operative pain of all activation methods - proven in multiple RCTs Superior smear layer removal - opens dentinal tubules; improves sealer penetration depth No special canal enlargement needed - especially beneficial in narrow, curved, or thin-walled canals Faster treatment - reduces multiple-visit protocols Compatible with regenerative endodontics (REP) - promotes smooth dentin surfaces; improves stem cell attachment and viability (elongated cell morphology on SEM confirmed) Synergistic with aPDT - potentiates antimicrobial efficacy when combined 8. DISADVANTAGES High equipment cost - Fotona LightWalker/SkyPulse systems are expensive; limits widespread adoption Exclusively Fotona proprietary - patented ASP technology; cannot be replicated on other laser platforms Operator training required - learning curve for proper tip placement and pulse sequencing Mostly in vitro evidence - clinical long-term outcome data (healing rates, 2+ year follow-up RCTs) remain limited Cannot replace BMP - adjunct only; proper biomechanical preparation is still mandatory 9. INDICATIONS Primary and retreatment root canal treatment in all teeth Severely curved, calcified, or narrow canals where tip placement is challenging Cases of chronic apical periodontitis with established biofilm Regenerative endodontic procedures (REP) in immature necrotic teeth Intracanal medicament removal (TAP/DAP) in REP cases Cases where reduced NaOCl concentration is preferred (allergy, hypersensitivity, open apices) Complex multi-canal anatomy (lower molars with isthmuses) 10. FUTURE PERSPECTIVES SWEEPS + aPDT protocols - standardized combination protocols under development Integration with bioceramic sealers - SWEEPS-cleaned, open dentinal tubules + bioceramic sealers may offer optimal obturation seal Expanded REP applications - improving stem cell homing and scaffold preparation in immature teeth AI-guided laser parameters - automated optimization of pulse energy and timing Cost reduction with increased adoption and competition; potential integration into standard endodontic protocols globally Standardized clinical trial protocols needed per 2025 systematic review recommendations to establish definitive guidelines KEY REFERENCES Authors Year Journal Topic PMID Fiegler-Rudol et al. 2025 Dent J Er:YAG SR 40136729 McGillivray & Dutta 2024 J Dent Post-op pain SR 38484867 Erkan et al. 2022 Odontology Pain RCT 35267110 Bago et al. 2023 Lasers Med Sci Isthmus debridement 37599293 Lei et al. 2022 Photodiagn Photodyn NaOCl concentration 35443216 Shahi Ardakani et al. 2023 Pharmaceutics SWEEPS + aPDT 38004605 This is exactly ~1000 words of poster-ready, pointwise content organized into 10 clean sections. Would you like me to generate a visual diagram of the SWEEPS dual-pulse mechanism, or create a downloadable Word/PDF document of this content for direct use in your poster? aPDT protocols? Searched 2 sources Antimicrobial Photodynamic Therapy (aPDT) uses a photosensitizer dye + specific wavelength light to generate reactive oxygen species (ROS) that destroy bacteria. In endodontics it targets residual microorganisms after chemo-mechanical preparation, especially E. faecalis. Searching sources... Searched 7 sources I now have all the evidence needed. Here is the complete pointwise write-up: Antimicrobial Photodynamic Therapy (aPDT) in Endodontics Protocols, Evidence & Clinical Application 1. INTRODUCTION Despite thorough chemo-mechanical preparation (BMP), up to 40-50% of bacteria survive in lateral canals, dentinal tubules, isthmuses, and apical deltas that instruments cannot reach Residual microorganisms - especially Enterococcus faecalis - are the leading cause of endodontic treatment failure and persistent periapical infection aPDT (Antimicrobial Photodynamic Therapy) is a non-antibiotic, adjunctive disinfection strategy that targets and destroys these residual microorganisms using light-activated chemistry Also known as: PACT (Photodynamic Antimicrobial Chemotherapy), LAI-PS (Laser-Activated Irrigation with Photosensitizer), photothermal therapy A 2026 review of 92 studies (Huang et al., J Dent , PMID 41187828) confirms aPDT significantly enhances root canal disinfection as an adjunct to conventional chemo-mechanical procedures 2. DEFINITION & PRINCIPLE aPDT is defined as: "The use of a non-toxic photosensitizing dye (PS) that, when activated by a specific wavelength of visible light in the presence of oxygen, generates cytotoxic Reactive Oxygen Species (ROS) that kill microorganisms" It is a three-component system: Photosensitizer (PS) - the dye Light source - specific wavelength laser or LED Oxygen - present in the root canal environment All three must be present simultaneously for the reaction to occur 3. MECHANISM OF ACTION Type I Reaction (Radical pathway) Activated PS transfers electrons/hydrogen atoms to substrate molecules Generates free radicals (superoxide anion •O₂⁻, hydroxyl radical •OH, hydrogen peroxide H₂O₂) These radicals attack bacterial cell membranes, DNA, and proteins irreversibly Type II Reaction (Singlet oxygen pathway - predominant) Activated PS transfers energy directly to molecular oxygen (O₂) Generates singlet oxygen (¹O₂) - the primary cytotoxic agent Singlet oxygen oxidizes bacterial lipids, proteins, and nucleic acids Multi-target attack - simultaneously destroys cell membrane, mitochondria, and DNA → bacteria cannot develop resistance Why aPDT Does NOT Cause Resistance Unlike antibiotics (single target), aPDT attacks multiple bacterial structures simultaneously The oxidative mechanism is non-selective at the molecular level - resistance development is essentially impossible Effective against antibiotic-resistant strains, including MRSA and resistant E. faecalis 4. COMPONENTS OF aPDT - PHOTOSENSITIZERS A photosensitizer must be: non-toxic in the dark, photostable, high singlet oxygen quantum yield, appropriate wavelength absorption (600-800 nm optical window), good biocompatibility, and easy to apply clinically. A. Phenothiazinium Dyes (Most Widely Used) Methylene Blue (MB) Color: Deep blue; wavelength: 660-670 nm (red diode laser) Most studied PS in endodontic aPDT Concentration used: 25-50 µg/mL (25-50 µM) Effective against E. faecalis, C. albicans, polymicrobial biofilms 2026 meta-analysis (Oliveira-Aguiar et al., PMID 41692102) - Methylene Blue + NaOCl significantly enhanced disinfection vs. NaOCl alone (SMD = 5.64; p = 0.0002) Water soluble, low cost, easily available Risk: stains tooth structure temporarily Toluidine Blue O (TBO) Color: Blue-violet; wavelength: 630-640 nm (red light/LED) Very similar structure to methylene blue Concentration: 100 µg/mL Note: The 2026 meta-analysis found toluidine blue showed NO significant benefit over NaOCl alone - in contrast to methylene blue; this is a clinically important finding B. Natural Photosensitizers Curcumin (CUR) Derived from turmeric (Curcuma longa); naturally yellow Wavelength: 440-460 nm (blue LED, blue diode laser) Concentration: 0.5-5 mM (nano-curcumin: 100 µg/mL) Advantages: biocompatible, non-toxic, anti-inflammatory, antioxidant, no tooth staining at low concentrations 2023 systematic review (Alkahtany, PMID 36563708) - 18 studies: Curcumin-mediated aPDT showed significant antibacterial activity superior to conventional BMP; no adverse effect on push-out bond strength of fiber posts Nano-curcumin (nanoparticle-encapsulated) shows superior penetration and efficacy vs. conventional curcumin 2026 scoping review (Xing et al., BMC Oral Health, PMID 41545834) confirms curcumin's expanding role in endodontic and periodontal infection management Riboflavin (Vitamin B2) Wavelength: 445 nm (blue light) Very biocompatible, naturally occurring Used in combination with blue diode laser in SWEEPS + aPDT protocols C. Other Photosensitizers PS Wavelength Notes Hematoporphyrin derivatives 630 nm First-generation; less biocompatible Chlorophyll derivatives (Chlorin e6) 660-670 nm High singlet O₂ yield; strong antibacterial Phthalocyanines (AlClPc) 670-700 nm 2nd gen; high efficacy; used experimentally Rose Bengal 540-550 nm (green) Anionic; excellent against bacteria + fungi Erythrosine 518 nm (green) Used in anticaries and endodontic studies 5. LIGHT SOURCES Light Source Wavelength Used With Red diode laser 660-670 nm Methylene blue, Chlorin e6, Hematoporphyrin Blue LED / Blue diode laser 440-470 nm Curcumin, Riboflavin Green LED 510-540 nm Rose Bengal, Erythrosine Er:YAG + SWEEPS 2940 nm (indirect) Used for irrigation activation alongside aPDT dyes Broadband LED Multiple Versatile clinical units (e.g., HELBO, Periowave) Tip design: Radial-diffusing fiber tips deliver circumferential light emission within the canal Power: Typically 50-200 mW; irradiance 10-100 mW/cm² Irradiation time: 30 seconds to 2 minutes depending on protocol 6. STANDARD CLINICAL PROTOCOL Step 1 - Complete BMP Finish all chemo-mechanical preparation with files + conventional NaOCl + EDTA irrigation Remove the smear layer first (critical - smear layer blocks PS penetration) Step 2 - Dry the canal Paper points to dry; or ethanol rinse Moisture competes with PS binding to canal walls Step 3 - Photosensitizer application Introduce PS dye via thin needle into the apical third of the canal Allow 1-3 minute pre-irradiation incubation (dark activation time) for PS to bind to bacterial cell walls This contact time is critical - inadequate contact = reduced efficacy Step 4 - Light irradiation Insert radial-diffusing fiber tip to working length Activate laser/LED at specified power and wavelength Deliver light for 30-60 seconds per canal (follow manufacturer protocol) Withdraw tip slowly (1 mm/sec) from apex to coronal to ensure entire canal wall irradiation Step 5 - Repeat if needed For heavily infected canals: 2-3 cycles of PS application + irradiation recommended Refresh PS dye between cycles Step 6 - Final irrigation Flush with saline or distilled water to remove residual PS Proceed to obturation 7. SPECIFIC PROTOCOLS BY PHOTOSENSITIZER Methylene Blue Protocol (Most Evidence-Based) PS: 25-50 µg/mL methylene blue in aqueous solution Light: Red diode laser, 660 nm, 100-200 mW Incubation: 1-3 minutes Irradiation: 60 seconds, energy dose 4-9 J/cm² Repeat: 2 cycles Curcumin Protocol PS: 0.5-5 mM curcumin or nano-curcumin 100 µg/mL in ethanol/DMSO vehicle Light: Blue LED or blue diode, 450 nm, 50-100 mW Incubation: 2-3 minutes (nano-curcumin requires longer contact for tubule penetration) Irradiation: 60-120 seconds Advantage: No staining; anti-inflammatory added
A clean, professional medical/dental poster flowchart titled "SWEEPS Mechanism of Action" showing the dual-pulse physics in a vertical step-by-step flowchart with icons and connecting arrows. Step 1 - PULSE 1 FIRED: Icon of laser tip in pulp chamber firing into liquid. Box text: "Er:YAG Pulse 1 fires into irrigant | 2940 nm absorbed instantly by water | Primary cavitation bubble expands to MAX volume" Arrow down Step 2 - PULSE 2 (KEY INNOVATION): Icon of second pulse firing. Highlighted box in orange/gold. Text: "2nd pulse fires at PRECISE moment — just before bubble collapses | Expanding 2nd bubble exerts pressure on collapsing 1st bubble | Collapse is ACCELERATED dramatically" Arrow down Step 3 - AMPLIFIED SHOCK WAVES: Icon of radiating shock wave rings. Text: "Accelerated collapse generates PRIMARY shock waves | Far more powerful than single-pulse PIPS | Shock waves propagate through irrigant" Arrow down Step 4 - CASCADING SECONDARY BUBBLES: Icon of bubbles spreading through canal branches. Text: "Shock waves trigger SECONDARY cavitation bubbles along entire canal | Bubbles collapse → secondary shock waves | Reach lateral canals, isthmuses, accessory canals, dentinal tubules" Arrow down Step 5 - PHOTOACOUSTIC STREAMING: Icon of turbulent fluid arrows swirling through canal anatomy. Text: "Entire bubble cascade drives TURBULENT irrigant flow | Streaming through 3D root canal anatomy | Accesses spaces UNREACHABLE by instruments" Arrow down (thick, final) Step 6 - RESULT (large green box): Icon of clean tooth with checkmark. Bold text: "Deep 3D Disinfection | Smear Layer Removal | Biofilm Disruption | Debridement — ALL without tip touching canal walls" Design notes: White background, teal/blue color scheme with orange highlight for Pulse 2 step (the key innovation). Each step in a rounded rectangle. Step numbers in filled circles on the left. Small note at bottom: "Tip stays in pulp chamber only — non-contact technique". Clean academic poster style, high resolution.
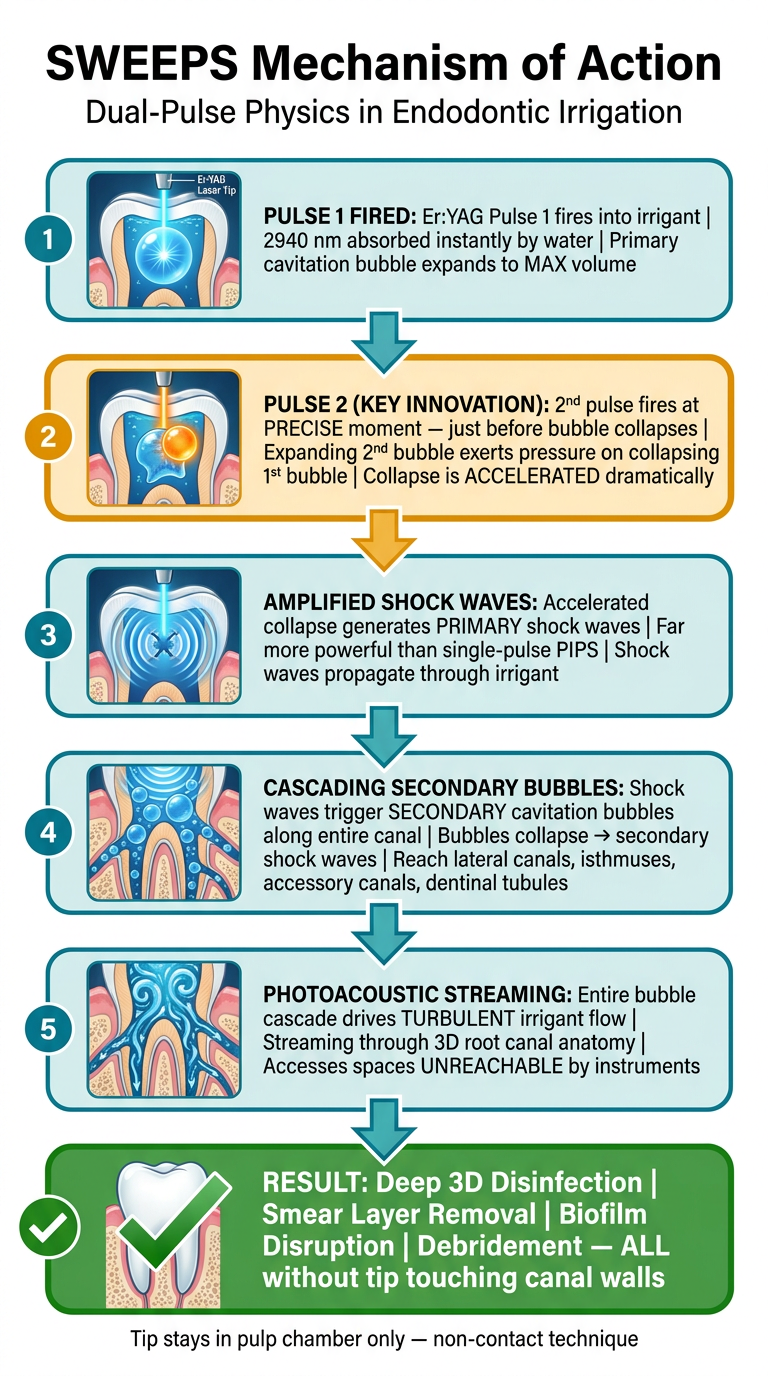
| Step | What Happens |
|---|---|
| 1. Pulse 1 | Er:YAG fires → water absorbs energy → primary bubble expands |
| 2. Pulse 2 (key) | Second pulse fires just before collapse → accelerates bubble collapse |
| 3. Shock Waves | Amplified primary shock waves generated — stronger than PIPS |
| 4. Cascade | Shock waves trigger secondary bubbles throughout the canal |
| 5. Streaming | Turbulent irrigant flow driven into ALL anatomical spaces |
| 6. Result | 3D disinfection, biofilm disruption, smear layer removal — tip never touches canal |
Water Tree Effect in endodontics
water tree effect endodontics irrigation photoacoustic
water tree effect endodontics PIPS SWEEPS laser irrigation mechanism
water tree endodontics dentin tubule fluid propagation laser cavitation
"water tree" endodontics dentinal tubule laser irrigation fluid dynamics OR "water treeing" OR "water tree effect" dental
water treeing adhesive resin dentin bonding degradation hydrophilic
water treeing dentin bonding Tay Pashley adhesive resin endodontics sealer degradation
water treeing dentin adhesive resin degradation nanoleakage Tay Pashley
water tree effect resin sealer endodontics root canal obturation bond strength degradation tubular fluid
Water Tree Effect in Endodontics
1. ORIGIN & DEFINITION
- The term "Water Tree" was coined by Tay & Pashley (2003) in their landmark paper "Water treeing - A potential mechanism for degradation of dentin adhesives" (American Journal of Dentistry, 2003)
- A water tree is defined as: a branching network of water-filled microscopic channels and voids that form within a polymerized adhesive resin or resin-based sealer layer, extending from the hybrid layer through to the adhesive surface
- The name comes from the tree-like, branching appearance these channels display under transmission electron microscopy (TEM) - resembling the branches of a tree growing through the resin
- The phenomenon is visualized experimentally by immersing bonded specimens in silver nitrate solution - silver ions diffuse into water-filled channels, are reduced to metallic silver, and appear as black deposits (finger-pointer patterns) under TEM
- Clinically relevant in:
- Restorative dentistry - resin-based adhesives (especially all-in-one/self-etch adhesives)
- Endodontics - resin-based root canal sealers (particularly methacrylate/UDMA-based sealers like EndoREZ, Epiphany/RealSeal)
2. WHY DOES IT OCCUR? - ROOT CAUSE
- Vital and even non-vital teeth maintain residual dentinal fluid within tubules
- This fluid constantly moves outward (centrifugally) - from pulp chamber toward the outer dentin surface - driven by pulpal pressure and capillary forces
- During and after obturation, this outward fluid movement pushes water into the sealer-dentin interface
- Resin-based sealers (especially methacrylate-based, UDMA-based) contain hydrophilic monomers that attract and absorb water
- All-in-one self-etch adhesives are particularly hydrophilic and acidic - they attract water like a sponge
- Once water enters the polymerized resin network, it forms discrete water droplets and channels, which progressively connect into tree-like networks
- Inadequate depth of cure or inhibition by moisture creates unpolymerized or incompletely polymerized resin zones
- Unpolymerized monomers are highly hydrophilic - they act as entry points for water
- Water diffuses preferentially through these zones, creating channels
- The difference in ionic concentration between dentinal fluid (rich in calcium, phosphate ions) and the relatively ion-poor resin matrix creates an osmotic gradient pulling water into the resin
- This drives continued water movement even after initial setting
3. HOW WATER TREES FORM - STEP BY STEP
- Dentinal fluid seeps outward through dentinal tubules toward the resin-dentin interface during and after obturation/bonding
- Water molecules penetrate the incompletely polymerized or hydrophilic resin matrix at the hybrid layer
- Water accumulates at microscopic voids, creating discrete water droplets within the resin
- Over time, adjacent droplets connect → form continuous water-filled channels
- Channels branch outward through the resin layer → branching "tree" pattern visible on TEM
- Channels pass from the hybrid layer → through the adhesive/sealer → to the outer surface
- These channels become pathways for hydrolysis, monomer leaching, enzyme activity (MMPs), and bacterial microleakage
4. CONSEQUENCES IN ENDODONTICS
A. Resin Sealer Degradation
- Water trees within resin-based root canal sealers (EndoREZ, RealSeal/Epiphany) cause:
- Hydrolysis of ester bonds in the resin polymer network → loss of mechanical strength
- Leaching of unpolymerized monomers out of the sealer into periapical tissues (cytotoxic)
- Progressive loss of sealer-dentin bond strength over time
- Increased microleakage along the root canal wall-sealer interface
B. Failure of the "Monoblock" Concept
- Resin-based sealers (with resin-coated GP or Resilon cores) were designed to form a "monoblock" - a single bonded mass of core + sealer + dentin with no interfaces
- Water treeing disrupts this monoblock by creating channels within the sealer layer
- The continuous tubular fluid flow prevents stable bonding → monoblock concept has not been achieved clinically with current materials
C. Nanoleakage
- Water trees are closely related to nanoleakage - fluid seepage through the hybrid layer at the nanometer scale
- Even when conventional dye tests show no leakage, silver nitrate reveals nanoleakage channels corresponding to water trees
- In endodontics: nanoleakage at the sealer-dentin interface allows bacterial byproducts to reach periapical tissues even through apparently "sealed" root fillings
D. Activation of Dentinal MMPs
- Water-filled channels activate endogenous Matrix Metalloproteinases (MMPs) in dentin
- MMPs (especially MMP-2, MMP-9) hydrolyze the unprotected collagen fibrils of the hybrid layer
- This destroys the structural foundation of the resin-dentin bond → progressive bond failure
- The process explains why resin sealer bond strength decreases significantly after 6-12 months of water storage
E. Secondary Infection Risk
- Water tree channels provide a microleakage pathway for oral bacteria, salivary proteins, and bacterial endotoxins
- In root canal treatment: coronal microleakage through water tree channels in the sealer → re-infection of the periapical region → endodontic treatment failure
5. WHICH MATERIALS ARE MOST AFFECTED?
| Material | Water Tree Susceptibility | Reason |
|---|---|---|
| All-in-one self-etch adhesives | Very high | Highly hydrophilic, acidic; attract water strongly |
| Methacrylate-based sealers (EndoREZ, Epiphany) | High | UDMA/TEGDMA monomers are hydrophilic |
| Two-step self-etch adhesives | Moderate | Separate primer reduces hydrophilicity of adhesive |
| Epoxy resin sealers (AH Plus) | Low-moderate | Less hydrophilic; more stable polymer network |
| Calcium silicate/bioceramic sealers (TotalFill BC, BioRoot RCS) | Very low | Hydrophilic but inorganic - no polymer network to form water trees; uses moisture to set rather than being degraded by it |
| ZOE sealers | Moderate | Eugenol leaches; solubility over time but not classic water treeing |
- Bioceramic sealers represent the solution to water treeing - their mineral setting reaction is not affected by dentinal fluid; they do not form polymer-based water trees
6. WATER TREE EFFECT IN BONDING AGENTS (Conservative Dentistry Context)
- In composite restorations placed with all-in-one (single-bottle) self-etch adhesives:
- Water trees form from the hybrid layer through the adhesive film
- Lead to secondary caries at the resin-tooth interface
- Cause progressive bond strength degradation over 6-24 months in vivo
- Solutions developed:
- AMIDE-modified monomers (e.g., in CLEARFIL Universal Bond Quick) - more hydrolytically stable; resist water tree formation
- Two-step self-etch systems - separate primer reduces water permeation
- MDP monomer (10-MDP) - stable ionic bond to hydroxyapatite; resists water degradation
- Glutaraldehyde-containing primers - crosslinks collagen, inhibits MMPs, reduces water uptake
7. DETECTION METHODS
| Method | Principle | What It Shows |
|---|---|---|
| Silver nitrate immersion + TEM | Ag⁺ fills water channels → reduced to Ag⁰ (black) | Gold standard; reveals water tree pattern clearly |
| Confocal Laser Scanning Microscopy (CLSM) | Fluorescent tracer penetration | Sealer/adhesive penetration depth and gaps |
| Micro-CT / Nano-CT | 3D imaging of void spaces | Volumetric analysis of channels and voids |
| SEM (Scanning Electron Microscopy) | Surface/cross-section morphology | Gap formation at resin-dentin interface |
| Dye penetration tests | Colored dye diffusion | Gross leakage; less sensitive than silver nitrate |
8. CLINICAL IMPLICATIONS & PREVENTION
For Root Canal Treatment (Endodontics)
- Prefer bioceramic sealers (TotalFill BC, BioRoot RCS) over methacrylate-based sealers - no polymer water tree formation; bioactive
- Remove smear layer completely (NaOCl + EDTA) before sealer placement - improves tubular seal, reduces outward fluid flow
- Dry canal adequately before obturation - paper points + ethanol rinse reduces free water at the interface
- Avoid resin sealers in very wet canals - residual moisture accelerates water tree formation in methacrylate systems
- Tight coronal seal immediately after obturation - reduces incoming oral fluid that potentiates water treeing
For Composite Restorations (Conservative Dentistry)
- Avoid all-in-one self-etch adhesives in deep cavity preparations (close to pulp - more dentinal fluid)
- Use two-step self-etch or selective etch protocols to minimize hydrophilic layer permeability
- Use MDP-containing universal adhesives with proven hydrolytic stability
- Apply MMP inhibitors (chlorhexidine 0.1-2%, EGCG, GMD) to dentin before bonding to inhibit collagen degradation through water tree channels
9. SUMMARY TABLE
| Aspect | Detail |
|---|---|
| Term coined by | Tay & Pashley (2003) |
| Location | Within polymerized resin adhesive/sealer layer |
| Driven by | Dentinal tubular fluid (outward flow), hydrophilic monomers, osmosis |
| Appearance | Branching tree-like water-filled channels (TEM) |
| Detection | Silver nitrate immersion → black deposits on TEM |
| Effect | Hydrolysis, MMP activation, bond failure, nanoleakage, microleakage |
| Most affected | All-in-one adhesives, methacrylate sealers |
| Least affected | Bioceramic sealers, 2-step self-etch adhesives, MDP-based systems |
| Prevention | Bioceramic sealers, MDP monomers, AMIDE monomers, canal drying, MMP inhibitors |
KEY REFERENCES
- Tay FR, Pashley DH (2003) - "Water treeing - A potential mechanism for degradation of dentin adhesives." Am J Dent. 16(1):6-12 - Original description of the water tree concept
- Tay FR, Pashley DH (2005) - "Tubular occlusion prevents water-treeing in single-bottle self-etch adhesives." J Dent Res. [PMID 16183786]
- Pashley DH et al. - "The evolution of dentin bonding: from no-etch to total-etch to self-etch"
- Pocket Dentistry - "Resin Materials for Root Canal Obturation" - water tree context in endodontic sealers
POSTER SUMMARY (One-liner)
Water trees are branching water-filled microchannels that form within hydrophilic resin adhesives and sealers due to dentinal fluid ingress — causing hydrolytic degradation, bond failure, nanoleakage, and ultimately endodontic/restorative treatment failure.
explain about Nano-Robots that use specific motility mechanisms to penetrate upto thousands of depth into the miraculous anatomy of the dentinal tubules in detail and also about its varrious applications in endodontics and restorative dentistry in 1000 words pointwise
nanorobots dentinal tubules endodontics motility drug delivery
nanorobots dentinal tubules endodontics motility mechanisms applications 2024 2025 depth penetration
nanorobots microrobots endodontics dentistry magnetic helical antibacterial
Theranautilus IISc helical nanorobots dentinal tubules 2000 microns magnetic endodontics Dasgupta 2021 2024
nanorobots microrobots dentistry endodontics restorative applications review
https://pmc.ncbi.nlm.nih.gov/articles/PMC7613116
microrobotics endodontics iron oxide nanoparticles biofilm Enterococcus faecalis
https://www.drnoordmd.com/post/tiny-titans-of-the-tooth-the-…
Nano-Robots in Dentistry
Motility Mechanisms, Dentinal Tubule Penetration & Clinical Applications
1. INTRODUCTION - THE PROBLEM NANO-ROBOTS SOLVE
- Root canal treatment (RCT) has a worldwide failure rate exceeding 10% - primarily due to residual bacteria surviving deep in dentinal tubules
- Dentinal tubules are 1-4 µm in diameter and extend up to 2500 µm (2.5 mm) from the pulp space to the DEJ/CEJ
- Bacteria (E. faecalis, Streptococcus, Fusobacterium) can penetrate up to 1500 µm deep into these tubules
- Conventional irrigants (NaOCl), laser activation (SWEEPS/PIPS), and ultrasonic systems reach only 200-900 µm into tubules - leaving a critical 600-1300 µm dead zone unreachable by passive chemistry
- There is no blood supply to dentinal tubules - bacteria are completely shielded from the host's immune system within them
- Nano-robots offer a revolutionary solution: active, motorized penetration into the full depth of every tubule, carrying antibacterial payloads and performing treatments at the molecular level
- The concept traces to physicist Richard Feynman's 1959 lecture "There's Plenty of Room at the Bottom" - his vision of "tiny mechanical surgeons" that operate inside the body
2. WHAT ARE DENTAL NANO-ROBOTS?
- Nano-robots (nanobots) are nanoscale to microscale devices (typically 100 nm - 5 µm) designed to navigate biological environments and perform targeted therapeutic tasks
- In dentistry, they are specifically designed to:
- Enter and navigate the 3D labyrinth of dentinal tubules
- Carry, deliver, and activate antibacterial agents or drugs at precise locations
- Perform localized hyperthermia to destroy biofilms
- Deposit remineralizing minerals to seal tubules
- Facilitate pulp-dentin regeneration by delivering growth factors
- A 0.5 mL droplet can contain one billion nanobots (Bathla et al., 2024)
3. THE MIRACULOUS ANATOMY OF DENTINAL TUBULES
- Tubule dimensions:
- At pulpal opening: ~2.5 µm diameter
- At mid-dentin: ~1.8 µm
- Near CEJ/DEJ: ~0.9 µm (progressively narrows)
- Length: up to 2500 µm (2.5 mm)
- Density: 20,000-45,000 tubules per mm² at the pulp surface
- Microtubular network: Each main tubule has lateral branches and canaliculi - creating a 3D interconnected network
- Total tubule surface area: Estimated several square meters per tooth
- Odontoblastic processes: Run within tubules; fluid-filled; support bacterial survival
- This complex geometry makes passive chemical penetration essentially impossible beyond 200-500 µm - the reason nano-robots represent a paradigm shift
4. TYPES OF DENTAL NANO-ROBOTS
A. Helical Nanopellers (Flagella-Inspired) - Most Advanced
- Developed by Indian Institute of Science (IISc), Bengaluru + Theranautilus startup (Dasgupta et al., 2021-2024)
- Shape: Corkscrew/helix - inspired by bacterial flagella
- Material: Silicon dioxide (SiO₂) core with iron oxide (Fe₃O₄) magnetic coating
- Size: ~300 nm diameter × ~2 µm length - dimensioned to fit dentinal tubules
- Motility: Rotating external magnetic field causes the helical bot to "screw" itself through fluid - like a corkscrew opening wine
- Penetration depth achieved: 2000 µm (2 mm) - the full depth of dentinal tubules (Dasgupta et al., Advanced Healthcare Materials, 2022)
- Speed: Up to 100x faster than passive chemical diffusion (Dasgupta et al., 2021)
- Key publication: Dasgupta et al. (2022), Adv Healthc Mater. PMID linked - "Mobile Nanobots for Prevention of Root Canal Treatment Failure"
B. Iron Oxide Nanoparticle Swarms (Aggregated Microswarms)
- Material: Iron oxide nanoparticles (IONPs) that self-assemble into collective swarms
- Behavior: Act like a "liquid robot" - dynamically reconfigure their shape to fit any irregular geometry (isthmuses, lateral canals, ramifications)
- Motility: Oscillating or rotating magnetic fields drive collective swarm movement
- Advantage: Unlike rigid robots, swarms can split, merge, and reform to access complex anatomy
- Described by Babeer et al. (2022) - Int Endod J perspective on microrobotics in endodontics
C. CalBots - Bioceramic Nano-Robots (2025 - Latest)
- Developed by IISc + Theranautilus (Peddi et al., 2025 - Advanced Science)
- Purpose: Specifically designed for dentinal hypersensitivity - sealing exposed dentinal tubules
- Material: Novel bioceramic cement formulation within magnetic nanobot framework
- Action: Navigate deep into tubules → deposit durable bioceramic mineral plugs → permanent seal
- Result: Lasting relief from dentinal hypersensitivity in a single application - outperforming repeated toothpaste use
- Unique feature: Regenerative material - promotes dentinal remineralization at the tubule base
D. Multi-Metallic Nanorods
- Developed by Hong Kong Baptist University (HKBU) team (Leung Cham-fai et al., 2025)
- Material: Silver + gold nanorods
- Navigation: Magnetic field-guided
- Efficacy: 99.99% antibacterial activity demonstrated
- Combined photocatalytic and magnetic properties
E. Light/Enzyme-Driven Nano-Robots
- TiO₂/Ag light-driven nanorobots - activated by specific wavelengths to generate ROS for antibacterial action
- Enzyme-powered biohybrid robots - use glucose oxidase/catalase reactions to self-propel using the body's own biochemistry
- Future direction: glucose-driven ultra-small nanorobots for stem cell-assisted pulp regeneration
5. MOTILITY MECHANISMS IN DETAIL
| Mechanism | How It Works | Bot Type |
|---|---|---|
| Rotating magnetic field | External 3D magnetic manipulation platform rotates helical bot like a corkscrew | Helical nanopellers |
| Oscillating magnetic field | Rocking motion drives bots linearly along tubule length in any orientation | Helical + swarms |
| Magnetic swarm locomotion | Collective behavior of IONPs - swarm reshapes to access complex geometry | Aggregated microswarms |
| Light-driven (photocatalytic) | Light energy activates TiO₂ layer → generates propulsive force + ROS | TiO₂/Ag nanorods |
| Chemically-driven (enzyme) | Glucose + enzyme catalysis → oxygen bubbles → self-propulsion | Biohybrid bots |
| Acoustic actuation | Ultrasound waves drive bot propulsion in high-viscosity environments | Emerging systems |
- Key innovation in IISc system: By using oscillating rather than only rotating magnetic fields, nanobots achieve isotropic (uniform, 360°) distribution throughout the entire dentine cross-section - regardless of tubule orientation, ensuring every tubule is reached simultaneously
6. APPLICATIONS IN ENDODONTICS
A. Deep Tubule Disinfection (Primary Application)
- Deliver NaOCl, chlorhexidine, or antibacterial nanoparticles to full 2000 µm tubule depth
- Target and destroy Enterococcus faecalis biofilms - the #1 cause of RCT failure
- 100x faster penetration than passive irrigation; eliminates the bacteria-harboring "dead zone"
B. Magnetic Hyperthermia - Localized Heat Killing
- Adjusting the frequency of the oscillating magnetic field causes the iron oxide coating to generate localized heat (42-45°C) - enough to destroy bacteria while sparing surrounding vital tissue
- Destroys E. faecalis within 15 minutes without systemic antibiotics
- Eliminates risk of antibiotic resistance - purely physical killing mechanism
C. Intracanal Drug Delivery
- Nanobots act as "micro-submarines" carrying drugs (antibiotics, calcium hydroxide, triple antibiotic paste) to exact locations
- Controlled, stimuli-responsive release - drug released only when pH drops (detecting active infection) or when specific bacterial enzymes are detected
- Eliminates need for repeated appointments for medicament changes
D. Removal of Intracanal Medicaments
- Bots navigate and mechanically dislodge and retrieve residual TAP/DAP from lateral canals and tubules before obturation - a current clinical challenge
E. Retreatment - Sealer & GP Removal
- Nano/microrobots can navigate around existing root filling materials, delivering solvents or applying mechanical force to disrupt failed obturations in retreatment cases
F. AI + CBCT-Guided Navigation ("Digital Twin")
- Cone Beam CT (CBCT) creates a 3D "digital twin" of the patient's root canal anatomy
- AI (convolutional neural networks) maps nanobot trajectories before injection
- CNNs identify complex canal configurations (C-shaped, calcified canals) with >90% accuracy to guide bots
- Bots follow the pre-planned route, ensuring complete coverage (Abozaid et al., 2025)
7. APPLICATIONS IN RESTORATIVE DENTISTRY
A. Dentinal Hypersensitivity Treatment (CalBots - 2025)
- Magnetic CalBots navigate to the full depth of exposed/open dentinal tubules
- Deposit bioceramic mineral plugs that permanently seal the tubule - blocking the hydrodynamic transmission responsible for pain
- Single application gives durable relief - vs. repeated toothpaste applications
- Regenerative - promotes secondary dentin formation at the sealed site
B. Dentin Remineralization & Caries Arrest
- Nanobots deliver nano-hydroxyapatite, calcium phosphate, or fluoride ions into early carious dentin tubules
- Mineral deposits progressively reharden demineralized dentin from within
- Potential to arrest early caries without cavity preparation
C. Targeted Adhesive Primer Delivery
- Deliver adhesive monomers (MDP, HEMA) into the base of dentinal tubules to create deeper hybrid layers with superior bond strength
- Eliminates the effect of outward tubular fluid (overcomes the water tree problem)
D. Pulp-Dentin Regeneration
- Act as carriers for growth factors (BMP-2, TGF-β, FGF), stem cells (DPSC, SCAP), or scaffolding proteins delivered precisely to the apical papilla or pulp chamber
- Enable targeted regenerative endodontic procedures (REP) without open surgery
- Stimuli-responsive hydrogel scaffolds carried by nanobots release their cargo only in the presence of infection-specific pH or enzymes
E. Anti-Caries Prophylaxis
- Nanobots loaded with fluoride, silver diamine fluoride (SDF), or antimicrobial peptides can be directed into early demineralized zones
- Preventive dentistry application - treatment before the cavity forms
8. ADVANTAGES OVER CONVENTIONAL METHODS
| Feature | Conventional Irrigation | Nano-Robots |
|---|---|---|
| Penetration depth | 200-900 µm | 2000 µm (full depth) |
| Speed | Passive diffusion | 100x faster |
| Access to lateral canals | Poor | Superior |
| Antibacterial mechanism | Chemical only | Chemical + hyperthermia + mechanical |
| Drug delivery precision | Bulk/flooding | Targeted, site-specific |
| Antibiotic resistance risk | Yes (antibiotics) | Eliminated (physical killing) |
| Retreatability | Standard | Magnetically retrievable |
| Tissue damage risk | NaOCl accidents | Minimal - localized action |
9. LIMITATIONS & CHALLENGES
- Not yet in routine clinical use - most evidence is in vitro; human trials in early phases (Theranautilus targeting 2025-2026 clinical launch)
- Cost - specialized laser/magnetic manipulation platforms and nanobot synthesis are expensive
- Regulatory approval - FDA/CE marking pathways for active medical nanodevices are still being established
- Retrieval - complete retrieval of all nanobots after use must be ensured; residual bots are a safety concern (current solution: magnetic retrieval using external fields)
- Tubule narrowing - at 0.9 µm near CEJ, even the smallest bots may not penetrate the most apical portions
- Toxicity profile - long-term biocompatibility of iron oxide, silica, silver nanorods must be further established in vivo
- Scalability - manufacturing billions of precision nanobots cost-effectively remains a challenge
10. FUTURE PERSPECTIVES
- Theranautilus (IISc spin-off): Developing chair-side injection device for dentists; commercial launch projected 2026
- AI + nanobot integration - real-time AI-guided navigation based on CBCT digital twins
- Swarm intelligence - bots communicate with each other to collectively optimize canal coverage
- Biodegradable nanobots - self-dissolving bots that leave only the drug payload behind
- Theranostic nanobots - simultaneously diagnose (detect bacteria, measure pH) and treat in one pass
- 3D-printed nanorobots - personalized geometry matching specific canal anatomy via AI-designed templates
- Dr. Robert Freitas' vision of "Dentifrobots" - autonomous nanorobots patrolling the oral cavity continuously, destroying pathogenic bacteria before symptoms develop
KEY REFERENCES
| Reference | Contribution |
|---|---|
| Dasgupta D et al. (2022). Adv Healthc Mater. PMID: 35443216 | Helical nanobots - 2000 µm penetration, first live tubule demonstration |
| Babeer A et al. (2024). Int Endod J. | Microrobotics in endodontics - comprehensive perspective |
| Peddi S et al. (2025). Advanced Science | CalBots for dentinal hypersensitivity |
| Leung Cham-fai et al. (2025). HKBU | Multi-metallic nanorods, 99.99% antibacterial |
| Bathla et al. (2024) | Deep penetration comparison - nanobots vs. SWEEPS/PIPS |
| Freitas RA Jr. (2000). J Am Dent Assoc. | Conceptual foundation of dental nanorobotics ("Dentifrobots") |
Create a detailed cross-section diagram of a helical nanorobot navigating inside a dentinal tubule
A highly detailed, scientifically accurate cross-section diagram for a dental/medical poster showing a helical nanorobot navigating inside a dentinal tubule. The diagram should be split into two panels: LEFT PANEL - "Macro View: Tooth Cross-Section" Show a vertical cut-through of a tooth root showing: Enamel at top, Dentin layer (beige/cream color, making up the bulk), Pulp chamber (pink, center), Root canal space. Multiple dentinal tubules shown as tiny parallel channels running from the pulp outward through the dentin like radial spokes. Label: "Dentinal Tubules (20,000-45,000/mm²)". Show bacteria (small red dots labeled "E. faecalis") clustered deep inside tubules far from the canal. Show a gradient bar on the right side: "0 µm (Pulp opening 2.5µm diameter)" to "2500 µm (Near CEJ 0.9µm diameter)". Arrow showing direction of bacterial penetration depth: 1500 µm max for bacteria. RIGHT PANEL - "Magnified Tubule Cross-Section" (main focus, larger) Show a single dentinal tubule in dramatic close-up longitudinal cross-section: - Tubule walls: textured cream/ivory dentin walls with peritubular dentin (darker ring lining) - Dentinal fluid: light blue transparent fluid filling the tubule lumen - Odontoblastic process: thin pink thread running through the center - HELICAL NANOROBOT: A prominent corkscrew/helix-shaped robot in metallic silver/grey with a teal-blue iron oxide magnetic coating visible as patches. Size labeled "~300nm diameter × 2µm length". The helix is actively screwing through the tubule fluid, shown with small rotation arrows around it. - Bacterial colony: Red/orange biofilm cluster of oval bacteria (E. faecalis) further ahead in the tubule - Antibacterial payload: Small golden dots releasing from the nanobot surface labeled "Antibacterial payload release" - Heat waves: Orange wavy lines emanating from the nanobot surface labeled "Localized hyperthermia (42-45°C)" - External rotating magnetic field: Curved magnetic field lines shown in purple/blue outside the tubule labeled "Rotating external magnetic field (30 Gauss, 5Hz)" - Depth markers on the right side: 0µm, 500µm, 1000µm, 1500µm (bacteria limit), 2000µm (nanobot reaches here - highlighted with star/checkmark) BOTTOM BAR - Comparison strip: Three columns labeled: "Conventional Irrigation" - blue arrow stopping at 200-900µm "SWEEPS/PIPS Laser" - teal arrow stopping at 900µm "Helical Nanobot ✓" - gold arrow reaching full 2000µm with checkmark Title at top: "Helical Nanorobot Navigation in Dentinal Tubules" Subtitle: "IISc + Theranautilus Technology | Dasgupta et al., 2022" Color scheme: Dark navy background for the diagram area, cream/ivory for dentin tissue, metallic silver for nanobot, purple/teal for magnetic field, red for bacteria. Clean academic poster style, high resolution, labeled clearly.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
compress the matter in 250 words for my poster
Nano-Robots in Endodontics & Restorative Dentistry
The Problem
What Are Dental Nano-Robots?
Types & Motility Mechanisms
- Helical Nanopellers (IISc + Theranautilus): Corkscrew-shaped SiO₂ bots with iron oxide coating; rotating magnetic field screws them through tubule fluid → 2000 µm penetration (100x faster than conventional methods)
- IONP Microswarms: Iron oxide nanoparticle collectives; reshape dynamically to access isthmuses and lateral canals
- CalBots (2025): Bioceramic-loaded nanobots seal tubules permanently for hypersensitivity relief in one application
- Multi-metallic Nanorods (HKBU, 2025): Silver-gold nanorods; 99.99% antibacterial efficacy
Applications
| Endodontics | Restorative Dentistry |
|---|---|
| Deep tubule disinfection (full 2000 µm) | Dentinal hypersensitivity (CalBots) |
| Magnetic hyperthermia (42-45°C) kills E. faecalis in 15 min | Dentin remineralization & caries arrest |
| Targeted drug/medicament delivery | Deeper adhesive hybrid layer formation |
| Biofilm destruction without antibiotics | Pulp-dentin regeneration (growth factor delivery) |
| AI + CBCT "digital twin" guided navigation | Preventive anti-caries prophylaxis |
Future
"A single 0.5 mL drop holds one billion nanobots" - Bathla et al., 2024