answer the following question all according to bds 3rd year(india general surgery
- Surgical anatomy
- Wounds and wound healing
- Infections and abscesses
- Cysts and tumors relevant to oral/maxillofacial region
- Fluid and electrolyte balance
- Shock
- Pre/post-operative care
- Common surgical conditions
Write short note on thyroid storm/crisis.
Thyroid Storm (Thyrotoxic Crisis)
Definition
Aetiology / Precipitating Factors
| Category | Examples |
|---|---|
| Systemic insult | Infection, trauma, general surgery |
| Thyroid surgery | Manipulation of thyroid in non-euthyroid patients |
| Drug/hormone related | Withdrawal of antithyroid drugs, iodine administration, ingestion of thyroid hormone |
| Cardiovascular | Myocardial infarction, pulmonary embolism, CVA |
| Obstetric | Labour and delivery, eclampsia |
| Endocrine | Diabetic ketoacidosis, hyperosmolar coma |
| Radioactive iodine therapy | Can trigger storm |
| Unknown | Up to 25% of cases have no identifiable cause |
Pathophysiology
- Adrenergic hyperactivity - either from increased release of thyroid hormones or increased receptor sensitivity
- Higher free thyroid hormone levels - precipitants such as infection or stress free T3/T4 from binding proteins, raising free hormone concentration
- Excess T3/T4 enter cells, T4 is converted to active T3, which binds nuclear thyroid hormone receptors and drives hypermetabolic gene transcription
- Negative feedback suppression of TSH at the pituitary
Clinical Features
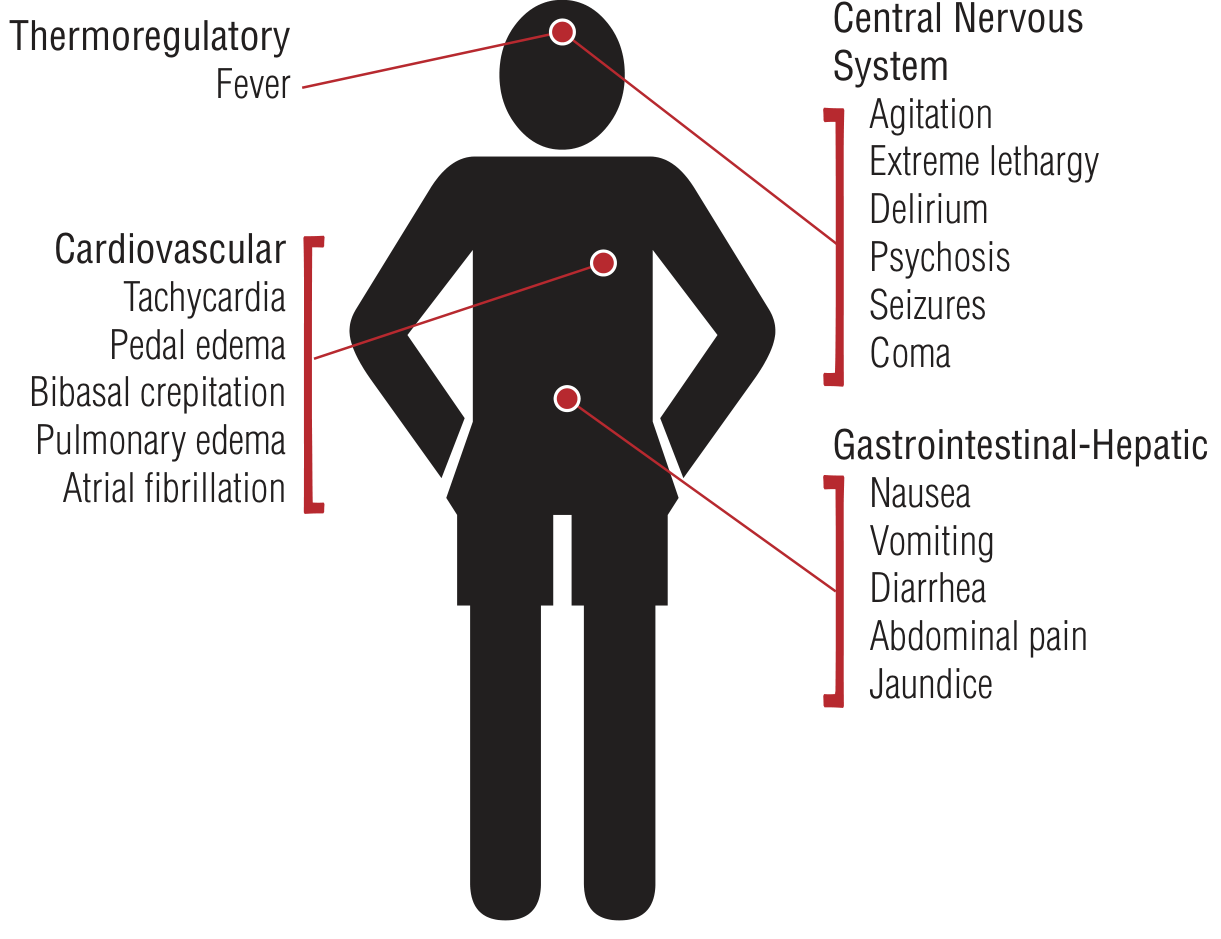
1. Thermoregulatory
- High fever - marked pyrexia 104-106°F (40-41°C), a hallmark feature
2. Cardiovascular
- Extreme tachycardia (often disproportionate to fever) - >140 bpm
- Atrial fibrillation
- Pedal oedema, bibasal crepitations
- Pulmonary oedema, congestive cardiac failure
- Hypotension (from volume depletion or low vascular resistance)
3. Central Nervous System
- Agitation, restlessness, tremor
- Delirium, psychosis
- Seizures, coma
4. Gastrointestinal-Hepatic
- Nausea, vomiting, diarrhoea
- Abdominal pain
- Jaundice (hepatic failure - poor prognosis)
Diagnosis
| Parameter | Score |
|---|---|
| Fever ≥104°F | 30 |
| Tachycardia ≥140 bpm | 25 |
| CNS - Coma | 30 |
| CNS - Seizure | 20 |
| CNS - Mild agitation | 10 |
| GI/hepatic dysfunction | 10-20 |
| Precipitant present | 10 |
| AF | 10 |
- Score ≥45 = Thyroid storm (likely)
- Score 25-44 = Impending storm
- Score <25 = Unlikely thyroid storm
- Low/undetectable TSH
- Elevated free T3 and T4
- LFTs may be deranged
Differential Diagnosis
- Heatstroke, neuroleptic malignant syndrome, serotonin syndrome
- Sympathomimetic intoxication, anticholinergic crisis
- Meningitis, sepsis
- Manic episode, panic attack
Treatment
Critical rule: Iodine must ALWAYS be given at least 1 hour AFTER antithyroid drugs (thionamides), as iodine given first can worsen the storm.
Order of Administration:
A. Supportive Treatment
- Cooling - tepid sponging, cooling blankets
- Antipyretics - Paracetamol (acetaminophen); avoid Aspirin (displaces T3/T4 from protein binding, worsens free hormone levels)
- IV fluids - dextrose-containing solutions (glycogen stores depleted)
- Benzodiazepines - for agitation
- Electrolyte replacement
- ICU monitoring
B. Symptomatic Treatment - Beta Blockers
- Propranolol (drug of choice) - blocks adrenergic effects AND blocks peripheral conversion of T4 to T3
- Also reduces tremor, hyperpyrexia, restlessness, emotional lability
- If beta blockers are contraindicated (asthma/COPD) - use Esmolol (short-acting, β1-selective) or Metoprolol
- Alternative: Reserpine 2.5-5 mg IM every 4 hours
C. Thyroid-Directed Treatment (Three Goals)
| Goal | Drug |
|---|---|
| Block thyroid hormone synthesis | PTU 500-1000 mg loading, then 250 mg 4-hourly OR Methimazole |
| Prevent thyroid hormone release | Lugol's iodine / SSKI - given ≥1 hour AFTER PTU |
| Block peripheral conversion of T4 to T3 | PTU (preferred over methimazole), Propranolol, Corticosteroids |
- PTU is preferred over methimazole in crisis because it additionally blocks T4-to-T3 conversion
- Corticosteroids (Hydrocortisone IV / Dexamethasone) - block T4 to T3 conversion, treat possible adrenal insufficiency
D. Treat the Precipitating Cause
- Antibiotics for infection
- Management of MI, DKA, etc.
E. Definitive Treatment (after stabilization)
- Radioactive iodine (RAI) therapy
- Total thyroidectomy
Prognosis
- Untreated: mortality ~100%
- With prompt treatment: mortality 10-30%
- Death occurs from: multiorgan failure, congestive heart failure, arrhythmias, DIC, hypoxic brain damage, or sepsis
- With PTU + iodine + beta blockers + corticosteroids + fluid resuscitation, acute thyroid storm can resolve within 24 hours
Write short note on solitary thyroid nodule.
Solitary Thyroid Nodule
Definition
- About 70% of discrete thyroid swellings are clinically isolated; 30% are dominant
- Autopsy studies suggest up to 50% of individuals may have thyroid nodules
- Clinically palpable nodules occur in approximately 4% of the population
- The incidence increases with age
Pathological Types (What It Can Be)
| Type | Frequency |
|---|---|
| Non-neoplastic (colloid cyst, thyroiditis, areas of colloid degeneration) | Most common |
| Follicular adenoma (benign) | 30-40% of isolated swellings |
| Malignant (thyroid carcinoma) | ~15% of isolated swellings; ~7% of dominant swellings |
Key fact: Benign neoplasms outnumber thyroid carcinomas by approximately 10:1. However, the solitary nodule carries a higher risk of malignancy than a multinodular goiter.
Features Suggesting Malignancy
History
- Age: Children (<20 yrs) have 20-50% malignancy risk; also higher in males
- History of head/neck radiation - 40% chance of malignancy; risk peaks 20-30 years post-exposure
- Family history of thyroid cancer or associated syndromes (MEN2, Cowden's, Gardner's)
- Rapid growth, hoarseness (suggests recurrent laryngeal nerve involvement - ominous sign)
- Dysphagia, dyspnoea, choking
Examination - Features Suspicious for Malignancy
- Hard, firm, non-tender, fixed nodule
- Cervical lymphadenopathy
- Vocal cord palsy (hoarseness)
- Horner's syndrome
Features Suggesting Benignity
- Soft, smooth, well-defined, mobile
- Tender nodule (suggests thyroiditis or haemorrhage into cyst)
- Toxic nodule (hot on scan - nearly always benign)
- Female sex, older age
Investigation
1. Thyroid Function Tests (TFTs)
- Serum TSH and T3/T4
- Hyperthyroidism with a nodule = toxic adenoma; indicates need for isotope scan
2. Autoantibody Titres
- To detect chronic lymphocytic (Hashimoto's) thyroiditis
- Positive antibodies increase risk of thyroid failure after lobectomy
3. Ultrasonography (USG) - First-line imaging
- Hypoechoic echotexture
- Irregular / ill-defined borders
- Microcalcifications (psammoma bodies - papillary Ca)
- Taller-than-wide shape
- Absent halo
- Internal vascularity on Doppler
- Cystic or spongiform nodule
- Well-defined halo
- Coarse calcification
4. Isotope Scan (Radionuclide - 99mTc / 131I)
- Now largely abandoned except when toxicity is associated with nodularity
- "Hot" nodule = takes up radioiodine avidly → nearly always benign (toxic adenoma)
- "Cold" nodule = no uptake → higher risk of malignancy (~15-20%), but most cold nodules are still benign
- "Warm" nodule = equal uptake → similar to normal tissue
5. Fine Needle Aspiration Cytology (FNAC) - Investigation of Choice / Gold Standard
- Most reliable, minimally invasive, cost-effective
- A 23-gauge needle is used; ultrasound guidance recommended for impalpable, cystic, or recurrent nodules
- Requires at least 6 follicular clusters, each with 10-15 cells, from 2 aspirates for adequacy
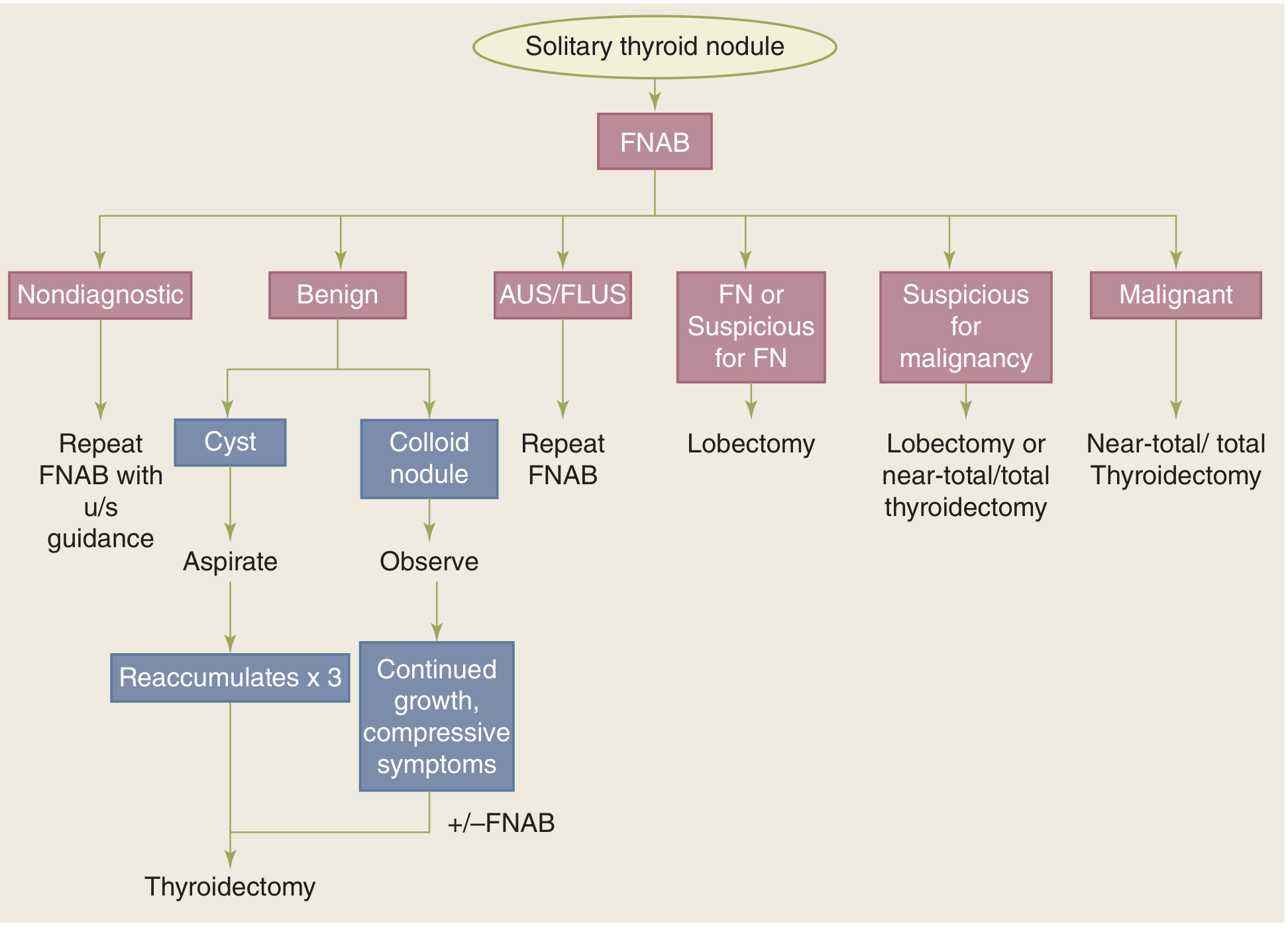
Bethesda Classification of FNAC Results
| Bethesda Category | Risk of Malignancy | Action |
|---|---|---|
| I - Non-diagnostic / Unsatisfactory | 1-4% | Repeat FNAC with US guidance |
| II - Benign | <3% | Observe (if cyst - aspirate; if recurs x3 - thyroidectomy) |
| III - AUS / FLUS | 5-15% | Repeat FNAC or molecular testing |
| IV - Follicular Neoplasm (FN) | 15-35% | Lobectomy |
| V - Suspicious for Malignancy | 60-75% | Lobectomy or near-total/total thyroidectomy |
| VI - Malignant | 97-99% | Near-total / Total thyroidectomy |
Management Flowchart
Treatment
Conservative / Observation
- Benign colloid nodules on FNAC → observe with periodic USG and FNAC
- TSH suppression therapy with thyroxine (controversial; less commonly used now)
Surgical
- Thyroid lobectomy (hemithyroidectomy) - for follicular neoplasm on FNAC, where frozen section at surgery guides further resection
- Near-total / Total thyroidectomy - for malignant or suspicious FNAC, bilateral disease, large nodules, radiation history, familial thyroid cancer
- Aspiration - for cystic nodules; if fluid reaccumulates 3 times, proceed to thyroidectomy
Radioactive Iodine (RAI)
- For toxic (hot) autonomous nodules causing hyperthyroidism
Key Surgical Points (Exam-Important)
- FNAC is the investigation of choice for all solitary thyroid nodules
- A cold nodule on isotope scan has ~15-20% risk of malignancy - NOT diagnostic by itself
- Frozen section during lobectomy helps guide further resection
- Complications of thyroid surgery: RLN injury (hoarseness), hypoparathyroidism (hypocalcaemia), haemorrhage
- Papillary carcinoma is the most common thyroid malignancy following radiation exposure
Write short note on tetany.
Tetany
Definition
Tetany is defined physiologically as repetitive electrical discharges of motor neurons after a single stimulus, producing sustained muscle spasm.
Aetiology
A. Hypocalcaemia (Most Common Cause)
| Category | Causes |
|---|---|
| Post-surgical (commonest surgical cause) | After thyroidectomy, parathyroidectomy, radical neck dissection; "Hungry bone syndrome" post-parathyroidectomy |
| Hypoparathyroidism | Autoimmune, infiltration (granuloma, metastases), radiation-induced, HIV |
| Vitamin D deficiency | Rickets, malabsorption, lack of sunlight |
| Renal failure | Deficiency of 1,25-dihydroxyvitamin D + hyperphosphataemia |
| Acute pancreatitis | Ca²⁺ precipitation in peripancreatic fat necrosis (saponification) |
| Malabsorption | Small bowel fistula, loss of calcium-rich effluent |
| Massive blood transfusion | Citrate (preservative) binds ionized Ca²⁺ |
| Hypomagnesaemia | Impairs PTH secretion and action |
| Drugs | Bisphosphonates, calcitonin, phenytoin, foscarnet |
B. Alkalosis (Without Hypocalcaemia)
- Hyperventilation tetany - the most common cause of tetany in clinical practice without true hypocalcaemia
- Alkalosis decreases ionized Ca²⁺ by increasing protein binding of calcium
- Seen in anxiety, hysteria, mechanical over-ventilation
- Note: Tetany is rarely seen in renal failure despite low calcium - due to protective effect of concurrent metabolic acidosis
C. Hypomagnesaemia
- Magnesium deficiency independently causes tetany and also impairs PTH release
Pathophysiology
- Normal serum calcium: 8.5-10.5 mg/dL; ionized calcium: 4.5-5.6 mg/dL
- Tetany typically occurs when:
- Ionized calcium falls below 4.3 mg/dL
- OR total serum calcium falls below 7.0 mg/dL
- Calcium stabilizes the neuronal membrane by blocking sodium channels. When calcium falls:
- Threshold for nerve firing is lowered
- Spontaneous depolarization of peripheral motor nerves occurs
- This leads to sustained, repetitive muscle contractions (spasm/tetany)
- Alkalosis worsens this by increasing calcium binding to albumin, further reducing the ionized fraction
Types of Tetany
| Type | Description |
|---|---|
| Latent tetany | No spontaneous spasms; detected only by clinical signs (Chvostek, Trousseau) |
| Manifest (overt) tetany | Spontaneous spasms, carpopedal spasm, laryngospasm |
Clinical Features
Symptoms (in order of increasing severity)
- Paraesthesias - earliest symptom; circumoral (perioral) numbness, tingling of fingers and toes (acral)
- Muscle cramps - painful cramps, especially in hands and feet
- Carpopedal spasm - characteristic posture of the hand (see below)
- Laryngospasm - stridor, respiratory difficulty (life-threatening)
- Seizures / convulsions
- Cardiac arrhythmia - prolonged QT interval, bradycardia, cardiac arrest
Classic Signs
1. Trousseau's Sign (More Specific - ~94% sensitive)
- A blood pressure cuff is inflated above systolic pressure (20 mmHg above) on the arm and maintained for 3 minutes
- Positive: Development of carpopedal spasm - characteristic flexion at wrist and MCP joints, extension of IP joints, thumb adduction ("obstetrician's hand" / "main d'accoucheur")
- More reliable and specific than Chvostek's sign
2. Chvostek's Sign (Less Specific)
- Tap the facial nerve just anterior to the ear (at the parotid region, 2 cm anterior to the tragus)
- Positive: Twitching/contraction of ipsilateral facial muscles (angle of mouth, cheek, nose)
- Note: Positive Chvostek's sign is seen in up to 10% of normal individuals - hence less specific
3. Peroneal Sign (Lust's Sign)
- Tap the common peroneal nerve below the head of the fibula
- Positive: Dorsiflexion and eversion of the foot
4. Erb's Sign
- Increased electrical excitability of peripheral nerves (galvanic current <5 mA causes tetanic contractions)
Other Manifestations of Hypocalcaemia (Chronic)
- Ocular: Cataracts (calcification of the lens)
- CNS: Basal ganglia calcification, Parkinsonian-like movements, papilloedema, raised intracranial pressure
- Psychiatric: Anxiety, depression, confusion, psychosis
- Cardiovascular: Prolonged QT interval on ECG, heart failure
- Dental (important for BDS!): Dental hypoplasia, failure of eruption, defective enamel and root formation, abraded/carious teeth (when hypocalcaemia occurs during early development)
- Skin/Hair: Dry skin, brittle nails, alopecia
Investigations
| Investigation | Finding |
|---|---|
| Serum total calcium | <8.5 mg/dL (tetany at <7.0 mg/dL) |
| Serum ionized calcium | <4.3 mg/dL (critical threshold for tetany) |
| Serum albumin | Needed to correct calcium: corrected Ca = measured Ca + 0.8 × (4 - albumin) |
| Serum phosphate | High in hypoparathyroidism; low in Vit D deficiency |
| Serum PTH | Low/normal in hypoparathyroidism; elevated in Vit D deficiency, renal failure |
| Serum magnesium | Rule out hypomagnesaemia |
| Serum 25(OH) Vitamin D | To assess Vit D stores |
| ECG | Prolonged QT interval, ST segment prolongation |
| ABG (blood gas) | Alkalosis in hyperventilation tetany |
Treatment
1. Immediate / Emergency Treatment
- IV Calcium gluconate 10% - 10-20 mL (1-2 ampoules) slowly IV over 10 minutes
- Drug of choice due to lower risk of tissue toxicity compared to calcium chloride
- IV Calcium chloride 10% - faster acting (does not require hepatic metabolism); preferred in cardiac arrest
- For ongoing hypocalcaemia: IV calcium infusion (calcium gluconate in dextrose/saline)
Important: If hyperphosphataemia is present (>6.5 mg/dL), do NOT give calcium first - it increases the Ca×P product and causes ectopic calcification. Manage phosphate first.
Important: Correct hypomagnesaemia first before giving calcium, as hypocalcaemia is refractory to treatment in the presence of low magnesium.
2. For Hyperventilation Tetany
- Rebreathe into a paper bag - raises CO₂, corrects alkalosis, raises ionized Ca²⁺
- Reassurance, sedation if anxious
3. Chronic Management
- Oral calcium supplements - calcium carbonate or calcium citrate
- Vitamin D or active metabolite - 1,25(OH)₂D₃ (calcitriol) to increase intestinal calcium absorption
- Oral magnesium if hypomagnesaemia present
Tetany After Thyroid Surgery (Surgically Important)
- Occurs due to accidental removal or devascularization of parathyroid glands during thyroidectomy or parathyroidectomy
- Also occurs due to "hungry bone syndrome" - rapid uptake of calcium by bones post-parathyroidectomy
- Typically appears 24-72 hours after surgery
- Early sign: perioral tingling, positive Chvostek's sign
- Managed with IV calcium gluconate, followed by oral calcium + calcitriol
Key Points for Exam
- Tetany = neuromuscular hyperexcitability from ↓ ionized Ca²⁺
- Most common surgical cause = post-thyroidectomy hypoparathyroidism
- Trousseau's sign (more specific) - carpopedal spasm with BP cuff
- Chvostek's sign (less specific) - facial twitch with facial nerve tap
- Alkalosis causes tetany without true hypocalcaemia (hyperventilation)
- Chvostek positive in 10% normals - not diagnostic alone
- Correct Mg²⁺ deficiency before treating Ca²⁺ deficiency
- Never give calcium if severe hyperphosphataemia is present
- ECG shows prolonged QT interval
Describe clinical symptoms, signs and treatment of primary thyrotoxicosis.
Primary Thyrotoxicosis (Graves' Disease)
Definition
Primary vs Secondary thyrotoxicosis:
- Primary = Affects younger patients; brunt falls on the nervous system and eyes; associated with diffuse goitre and eye signs
- Secondary = Occurs in pre-existing nodular goitre in middle-aged/elderly; brunt falls on the cardiovascular system; eye signs absent
Aetiology / Risk Factors
- Young women (F:M = 7:1)
- Family history positive in 55% of patients (autoimmune endocrine diseases)
- Stress, pregnancy, iodine excess may trigger onset
- Genetic predisposition (HLA-DR3, HLA-B8)
Pathophysiology
- TSH-RAb (IgG antibodies) bind to and stimulate TSH receptors on thyroid follicular cells
- This leads to hyperplasia and hypertrophy of all functioning thyroid tissue
- Excess T3 and T4 → hypermetabolic state + sympathetic nervous system activation
- Histology: hyperplastic acini lined by tall columnar epithelium, empty or vacuolated colloid with characteristic "scalloped" pattern at the periphery
Clinical Symptoms
General / Metabolic
- Weight loss despite good (increased) appetite - most significant and characteristic symptom
- Heat intolerance and preference for cold climate
- Excessive sweating
- Fatigue and weakness
Nervous System (Dominant in Primary Thyrotoxicosis)
- Nervousness, irritability, emotional lability
- Insomnia
- Tremor of hands (fine tremor)
- Weakness of muscles (proximal myopathy)
- Poor concentration
Cardiovascular
- Palpitations (awareness of heartbeat)
- Tachycardia (including elevated sleeping pulse rate - key clinical indicator)
- Dyspnoea on exertion
- (Less pronounced than in secondary thyrotoxicosis)
Eye Symptoms (Specific to Graves' Disease / Primary Thyrotoxicosis)
- Staring or protruding eyes
- Diplopia (double vision) - due to ophthalmoplegia (extraocular muscle weakness)
- Difficulty closing eyelids
- Eye pain (if corneal ulceration develops)
- Watering, grittiness, irritation
Gastrointestinal
- Diarrhoea, nausea, vomiting
Reproductive
- Amenorrhoea / oligomenorrhoea in women
- Decreased libido
Clinical Signs
Five Cardinal Signs of Primary Thyrotoxicosis (S. Das)
1. Eye Signs (4 types - pathognomonic of Graves')
| Sign | How to Elicit | What it Means |
|---|---|---|
| Lid retraction | Upper lid higher than normal; sclera visible above/below iris | Overactivity of smooth muscle of levator palpebrae; sympathetic overactivity |
| Lid lag (von Graefe's sign) | Upper eyelid lags behind eyeball as patient looks downward | Exophthalmos; sympathetic overactivity |
| Stellwag's sign | Staring look + infrequent blinking + widening of palpebral fissure | Toxic contraction of striated fibers of levator |
| Joffroy's sign | Absence of forehead wrinkling when patient looks upward with face inclined downward | Exophthalmos |
| Exophthalmos (proptosis) | Eyeball pushed forward by retro-orbital fat/oedema/cellular infiltration; sclera visible below lower edge of iris (later above upper iris too) | Autoimmune retroorbital inflammation |
| Möbius sign | Inability to converge eyeballs | Weakness of convergence |
Note: Lid retraction and lid lag are not the same as exophthalmos. Exophthalmos = forward displacement of the eyeball itself.
2. Goitre
- Diffuse, smooth, uniformly enlarged thyroid (both lobes)
- Firm consistency
- Bruit (vascular murmur audible over the gland) - due to markedly increased vascularity - characteristic of Graves' disease
- Thrill may be palpable over the goitre
- Moves upward on deglutition (confirms thyroid origin)
3. Pulse
- Tachycardia - rapid, bounding pulse
- Sleeping pulse rate is the most reliable index:
- Mild thyrotoxicosis: sleeping pulse < 90 bpm
- Moderate: 90-110 bpm
- Severe: > 110 bpm
- May be irregular in severe cases (atrial fibrillation - more in secondary)
4. Skin
- Hot and moist (warm, sweaty) palms - characteristic of primary thyrotoxicosis
- Fine, soft, velvety skin
- Pretibial myxoedema (bilateral non-pitting oedema of shins - specific to Graves')
5. Tremor
- Fine tremor of outstretched hands - characteristic
- Hyperreflexia
Other Signs
- Hypertension (wide pulse pressure - raised systolic, low diastolic)
- Proximal muscle weakness
- Gynaecomastia in males
- Acropachy (clubbing + periosteal new bone formation - rare, specific to Graves')
- Onycholysis (nails separating from nail bed)
Investigations
| Investigation | Finding |
|---|---|
| Serum TSH | Suppressed / undetectable (first line, highest sensitivity) |
| Free T3, Free T4 | Elevated |
| TRAb (TSH receptor antibodies) | Elevated - diagnostic of Graves' disease |
| Radioactive iodine (123I) scan | Diffuse, uniform, elevated uptake throughout gland - confirms Graves' (vs focal uptake in toxic adenoma) |
| Thyroid USG + Doppler | Diffuse enlargement; increased vascularity |
| FNAC | Not usually needed unless co-existing nodule |
| ECG | Sinus tachycardia; occasionally atrial fibrillation |
| CBC, LFTs | Baseline before antithyroid drugs |
Treatment
A. Non-Specific / Symptomatic Treatment
- Rest - both physical and mental
- High caloric, high protein diet
- Sedatives - benzodiazepines for anxiety and insomnia
- Beta-blockers (Propranolol) - first line for symptomatic relief
- Controls tachycardia, palpitations, tremor, anxiety
- Also blocks peripheral conversion of T4 to T3
- Dose: 40-80 mg TDS; used until euthyroid state achieved
B. Medical Treatment (Antithyroid Drugs - ATDs)
1. Thionamides (Carbimazole / Methimazole / PTU)
| Drug | Mechanism | Dose |
|---|---|---|
| Carbimazole | Blocks oxidation and organification of iodine; inhibits thyroid hormone synthesis | 10-15 mg TDS initially; reduce to maintenance 5 mg OD-BD |
| Methimazole (active metabolite of carbimazole) | Same as carbimazole | Preferred over PTU (less hepatotoxicity) |
| PTU (Propylthiouracil) | Blocks synthesis + blocks peripheral T4→T3 conversion | Preferred in pregnancy (1st trimester) and thyroid storm |
- Duration: 12-18 months
- Remission rate: ~30-50% after stopping drugs
- Side effects: agranulocytosis (most serious - check WBC if fever/sore throat), rash, hepatotoxicity (PTU)
2. Iodine (Lugol's Iodine - 5% I₂ + 10% KI)
- Wolff-Chaikoff effect - high iodine load transiently suppresses thyroid hormone synthesis and release
- Reduces vascularity and size of gland (firm up the gland)
- Used pre-operatively for 10-14 days before thyroidectomy to reduce intraoperative bleeding
- NOT used for long-term medical treatment (escape phenomenon occurs after 2 weeks)
C. Radioactive Iodine (RAI - ¹³¹I) Therapy
- Mechanism: Concentrated in thyroid; beta radiation destroys thyroid cells
- Indications: Relapse after ATD, patients unfit for surgery, elderly patients, small goitre, patient preference
- Contraindications: Pregnancy, breastfeeding, active Graves' orbitopathy (worsens eye disease), suspected malignancy, children < 5 years
- Effect: Gradual reduction in thyroid size and function over 6-12 weeks
- Complication: Hypothyroidism (often intentional - ~80% become hypothyroid within 1 year, requiring lifelong thyroxine)
D. Surgical Treatment (Thyroidectomy)
- Large goitre causing compressive symptoms (dysphagia, stridor, tracheal compression)
- Suspected or confirmed co-existing thyroid malignancy
- Pregnancy or planning pregnancy within 6 months (relative)
- Failed medical therapy or relapse
- Patient preference
- Active Graves' orbitopathy (surgery preferred over RAI)
- Children and young patients with large goitres
- Render euthyroid with antithyroid drugs (carbimazole) for 6-8 weeks
- Beta-blockers to control pulse rate (pulse < 80 before surgery)
- Lugol's iodine for 10-14 days pre-op (firms the gland, reduces vascularity, reduces intraoperative bleeding)
- Near-total or total thyroidectomy - preferred for Graves' disease (lowest relapse rate)
- Subtotal thyroidectomy (leaving 4-8 g of tissue) - historically done; higher relapse rate
| Complication | Time | Mechanism |
|---|---|---|
| Reactionary haemorrhage | Within 24 hrs | Vessel slippage |
| Tetany / Hypocalcaemia | 24-72 hrs | Accidental parathyroid removal or devascularization |
| RLN injury (hoarseness) | Immediate | Nerve division or traction |
| Thyroid storm | Intra/post-op | Surge of thyroid hormones (if inadequate pre-op preparation) |
| Hypothyroidism | Weeks-months | Over-resection |
| Wound infection | 3-5 days |
Summary Table: Comparison of Treatment Options
| Modality | Advantage | Disadvantage |
|---|---|---|
| ATDs | Non-invasive; first-line; safe in pregnancy | Relapse common (50-70%); agranulocytosis risk; long course |
| RAI (¹³¹I) | Simple, outpatient, effective | Hypothyroidism; contraindicated in pregnancy/active GO |
| Surgery | Immediate cure; removes large goitre | Requires general anaesthesia; risk of RLN/parathyroid injury |
Key Exam Points
- Primary thyrotoxicosis = Graves' disease = diffuse toxic goitre = autoimmune (TRAb)
- Young women; nervous system symptoms predominate
- Five cardinal signs: Eye signs, goitre (with bruit/thrill), tachycardia (sleeping pulse), hot & moist palms, tremor
- Von Graefe's sign (lid lag on looking down), Stellwag's sign (staring + infrequent blinking), Joffroy's sign (no forehead wrinkling on upward gaze)
- Pre-op prep: Carbimazole + Beta-blocker + Lugol's iodine
- PTU preferred in thyroid storm (also blocks T4→T3 conversion) and 1st trimester pregnancy
- RAI contraindicated in active Graves' orbitopathy (worsens eye disease)
Write short note on hashimoto disease of thyroid.
Hashimoto's Disease of the Thyroid (Hashimoto's Thyroiditis)
Definition and Historical Note
- First described by Hakaru Hashimoto in 1912 as "struma lymphomatosa" - patients with goitre and lymphocytic infiltration of the thyroid
- The most common cause of hypothyroidism in iodine-sufficient regions (responsible for ~85% of cases)
- The most common cause of non-endemic (non-iodine-deficient) goitre in the world
- The most prevalent autoimmune disease worldwide
Epidemiology
- Age: Most prevalent between 45-65 years; can occur in children (major cause of non-endemic goitre in paediatric population)
- Sex: Strongly female predominant - F:M = 10:1 to 20:1
- Prevalence of hypothyroidism in iodine-replete populations: 1-2%; Hashimoto's is the cause in ~85%
- Tends to cluster in families; can co-occur with Graves' disease and other autoimmune diseases
Aetiology and Pathogenesis
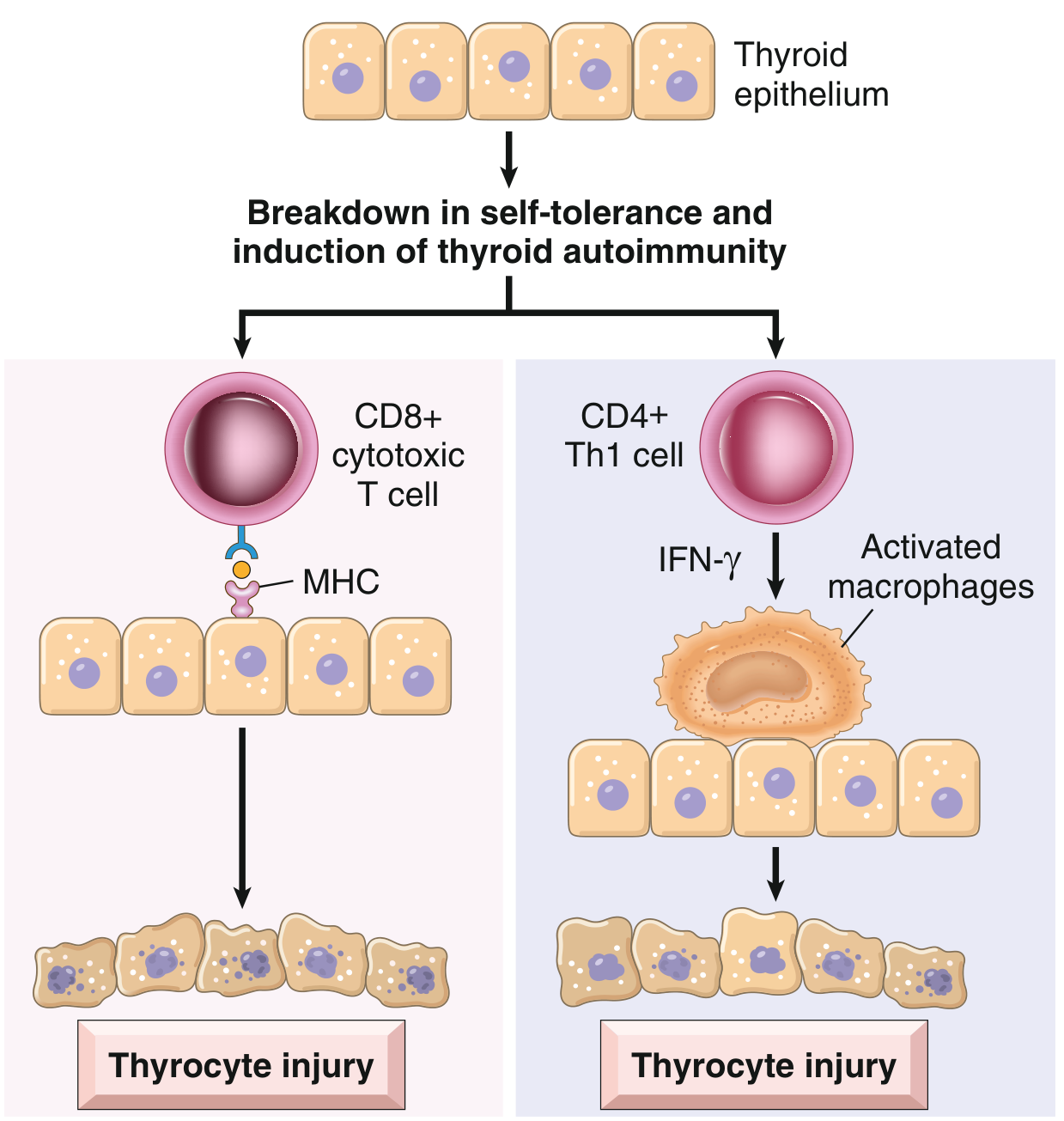
Immunological Mechanisms of Thyrocyte Destruction:
| Mechanism | Details |
|---|---|
| CD8+ Cytotoxic T-cell mediated killing | CD8+ T cells specific for thyroid antigens directly kill follicular epithelial cells via MHC presentation |
| Cytokine-mediated damage | CD4+ Th1 cells produce IFN-γ → recruits and activates macrophages → follicular damage |
| Antibody-dependent cytotoxicity | Anti-TPO and anti-thyroglobulin antibodies → ADCC or complement-dependent damage |
Key Autoantibodies:
- Anti-thyroid peroxidase (anti-TPO) antibodies - also called antimicrosomal antibodies (most sensitive marker; present in >95% of patients)
- Anti-thyroglobulin (anti-Tg) antibodies - present in majority
- These antibodies are the diagnostic hallmark but may be the consequence rather than cause of destruction
Genetic Factors:
- Strong genetic predisposition - concordance ~40% in monozygotic twins
- Associated with polymorphisms in immune regulation genes: CTLA4 (T-cell inhibitor), PTPN22, IL2RA
- Associated with HLA-DR3, HLA-DR5
Pathological Types
- Goitrogenic (Classic) form - diffuse enlargement (most common)
- Atrophic form - no goitre; thyroid fibrosis and atrophy predominate
- Fibrosing variant - extensive fibrosis; may mimic Riedel's thyroiditis
Morphology (Gross and Microscopic)
Gross
- Thyroid is diffusely and symmetrically enlarged (thyromegaly)
- Well demarcated from adjacent structures (no invasion - unlike Riedel's)
- Cut surface: pale, yellow-tan, firm, nodular
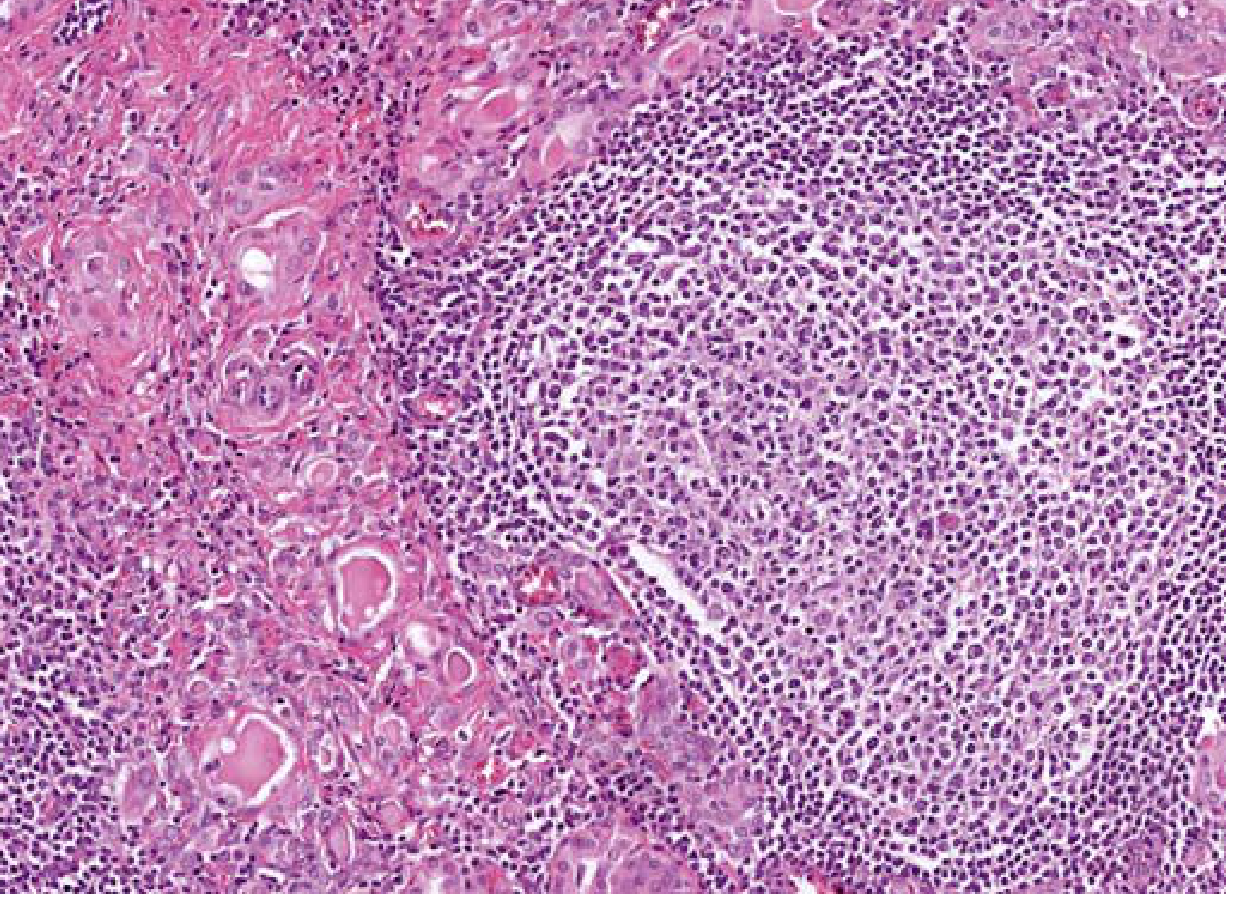
Microscopic (Histology) - Characteristic Features
| Feature | Description |
|---|---|
| Hürthle cell (Oxyphil cell) metaplasia | Follicular epithelial cells become large, eosinophilic cells with abundant granular cytoplasm (filled with mitochondria). Pathognomonic feature |
| Atrophy of thyroid follicles | Follicles are small, atrophic, contain scant colloid |
| Lymphocytic infiltration | Dense mononuclear infiltrate - small lymphocytes, plasma cells, macrophages throughout parenchyma |
| Follicle formation with germinal centres | Lymphoid follicles with well-developed germinal centres - characteristic feature |
| Fibrosis | Increased interstitial connective tissue; in fibrosing variant, extensive; does NOT extend beyond capsule (unlike Riedel's) |
Clinical Features
Presentation
- Painless, diffuse, firm enlargement of the thyroid (goitre) - most common presentation
- Gland feels rubbery to firm on palpation; may be tender
- Moves on deglutition (thyroid origin)
- Usually no bruit or thrill (unlike Graves')
- Develops slowly, often in a middle-aged woman
Phases of Thyroid Function
| Phase | Timing | Mechanism | TFTs |
|---|---|---|---|
| Hashitoxicosis | Early (transient) | Disruption of follicles → release of stored T3/T4 | ↑ T3/T4, ↓ TSH |
| Euthyroid | Intermediate | Transient normal function | Normal |
| Hypothyroid | Late (permanent) | Progressive destruction, inadequate synthesis | ↓ T3/T4, ↑ TSH |
Symptoms of Established Hypothyroidism (most patients present here)
- Weight gain despite poor appetite
- Cold intolerance; preference for warm weather
- Dry skin, coarse hair, hair loss (loss of outer 1/3 of eyebrows - characteristic)
- Puffiness of face (myxoedematous facies)
- Fatigue, lethargy, weakness (muscle fatigability)
- Constipation
- Bradycardia
- Slow speech, hoarse voice (due to myxoedema of vocal cords)
- Oligomenorrhoea / amenorrhoea
- Failing memory, depression
Compressive Symptoms (from thyromegaly)
- Dysphagia (difficulty swallowing)
- Dyspnoea (difficulty breathing)
- Cough, choking sensation
- Hoarseness (tracheal compression / RLN pressure)
- Stridor (tracheal narrowing)
Additional/Associated Symptoms
- Globus sensation
- Profound fatigue, muscle and joint pain, poor sleep, dry mouth and eyes (may persist even after thyroid hormone replacement - thought to be autoimmune-related)
Investigations
| Investigation | Finding |
|---|---|
| Serum TSH | Elevated (most sensitive test for hypothyroidism) |
| Free T4 | Low |
| Anti-TPO antibodies | Markedly elevated - hallmark test (>95% of patients) |
| Anti-thyroglobulin antibodies | Elevated (less specific) |
| Thyroid USG | Diffuse heterogeneity (characteristic "swiss-cheese" or salt-and-pepper pattern); increased vascularity; enlarged gland |
| Radioiodine scan | Low, patchy uptake |
| FNAC | Diagnostic: follicular cells + Hürthle cells + heterogeneous lymphocytes + plasma cells |
| CBC | May show anaemia |
FNAC Bethesda Categories in Hashimoto's:
- Bethesda II (Benign) - lymphocytes + colloid + Hürthle cells (most common)
- Bethesda III (AUS) - if predominantly Hürthle cells
- Bethesda IV (FN) - Hürthle cell neoplasm pattern
- Bethesda V - Hashimoto's can cause false-positive suspicious for papillary carcinoma
Associated Conditions (Complications)
| Association | Comment |
|---|---|
| Other autoimmune diseases | Type 1 diabetes, Addison's disease, pernicious anaemia, vitiligo, SLE, rheumatoid arthritis |
| Thyroid lymphoma (B-cell NHL) | Patients with Hashimoto's have higher incidence than general population; primary thyroid lymphoma almost always arises on a background of Hashimoto's |
| Papillary thyroid carcinoma | Controversial but increased predisposition suggested by morphological and molecular studies |
| Hashitoxicosis | Transient hyperthyroidism phase at onset |
| Postpartum thyroiditis | Variant; occurs within 1 year of delivery/miscarriage in up to 10% of pregnancies |
Treatment
1. Medical (Conservative) - Mainstay
- Indicated when:
- Patient is symptomatic with hypothyroidism
- TSH > 10 mIU/L (even if asymptomatic)
- Goitre with compressive symptoms
- Dose: Start low, titrate to target TSH in normal range
- Usually lifelong as gland is progressively destroyed
- Also reduces goitre size by suppressing TSH stimulation
- Beta-blockers during Hashitoxicosis (thyrotoxic phase) for palpitations, tremor
- Antithyroid drugs and RAI are NOT effective for Hashitoxicosis - the thyrotoxicosis is from hormone release (not synthesis), with suppressed iodine uptake
- Yearly screening TSH level for all patients
- Monitor for development of thyroid lymphoma or nodules
2. Surgical Treatment
- Large goitre causing significant compressive symptoms (dysphagia, stridor, tracheal compression) despite medical therapy
- Suspected thyroid malignancy (co-existing thyroid nodule suspicious on FNAC)
- Suspected thyroid lymphoma
- Cosmetically disfiguring goitre
Key Exam Points (BDS Exam Focus)
- Hashimoto's = chronic autoimmune thyroiditis = struma lymphomatosa
- Most common cause of hypothyroidism in iodine-sufficient regions
- F:M = 10:1 to 20:1; peak age 45-65 years
- Autoantibodies: anti-TPO (most sensitive) + anti-thyroglobulin
- Histology: Hürthle cell metaplasia + lymphocytic infiltrate + germinal centres + fibrosis
- Fibrosis stays within capsule (unlike Riedel's thyroiditis)
- Can start with transient Hashitoxicosis before progressing to hypothyroidism
- Increased risk of thyroid lymphoma (B-cell NHL)
- Treatment: Levothyroxine lifelong; surgery only for compression or malignancy
- Positive autoantibodies increase risk of hypothyroidism after lobectomy
Write classification of thyroid swelling. Discuss treat ment of simple goiter.
Classification of Thyroid Swellings and Treatment of Simple Goitre
Part I: Classification of Thyroid Swellings
Goitre (from Latin guttur = throat): Any enlargement of the thyroid gland, irrespective of its cause or pathology.
Classification (S. Das / Bailey & Love)
A. Non-Toxic (Simple) Goitre - Euthyroid
| Type | Features |
|---|---|
| 1. Diffuse hyperplastic (parenchymatous) | Uniform enlargement; soft; young girls; iodine deficiency / puberty / pregnancy |
| 2. Colloid goitre | Involuted hyperplastic goitre; follicles filled with colloid; firm, smooth, rubbery |
| 3. Multinodular goitre | Multiple nodules; recurrent hyperplasia + involution; middle-aged women |
| 4. Solitary nodular goitre | Single discrete nodule; must exclude malignancy |
B. Toxic Goitre (Hyperthyroid)
| Type | Eponym / Features |
|---|---|
| 1. Diffuse toxic goitre | Graves' disease; autoimmune (TSH-RAb); young women; eye signs; bruit |
| 2. Toxic multinodular goitre | Secondary thyrotoxicosis; elderly; cardiovascular symptoms predominate |
| 3. Toxic nodule (Toxic adenoma) | Single autonomous hot nodule; TSH suppressed |
C. Neoplastic
| Type | |
|---|---|
| Benign | Follicular adenoma, Hürthle cell adenoma |
| Malignant | Papillary carcinoma (most common), Follicular carcinoma, Medullary carcinoma, Anaplastic carcinoma, Thyroid lymphoma |
D. Thyroiditis (Inflammatory)
| Type | Features |
|---|---|
| 1. Acute (bacterial) thyroiditis | Suppurative; abscess; rare |
| 2. Subacute granulomatous thyroiditis | De Quervain's; viral; painful; self-limiting |
| 3. Autoimmune (Hashimoto's) | Chronic lymphocytic; anti-TPO antibodies; hypothyroidism |
| 4. Riedel's thyroiditis | "Iron-hard" thyroid; extensive fibrosis extending beyond capsule; very rare |
| 5. Chronic specific | Tuberculosis, syphilis (rare) |
E. Other / Rare
- Amyloid goitre
- Thyroid cysts (simple, haemorrhagic)
- Thyroglossal cyst (moves on tongue protrusion)
WHO Grading of Goitre (Clinical Field Classification)
| Grade | Description |
|---|---|
| Grade 0 | No goitre (thyroid not palpable or visible) |
| Grade 1 | Goitre palpable but not visible with neck in normal position |
| Grade 2 | Goitre visible with neck in normal position; clearly palpable |
Part II: Simple Goitre - Definition, Aetiology, Pathology
Definition
- Non-toxic (patient is euthyroid)
- Non-inflammatory (no thyroiditis)
- Non-neoplastic
Types
- Common in mountainous areas (Himalayas, Andes, Alps, Vindhyas, Satpura ranges in India)
- Iodine content of soil and water is very low
- More common in adolescent girls and during pregnancy
Aetiology
| Cause | Mechanism |
|---|---|
| Iodine deficiency (most important for endemic) | ↓ iodine → ↓ T3/T4 synthesis → ↑ TSH → thyroid hyperplasia |
| Goitrogens | Dietary substances interfere with hormone synthesis. Brassica family vegetables (cabbage, kale, turnip, cauliflower, Brussels sprouts), cassava (contains thiocyanate that inhibits iodide transport) |
| Dyshormonogenesis | Hereditary enzyme defects (autosomal recessive) impairing thyroid hormone synthesis |
| Physiological states | Puberty, pregnancy - increased demand for thyroid hormone → relative deficiency → compensatory goitre |
| Growth factors | Immunoglobulins and local growth factors (not just TSH) also stimulate thyroid cell proliferation |
Pathology - Stages of Simple Goitre
| Stage | Gross | Microscopic |
|---|---|---|
| Phase 1: Diffuse hyperplastic | Uniform, diffuse, smooth, soft enlargement (rarely >100-150g) | Follicular cell hypertrophy + hyperplasia; columnar cells; scanty colloid; papillary projections |
| Phase 2: Colloid involution | Gland enlarges further; cut surface: brown, translucent, glistening | Follicles distended with colloid; flat cuboidal epithelium; minimal cellularity |
| Phase 3: Multinodular (irreversible) | Asymmetric, irregular, nodular gland; may have haemorrhage, cysts, calcification | Mixed areas of hyperplasia and involution; nodules of varying size; fibrosis |
Clinical Features of Simple Goitre
- Painless anterior neck swelling - slowly progressive
- Cosmetic concern
- Compression symptoms (in large goitres):
- Dysphagia (oesophageal compression)
- Dyspnoea, stridor (tracheal compression)
- Hoarseness (recurrent laryngeal nerve pressure)
- Choking, cough
- Sensation of fullness or discomfort in the neck
- Thyroid enlargement - diffuse (early) or nodular (late)
- Moves upward on deglutition (pathognomonic of thyroid origin)
- Soft (hyperplastic) → rubbery/firm (colloid) → hard with irregular nodules (multinodular)
- No bruit or thrill (unlike Graves')
- No eye signs
- Pulse normal (euthyroid)
- Tracheal deviation may be present in large goitres
- Pemberton's sign - flushing and venous engorgement of face/neck when both arms are raised above the head (indicates retrosternal extension causing SVC compression)
- Secondary thyrotoxicosis (in up to 30% - especially multinodular goitre)
- Haemorrhage into a nodule - sudden painful swelling; may cause acute airway obstruction
- Tracheal compression/obstruction (retrosternal extension)
- Malignant change - increased incidence of follicular carcinoma in endemic areas; dominant or rapidly growing nodules must be investigated
- Cosmetic disfigurement
- Retrosternal extension
Part III: Treatment of Simple Goitre
A. Prevention (Endemic Goitre)
- Iodised salt - addition of potassium iodate to common salt (most effective public health measure)
- Has strikingly reduced the incidence of endemic goitre in iodine-deficient regions
- Iodised oil injections (in severely deficient remote areas)
- Iodine supplementation in drinking water
B. Medical Treatment
1. Thyroxine (Levothyroxine - LT4) Therapy
- Mechanism: Exogenous thyroxine suppresses TSH → removes stimulus for thyroid growth
- Indication: Early hyperplastic (diffuse) stage of simple goitre
- Dose: 0.15-0.2 mg (150-200 μg) daily for several months
- Outcome: Hyperplastic goitre may regress significantly with thyroxine therapy
- Important limitation: The nodular stage is irreversible - thyroxine will NOT reduce a long-standing nodular goitre
- Continue for at least 6-12 months; monitor TSH
2. Iodine Supplementation
- In pure iodine-deficient hyperplastic goitres in children/adolescents:
- Potassium iodide or iodised salt supplementation
- Effective in early diffuse hyperplastic stage
- Leads to colloid involution → gland softens and reduces in size
- Not effective in established nodular goitre
- Caution: Excess iodine in patients with pre-existing multinodular goitre can precipitate hyperthyroidism (Jöd-Basedow phenomenon)
3. Observation / Watchful Waiting
- Most patients with multinodular goitre are asymptomatic
- More than half of benign nodules will regress in size over 10 years without intervention
- Serial USG and TFT monitoring every 6-12 months
- Indicated: asymptomatic, no suspicious features, no compression, small goitre
C. Surgical Treatment
Indications for Surgery
- Pressure symptoms - dysphagia, stridor, tracheal compression/deviation (if no other treatable cause)
- Suspected or confirmed malignancy - dominant nodule, rapid growth, hard irregular nodule, suspicious FNAC
- Cosmetic - patient finds goitre unsightly and disfiguring
- Retrosternal goitre - causing SVC compression or respiratory symptoms
- Failure of medical treatment - goitre enlarging despite thyroxine
- Development of secondary thyrotoxicosis with pressure symptoms
- Haemorrhage into a nodule causing acute airway compromise
Choice of Surgical Procedure
| Situation | Preferred Procedure |
|---|---|
| Bilateral multinodular goitre | Total thyroidectomy (preferred now - avoids regrowth, eliminates risk of remnant cancer) |
| Historically used for bilateral disease | Subtotal thyroidectomy (leaving 4-8g of tissue per remnant) - higher relapse/regrowth rate |
| Asymmetric disease (one lobe more involved) | Total lobectomy of the more affected side |
| Asymmetric + significant contralateral involvement | Dunhill procedure (total lobectomy one side + subtotal other side) |
| Retrosternal goitre | Cervical incision usually sufficient; rarely requires sternal split |
Important Surgical Considerations
- Reoperation for recurrent nodular goitre is more hazardous (adhesions, distorted anatomy)
- For this reason, many surgeons prefer total thyroidectomy in younger patients as initial procedure
- Post-total thyroidectomy: lifelong levothyroxine replacement required
- In many cases, causative factors persist (iodine deficiency, goitrogens) and recurrence is likely if only partial resection performed
Post-operative Complications
| Complication | Time | Mechanism |
|---|---|---|
| Reactionary haemorrhage | 0-24 hrs | Vessel slippage; can cause airway compromise |
| Tetany / hypocalcaemia | 24-72 hrs | Parathyroid removal/devascularization |
| RLN injury (hoarseness) | Immediate | Nerve traction/division |
| Hypothyroidism | Weeks-months | Over-resection of functional tissue |
| Recurrence of goitre | Months-years | Residual tissue + continued TSH stimulation |
| Wound infection | 3-5 days |
Summary of Treatment Approach
Simple Goitre
│
├── Hyperplastic (early, diffuse) → MEDICAL: Thyroxine 150-200 μg/day
│ + Iodine supplementation (if endemic)
│
├── Colloid / Asymptomatic nodular → OBSERVATION: Monitor TFTs + USG
│
└── Nodular with symptoms / suspicion / large size → SURGICAL
│
├── Bilateral → Total thyroidectomy (preferred)
└── Asymmetric → Lobectomy of affected side
Define and classify goiters. Describe differentiating features between primary and secondary thyrotoxicosis along with medical treatment to make patient euthyroid.
Definition and Classification of Goitres + Primary vs Secondary Thyrotoxicosis + Medical Treatment
PART I: Definition and Classification of Goitre
Definition
Goitre (from Latin guttur = throat): Any enlargement of the thyroid gland, irrespective of its aetiology, pathology, or functional status.
Classification of Goitre
A. Non-Toxic (Simple) Goitre - Euthyroid
| Type | Features |
|---|---|
| 1. Diffuse hyperplastic (parenchymatous) | Uniform, soft; young girls; iodine deficiency / puberty / pregnancy |
| 2. Colloid goitre | Involuted hyperplastic goitre; follicles distended with colloid; firm, rubbery |
| 3. Multinodular goitre | Recurrent hyperplasia + involution; asymmetric, irregular, nodular; middle-aged women |
| 4. Solitary nodular goitre | Single discrete nodule; must always exclude malignancy |
B. Toxic Goitre (Thyrotoxic - Hyperthyroid)
| Type | Description |
|---|---|
| 1. Primary (Diffuse toxic) | Graves' disease; autoimmune (TSH-RAb); in previously healthy gland; young women |
| 2. Secondary (Toxic multinodular) | Toxicity superimposed on pre-existing nodular goitre; middle-aged/elderly |
| 3. Toxic adenoma | Single autonomous hot nodule; TSH suppressed |
C. Neoplastic
| Type | Examples |
|---|---|
| Benign | Follicular adenoma, Hürthle cell adenoma |
| Malignant | Papillary carcinoma (most common), Follicular carcinoma, Medullary carcinoma, Anaplastic carcinoma, Malignant lymphoma |
D. Thyroiditis (Inflammatory)
| Type | Eponym |
|---|---|
| Acute bacterial (suppurative) | Rare; post-URTI |
| Subacute granulomatous | De Quervain's thyroiditis; viral; painful |
| Chronic autoimmune | Hashimoto's thyroiditis; anti-TPO antibodies |
| Fibrosing | Riedel's thyroiditis; iron-hard; fibrosis beyond capsule |
| Chronic specific | Tuberculosis, syphilis (rare) |
E. Miscellaneous / Rare
- Amyloid goitre
- Thyroglossal cyst (moves on tongue protrusion)
- Thyroid cysts
WHO Grading of Goitre
| Grade | Description |
|---|---|
| Grade 0 | No goitre - not palpable or visible |
| Grade 1 | Palpable but not visible in normal neck position |
| Grade 2 | Clearly visible in normal position AND palpable |
PART II: Differentiating Features Between Primary and Secondary Thyrotoxicosis
Thyrotoxicosis = clinical syndrome of excess circulating thyroid hormones Primary thyrotoxicosis = hyperthyroidism arising in a previously healthy gland (Graves' disease) Secondary thyrotoxicosis = hyperthyroidism superimposed on a previously diseased gland (usually longstanding multinodular goitre)
Comparison Table: Primary vs Secondary Thyrotoxicosis
| Feature | Primary Thyrotoxicosis (Graves') | Secondary Thyrotoxicosis |
|---|---|---|
| Aetiology | Autoimmune - TSH receptor-stimulating antibodies (TSH-RAb / LATS) in previously healthy gland | Toxicity develops in longstanding nodular goitre or colloid goitre |
| Age | Young women (20s-30s) | Middle-aged to elderly (40s-60s) |
| Sex | Females >> Males (8:1) | Females >> Males |
| Previous history | No prior thyroid disease | Pre-existing goitre for many years |
| System primarily affected | Nervous system (hallmark) | Cardiovascular system (hallmark) |
| Weight loss | Marked - weight loss despite good appetite | May be present but less dramatic |
| Nervous symptoms | Prominent: nervousness, irritability, insomnia, emotional lability, poor concentration | Mild or absent |
| Tremor | Characteristic fine tremor of hands and tongue | Usually absent |
| Cardiovascular symptoms | Present but less pronounced - palpitations, tachycardia | Predominant: severe palpitations, ectopic beats, arrhythmias, cardiac failure |
| Atrial fibrillation | Occasional | Very common; often the presenting feature |
| Cardiac failure | Uncommon | Common in late stages |
| Pulse | Rapid (tachycardia); sleeping pulse elevated | Rapid AND irregular (AF); pulse may be irregular even at rest |
| Eye signs | Characteristic and prominent: exophthalmos, lid retraction, Von Graefe's sign, Stellwag's sign, Joffroy's sign, ophthalmoplegia, diplopia | Absent or minimal |
| Goitre | Diffuse, smooth, uniform enlargement; firm; bruit and thrill present (increased vascularity) | Pre-existing nodular (multinodular or solitary) goitre; NO bruit |
| Skin | Hot, moist, warm palms; sweating | Less pronounced |
| Exophthalmos | Present (pathognomonic of Graves') | Absent |
| Pretibial myxoedema | May be present (specific to Graves') | Absent |
| Acropachy | Rarely present | Absent |
| Thyroid antibodies (TRAb) | Markedly elevated | Negative / low titre |
| Radioiodine scan | Diffuse, uniform uptake throughout both lobes | Patchy/nodular uptake; hot and cold areas |
| BMR | Elevated (often +100%) | Elevated but usually less than primary |
| Prognosis | Responds well to antithyroid drugs and surgery | Antithyroid drugs only temporize; surgery or RAI required for cure |
| Remission with ATDs | Possible (~30-50% after 12-18 months) | Recurrence certain on stopping drugs (autonomous tissue) |
Key Differentiating Mnemonic
- Young woman + Nervous system symptoms + Eye signs + Diffuse smooth goitre with bruit
- Older patient + Cardiac symptoms (AF, CCF) + No eye signs + Pre-existing nodular goitre, irregular pulse
PART III: Medical Treatment to Make the Patient Euthyroid
Step 1: Beta-Adrenergic Blockade (Immediate Symptom Control)
| Drug | Dose | Notes |
|---|---|---|
| Propranolol | 40-80 mg TDS/QDS | Drug of choice; blocks adrenergic effects AND blocks peripheral T4→T3 conversion |
| Atenolol | 25-100 mg OD-BD | β1-selective; less effective for tremor |
| Metoprolol | 25-50 mg BD-TDS | β1-selective; useful in mild asthma |
| Esmolol | IV, short-acting | For acute/thyroid storm; if beta-blockers relatively contraindicated |
- Controls tachycardia, palpitations, tremor, anxiety, sweating, heat intolerance
- Blocks peripheral conversion of T4 to T3 (propranolol specifically)
- Used until patient becomes euthyroid with ATDs
- Contraindicated in: Asthma, COPD (use esmolol/metoprolol cautiously); severe congestive heart failure
Step 2: Antithyroid Drugs (ATDs) - Thionamides
Drugs Available
| Drug | Dose (Initial) | Dose (Maintenance) | Notes |
|---|---|---|---|
| Carbimazole | 10-15 mg TDS (30-45 mg/day) | 5 mg OD-BD | Most commonly used in India/UK; metabolised to methimazole |
| Methimazole (MMI) | 10-20 mg BD-TDS | 5-10 mg OD | Active drug of carbimazole; preferred over PTU (except in specific situations) |
| Propylthiouracil (PTU) | 100-150 mg TDS | 50 mg OD-BD | Additionally blocks peripheral T4→T3 conversion; preferred in thyroid storm and 1st trimester pregnancy |
Duration of Treatment
- 12 to 18 months (results not improved beyond 18 months)
- Start high dose → reduce to maintenance once euthyroid (usually 4-8 weeks)
- Monitor TFTs every 4-6 weeks; aim: TSH in normal range
- After stopping, monitor for relapse
Expected Outcomes
- Primary thyrotoxicosis (Graves'): Remission in 30-50% after 12-18 months
- Relapse rate: 20-30% over 3-5 years after stopping
- Secondary thyrotoxicosis: Recurrence certain on stopping drugs (autonomous tissue not suppressible) - ATDs only temporize before definitive treatment
Adverse Effects of ATDs
| Side Effect | Drug | Action |
|---|---|---|
| Agranulocytosis (most serious) | Both, but PTU > MMI | STOP drug immediately if fever/sore throat; check WBC; neutrophil count <500/µL confirms diagnosis |
| Skin rash, urticaria | Both | Mild; may switch to other drug |
| Hepatotoxicity (cholestatic) | MMI | Monitor LFTs |
| Hepatocellular injury / fulminant liver failure | PTU | FDA black box warning 2010; avoid PTU in children |
| Vasculitis (ANCA-positive) | PTU | Rare |
| Hypothyroidism (over-treatment) | Both | Reduce dose; monitor TSH |
Step 3: Iodine (Adjunct - Pre-operative Use Only)
- Wolff-Chaikoff effect: High iodine transiently suppresses thyroid hormone synthesis and release
- Reduces vascularity and firmness of the gland
- Used pre-operatively for 10-14 days before thyroidectomy - reduces intraoperative bleeding
- NOT used for long-term medical control - escape phenomenon (Jöd-Basedow) occurs after 10-14 days
- Must be given AFTER antithyroid drugs are started (iodine given first can worsen thyrotoxicosis by providing substrate for more hormone synthesis)
Step 4: Corticosteroids (Adjunct in Severe Thyrotoxicosis)
- Hydrocortisone / Dexamethasone
- Block peripheral conversion of T4 to T3
- Treat possible associated adrenal insufficiency
- Used mainly in thyroid storm or severe thyrotoxicosis with ophthalmopathy
- Not a routine part of treatment to achieve euthyroidism
Summary of Medical Treatment Algorithm
Thyrotoxicosis diagnosed
│
▼
Step 1: Beta-blocker (Propranolol) → Immediate symptom control
│
▼
Step 2: Antithyroid drug (Carbimazole/MMI) → Blocks hormone synthesis
[PTU preferred: thyroid storm, 1st trimester pregnancy]
│
4-8 weeks
│
▼
Euthyroid state achieved
│
┌────┴────┐
│ │
Continue If relapse or
12-18 months autonomous nodule
│ │
Remission? Definitive Rx:
YES → Stop RAI or Surgery
NO → Definitive Rx
When Medical Treatment is NOT Sufficient (Definitive Treatment Needed)
| Situation | Preferred Treatment |
|---|---|
| Relapse after ATDs | RAI or surgery |
| Secondary thyrotoxicosis (autonomous nodules) | Surgery or RAI (ATDs will never cure this) |
| Adverse reaction to ATDs | RAI or surgery |
| Large goitre with pressure symptoms | Surgery (thyroidectomy) |
| Active Graves' orbitopathy | Surgery (preferred over RAI) |
| Pregnancy | ATDs carefully (PTU 1st trimester, MMI 2nd-3rd trimester) |
Enlist midline neck swellings. Describe surgical anatomy of thyroid gland with reference to embryology, blood supply relationship and nerves related to thyroid gland.
Midline Neck Swellings + Surgical Anatomy of the Thyroid Gland
PART I: Midline Neck Swellings
Classification of Midline Neck Swellings
A. Congenital
- Thyroglossal cyst (most common midline neck swelling) - cyst along the thyroglossal duct tract; moves upward on tongue protrusion and on swallowing
- Thyroglossal fistula - usually post-infected/ruptured thyroglossal cyst
- Dermoid cyst - at the root of the nose, above the hyoid (sublingual dermoid), or below the hyoid; does NOT move on swallowing or tongue protrusion
- Ectopic thyroid (lingual thyroid, sublingual thyroid) - thyroid tissue at the base of the tongue or along the thyroglossal tract
- Thymic cyst (rare) - remnant of thymic descent
B. Acquired - Thyroid Origin
- Goitre (any type) - moves upward on swallowing (most characteristic sign)
- Simple/colloid goitre
- Multinodular goitre
- Toxic goitre (Graves')
- Thyroid carcinoma
- Thyroiditis (Hashimoto's, De Quervain's)
- Thyroid cyst - moves on swallowing
C. Acquired - Non-Thyroid
- Subhyoid bursa - between hyoid bone and thyrohyoid membrane; moves on swallowing
- Pre-laryngeal lymph node (Delphian node) - sentinel node in thyroid malignancy; moves on swallowing
- Pre-tracheal lymph nodes - inflammatory or metastatic
- Lipoma - soft, lobulated; does NOT move on swallowing
- Sebaceous cyst / epidermoid cyst - attached to skin; moves with skin
D. Vascular
- Aneurysm of the aortic arch (rare) - pulsatile; retrosternal extension
Key Clinical Differentiating Features
| Swelling | Moves on Swallowing | Moves on Tongue Protrusion | Other Features |
|---|---|---|---|
| Thyroid goitre | YES | NO | Most common midline swelling overall |
| Thyroglossal cyst | YES | YES (pathognomonic) | Most common true midline swelling; at/below hyoid |
| Subhyoid bursa | YES | NO | At hyoid level |
| Dermoid cyst | NO | NO | Smooth, doughy, transilluminates |
| Lipoma | NO | NO | Soft, lobulated |
| Sebaceous cyst | NO | NO | Attached to skin, punctum visible |
PART II: Surgical Anatomy of the Thyroid Gland
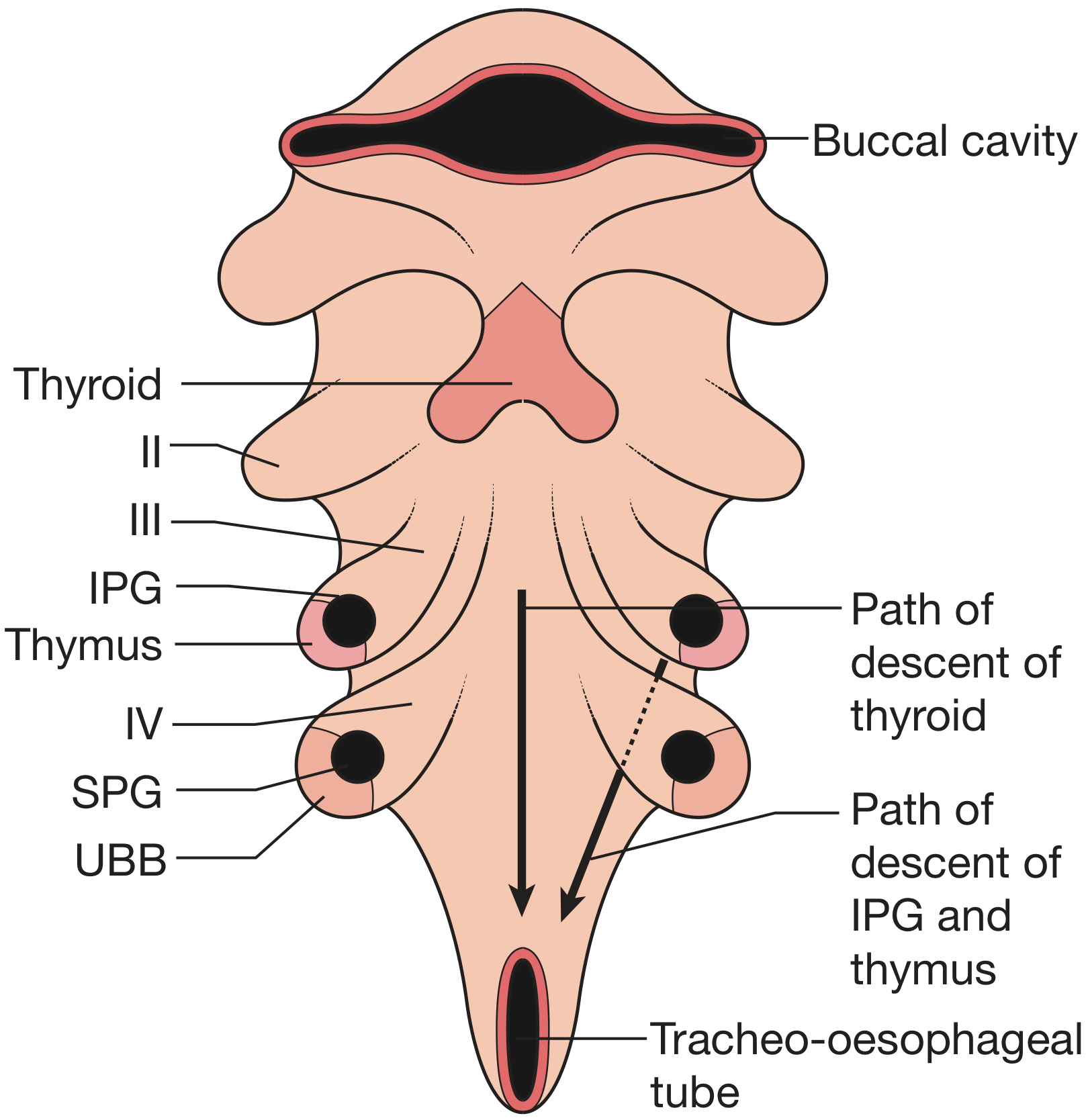
1. Embryology
Origin of the Thyroid
- The thyroid develops from the median bud (endodermal thickening) of the pharynx at the floor of the primitive pharynx
- This originates between the 1st and 2nd pharyngeal arches at the site that becomes the foramen caecum (at the junction of the anterior 2/3 and posterior 1/3 of the tongue)
- This median diverticulum is called the thyroglossal duct
- The thyroid migrates caudally (downward) from the foramen caecum, passing closely in relation to (and sometimes through) the developing hyoid cartilage
- It descends anterior to the larynx and trachea to reach its final position in the neck
- The thyroglossal duct normally obliterates and disappears by the 8th week
- Foramen caecum = vestigial remnant of this duct, visible on the tongue
Surgical Significance of Embryology
| Remnant/Anomaly | Clinical Significance |
|---|---|
| Thyroglossal cyst | Cystic dilatation of remnant thyroglossal duct; presents as midline neck swelling; moves on tongue protrusion |
| Thyroglossal fistula | Opens at skin after rupture/incision of cyst |
| Lingual thyroid | Failure of descent; thyroid tissue at foramen caecum base of tongue (may be only functioning thyroid tissue - must confirm by scan before excision) |
| Ectopic thyroid | Thyroid tissue anywhere along the path of descent |
| Pyramidal lobe | Remnant of caudal end of thyroglossal duct; small upward projection from isthmus (present in 50% of individuals) |
Origin of Parathyroid Glands
- Superior parathyroid glands (2) → from 4th pharyngeal pouch; constant in position on posterior surface of upper thyroid lobe
- Inferior parathyroid glands (2) → from 3rd pharyngeal pouch (same as thymus)
- The thymus descends from the 3rd pouch and carries the inferior parathyroid with it
- This explains why the inferior parathyroid is more variable in position - may be found anywhere from jaw to mediastinum along the line of thymic descent
Origin of Parafollicular C Cells
- C cells (parafollicular cells - produce calcitonin) arrive in the thyroid via the ultimobranchial body (5th pharyngeal pouch) from the neural crest
- C cells are the cell of origin of medullary thyroid carcinoma
2. Gross Anatomy of the Thyroid Gland
Size, Weight, and Shape
- Weight: 20-25 g (normal adult)
- Shape: Butterfly-shaped (H-shaped)
- Components:
- Two lateral lobes (right and left) - each ~5 cm long, 3 cm wide, 2 cm thick
- Isthmus - connects the two lobes; overlies the 2nd-4th tracheal rings
- Pyramidal lobe - present in ~50%; upward projection from isthmus (usually left of midline); represents caudal end of thyroglossal duct
Capsule and Fascia
- Enclosed in a true fibrous capsule (from which septa divide the gland into lobules)
- Surrounded by a false capsule (surgical capsule) - a condensation of pretracheal fascia
- The space between true and false capsule contains the parathyroid glands and branches of blood vessels
3. Relations of the Thyroid Gland (Surgical Importance)
Anterior Relations (Superficial to Deep)
- Skin
- Superficial fascia + platysma
- Deep fascia (investing layer)
- Strap muscles: Sternohyoid, Sternothyroid (directly overlying lobes), Omohyoid
- Sternocleidomastoid (laterally)
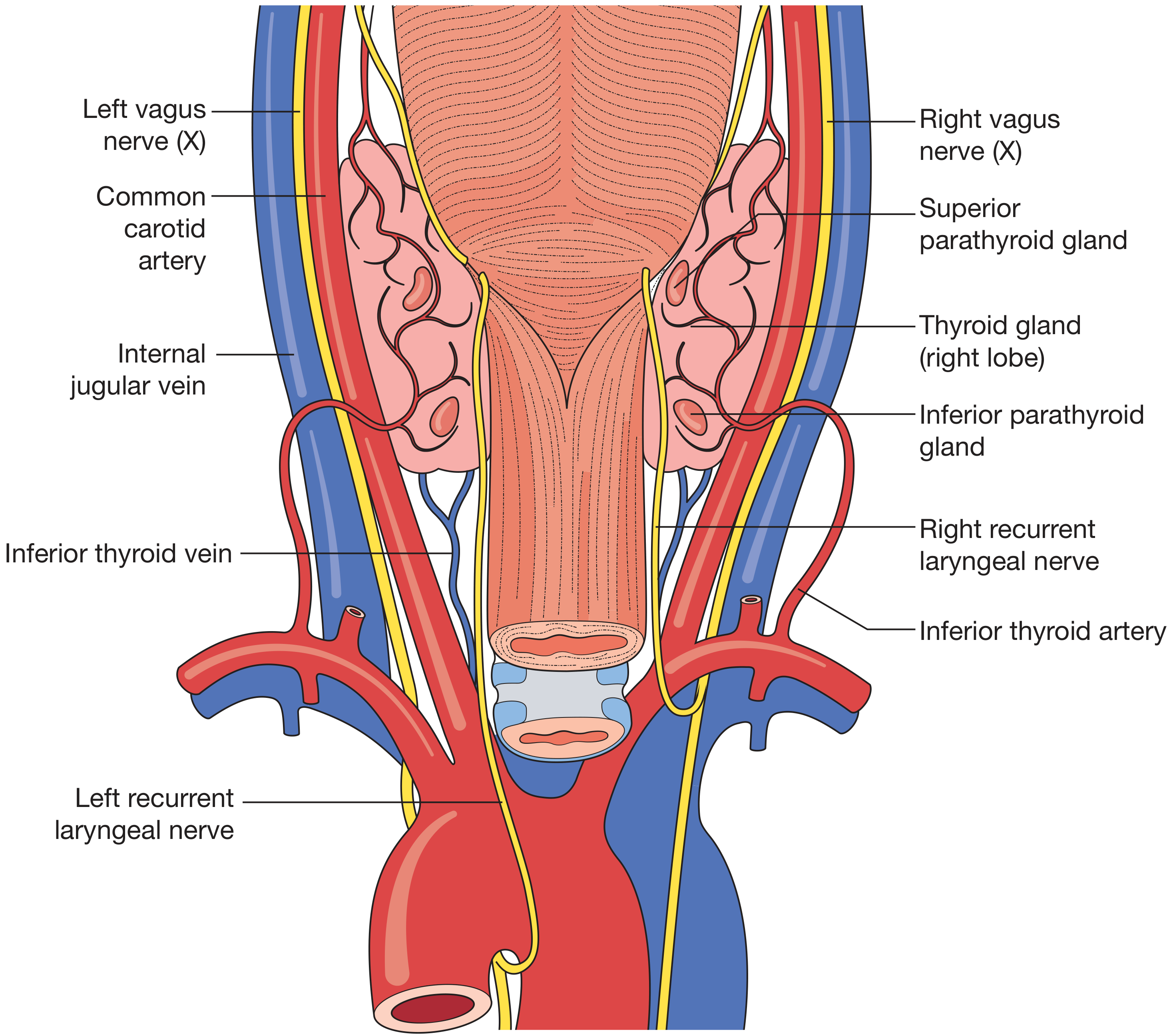
Posterior Relations (Critical for Surgery)
- Trachea and larynx (medially) - isthmus overlies 2nd-4th tracheal rings
- Oesophagus - posterior to trachea; may be deviated by goitre
- Parathyroid glands - 4 glands on posterior surface between true and false capsule
- Recurrent laryngeal nerve (RLN) - in the tracheo-oesophageal groove on each side
- Carotid sheaths (common carotid artery, internal jugular vein, vagus nerve) - laterally
Berry's Ligament (Ligament of Berry)
- Condensation of pretracheal fascia binding the thyroid to the trachea and cricoid cartilage
- Located just caudal to the cricoid cartilage
- The RLN is at highest risk of injury at this point during thyroidectomy
- Contains small branches of the inferior thyroid artery and small veins
Tubercle of Zuckerkandl
- Posterior projection of the thyroid lobe
- The RLN is normally found just deep to this structure
- Useful landmark for identifying the RLN during surgery
4. Blood Supply
Arterial Supply
- Origin: First branch of the external carotid artery
- Course: Runs anteroinferiorly, deep to infrahyoid muscles, to the superior pole of the gland
- Divides into anterior and posterior branches at the superior pole
- Branches: Superior laryngeal artery (branch of external carotid or superior thyroid artery - supplies larynx)
- Surgical importance: The external branch of the superior laryngeal nerve (EBSLN) runs with the superior thyroid artery and must be identified and preserved when ligating the superior pole vessels. The nerve supplies the cricothyroid muscle; injury causes change in voice pitch/quality
- Origin: Thyrocervical trunk → from the subclavian artery (1st part)
- Course: Runs superiorly over scalenus anterior → passes medially posterior to the carotid sheath → reaches the posterior surface of the lower thyroid lobe
- Most important branch for surgery - supplies both parathyroid glands (primary blood supply to all 4 parathyroid glands)
- Surgical importance: The recurrent laryngeal nerve (RLN) crosses the inferior thyroid artery - variably passing anterior, posterior, or between its branches at this point. This relationship is the most dangerous in thyroid surgery
- Present in 8-10% of individuals (anatomical variant)
- Origin: Brachiocephalic artery, aortic arch, right common carotid, or subclavian artery
- Ascends in the midline anterior to the trachea
- Surgical importance: Must be ligated carefully during midline approaches; unexpected bleeding in the midline may be from this vessel
- Extensive anastomoses occur between superior and inferior thyroid arteries
- Also anastomose with tracheal and oesophageal arteries
- Makes ligation near the gland (rather than main trunk) important to avoid devascularising parathyroids
Venous Drainage
| Vein | Drains Into | Notes |
|---|---|---|
| Superior thyroid vein | Internal jugular vein | Follows the superior thyroid artery closely |
| Middle thyroid vein | Internal jugular vein | Short, broad; drains from lateral border of gland; no corresponding artery; must be ligated to mobilize the thyroid medially |
| Inferior thyroid vein | Left brachiocephalic vein (both sides) | Present in ~50%; multiple trunks from lower pole; run inferiorly anterior to trachea |
5. Nerves Related to the Thyroid Gland
A. Recurrent Laryngeal Nerve (RLN) - Most Important Nerve in Thyroid Surgery
| Side | Origin | Loop | Course to Larynx |
|---|---|---|---|
| Right RLN | Right vagus nerve as it crosses anterior to right subclavian artery | Loops under (posterior to) right subclavian artery | Ascends obliquely in tracheo-oesophageal groove; more lateral/oblique course |
| Left RLN | Left vagus nerve as it crosses anterior to aortic arch | Loops under aortic arch (ligamentum arteriosum) | Ascends more medially in tracheo-oesophageal groove |
- Enters the larynx at the cricothyroid joint (level of Berry's ligament)
- This is the point of highest surgical risk
- Motor: All intrinsic laryngeal muscles EXCEPT cricothyroid (which is supplied by EBSLN)
- Sensory: Laryngeal mucosa below the vocal cords
- Note: Only the inferior laryngeal branch (terminal branch of RLN) supplies laryngeal musculature; other branches are sensory - injury to sensory branches may cause aspiration
- Three sides: Common carotid artery + inferior thyroid artery + RLN
- The RLN lies in the angle between these structures, in the tracheo-oesophageal groove
- Non-recurrent RLN (right side): ~2% of right-sided nerves; enters larynx directly from above without looping around subclavian artery (associated with aberrant right subclavian artery - arteria lusoria)
- Non-recurrent left RLN: Extremely rare; associated with right-sided aortic arch
- RLN may divide into 2-3 branches before entering larynx - must identify ALL branches
| Type | Effect |
|---|---|
| Unilateral complete RLN injury | Hoarseness (ipsilateral vocal cord paralysis in paramedian position) |
| Bilateral complete RLN injury | Severe respiratory distress; stridor; may need tracheostomy |
| Unilateral partial injury | Voice changes, aspiration |
B. External Branch of the Superior Laryngeal Nerve (EBSLN) - "The Voice Nerve"
- Internal branch (sensory): Pierces thyrohyoid membrane; supplies laryngeal mucosa above vocal cords
- External branch (motor): Runs along the lateral border of pharyngeal constrictor muscles → supplies cricothyroid muscle
- EBSLN runs with the superior thyroid artery near the superior pole
- Cernea Classification of EBSLN-superior thyroid artery relationship:
- Type 1: Nerve crosses >1 cm above upper pole vessels - SAFE
- Type 2a: Nerve crosses within 1 cm of upper pole - CAUTION
- Type 2b: Nerve crosses below the upper border of the superior pole - HIGH RISK OF INJURY
- Loss of cricothyroid muscle function → inability to tense vocal cord
- Loss of high notes, fatigue on prolonged speaking, change in voice quality (singers most affected)
- Called "the nerve of Amelita Galli-Curci" (famous soprano whose voice was damaged during thyroid surgery)
C. Cervical Sympathetic Trunk
- Lies posterior to the carotid sheath
- May be compressed or involved by large thyroid tumours
- Horner's syndrome (enophthalmos, pseudoptosis, miosis, anhidrosis) if involved
6. Lymphatic Drainage
- Subcapsular plexus drains to:
- Central compartment (Level VI): Pre-tracheal, paratracheal, and "Delphian" node (pre-laryngeal - Sentinel node; when enlarged, indicates thyroid malignancy)
- Deep cervical nodes (Levels II, III, IV, V)
- Mediastinal nodes (Level VII)
- Knowledge of lymphatic drainage is essential for central neck dissection in thyroid malignancy
7. Functioning Unit - Histology
- The functional unit of the thyroid is the follicle (acinus)
- Each lobule (supplied by a single arteriole) contains 24-40 follicles
- Follicles are lined by cuboidal epithelium (flat in involution, columnar in hyperplasia)
- Follicle lumen contains colloid = storage form of thyroglobulin (contains T3 and T4 bound to thyroglobulin)
- C cells (parafollicular cells) lie between follicles; produce calcitonin; derived from neural crest via ultimobranchial body
Summary Diagram: Key Relationships in Thyroid Surgery
| Structure | Relationship | Risk if Damaged |
|---|---|---|
| RLN | In tracheo-oesophageal groove; crosses inferior thyroid artery; at greatest risk at Berry's ligament | Hoarseness (unilateral) / Stridor (bilateral) |
| EBSLN | Runs with superior thyroid artery at superior pole | Loss of voice pitch/quality |
| Parathyroid glands | Between true and false capsule, posterior surface; blood supply from inferior thyroid artery | Hypocalcaemia, tetany |
| Trachea | Medial - isthmus overlies 2nd-4th rings | Airway compromise if compressed by goitre |
| Oesophagus | Posterior to trachea | Dysphagia if compressed |
| Carotid sheath | Lateral to each lobe | Carotid/IJV injury if invaded by malignancy |
Classify thyroid swellings. Describe pathogenesis, clinical features and management of multinodular goiter.
Classification of Thyroid Swellings + Multinodular Goitre
PART I: Classification of Thyroid Swellings
Goitre (Latin guttur = throat): Any enlargement of the thyroid gland, irrespective of its cause or pathology.
A. Non-Toxic (Simple) Goitre - Euthyroid
| Type | Features |
|---|---|
| 1. Diffuse hyperplastic (parenchymatous) | Uniform, soft enlargement; puberty/pregnancy/iodine deficiency; TSH-driven |
| 2. Colloid goitre | Involuted hyperplastic goitre; follicles filled with colloid; firm, smooth, rubbery; age 20-30 |
| 3. Multinodular goitre | Multiple nodules; recurrent hyperplasia + involution; asymmetric; females >> males |
| 4. Solitary nodular goitre | Single palpable nodule; must always exclude malignancy |
B. Toxic Goitre (Hyperthyroid)
| Type | Features |
|---|---|
| 1. Primary diffuse toxic (Graves') | Autoimmune; TSH-RAb; young women; eye signs; diffuse bruit |
| 2. Secondary toxic (multinodular) | Pre-existing nodular goitre becomes toxic; elderly; cardiac features |
| 3. Toxic adenoma (solitary) | Single autonomous hot nodule; suppressed surrounding tissue |
C. Neoplastic
| Type | |
|---|---|
| Benign | Follicular adenoma, Hürthle cell adenoma |
| Malignant | Papillary Ca (most common), Follicular Ca, Medullary Ca, Anaplastic Ca, Thyroid lymphoma |
D. Thyroiditis
| Type | Eponym |
|---|---|
| Acute suppurative | Bacterial |
| Subacute granulomatous | De Quervain's; viral |
| Chronic autoimmune | Hashimoto's; anti-TPO antibodies |
| Fibrosing sclerosing | Riedel's thyroiditis |
| Chronic specific | TB, syphilis |
E. Miscellaneous / Rare
- Amyloid goitre
- Thyroid cysts
- Ectopic thyroid
PART II: Multinodular Goitre (MNG)
Definition
- Synonyms: Adenoparenchymatous goitre, nodular goitre, colloid nodular goitre
- MNG occurs in both endemic (iodine-deficient) and sporadic forms
- Important: Approximately 50% of patients presenting with a "solitary nodule" actually have MNG on ultrasound
Epidemiology
- Age: Endemic areas: 20-30 years; Sporadic: 30-40 years (nodules generally appear later and patients may be unaware till late 40s-50s)
- Sex: Females >> Males (6:1) - due to oestrogen receptors in thyroid tissue
- Incidence of sporadic MNG: ~5% in iodine-replete populations; increases with age
Pathogenesis
Step 1: Initial Stimulus (Deficiency of Thyroid Hormone)
- Any cause of deficient thyroid hormone synthesis → ↑ TSH secretion from anterior pituitary
- Main causes: Iodine deficiency (endemic), goitrogens (Brassica family vegetables, cassava), dyshormonogenesis (enzyme defects), physiological states (puberty, pregnancy)
Step 2: Diffuse Hyperplasia (Phase I)
- Elevated TSH → uniform stimulation of all follicular cells
- Follicular cell hypertrophy and hyperplasia → diffuse, soft enlargement of the entire gland
- Increased vascularity
- Histology: Tall columnar epithelium, minimal colloid, papillary projections
Step 3: Colloid Involution (Phase II)
- When hormone demand normalises (e.g., after pregnancy) or iodine supply improves → TSH falls
- Stimulated follicles involute → fill with colloid
- Follicle epithelium flattens to cuboidal
- Gland enlarges further but softer (colloid-filled follicles)
Step 4: Nodule Formation - Key Pathogenetic Mechanism
- Repeated cycles of hyperplasia and involution are not uniform throughout the gland
- Different follicular cells have different sensitivities to TSH and growth factors (heterogeneous response)
- Some follicular cell clones have a growth advantage (due to acquired genetic mutations similar to those in adenomas, including activating mutations in the TSH receptor signaling pathway)
- These clones proliferate autonomously → form discrete nodules
- Both polyclonal and monoclonal nodules coexist within the same MNG:
- Polyclonal nodules = hyperplastic areas from general TSH stimulation
- Monoclonal nodules = autonomous clonal proliferation (true adenomatous nodules)
- The heterogeneous structural and functional response produces characteristic nodularity
Step 5: Secondary Degenerative Changes
- Areas of haemorrhage (from rupture of stretched blood vessels) → cystic change, pain, sudden enlargement
- Fibrosis and scarring between nodules
- Calcification of old haemorrhagic/necrotic areas → may mimic carcinoma on imaging
- Cyst formation from liquefaction of colloid/haemorrhage
- Inactive nodules accumulate over time; most nodules eventually become non-functional
Morphology (Gross and Microscopic)
- Multilobulated, asymmetrically enlarged gland
- Can reach weights of >2000 g (enormous!)
- Pattern of enlargement is unpredictable - often one lobe much larger than the other
- May extend behind sternum (substernal/retrosternal goitre)
- Occasionally a single dominant nodule stands out mimicking a solitary tumour
- Cut surface: Irregular nodules with brown gelatinous colloid, areas of haemorrhage, fibrosis, cysts, calcification
- Follicles of varying sizes - some hugely distended with colloid, others showing cellular hyperplasia
- Colloid-rich follicles lined by flattened/cuboidal inactive epithelium (inactive areas)
- Areas of follicular hyperplasia with columnar cells
- Degenerative changes: Haemorrhage, fibrosis, calcification, cystic change
- No prominent capsule between nodules and residual parenchyma (unlike true adenoma - which has a complete capsule)
- Histological term: "Follicular nodular disease"
Clinical Features
Symptoms
- Slowly enlarging, painless lump in the neck - most common presentation
- May have been present for many years before the patient seeks attention
- Cosmetic concern
- Predominantly in the female
- Due to haemorrhage into an inactive nodule - characteristic feature of MNG
- Tender, tense nodule appears suddenly
- May cause acute airway embarrassment → emergency tracheostomy may be needed
- Dyspnoea (breathlessness) - tracheal compression or deviation; worse in particular neck positions
- Stridor - whistling noise when air passes through narrowed trachea
- Dysphagia - oesophageal compression (less common - oesophagus is muscular and can be displaced)
- Hoarseness - RLN compression (rare in benign MNG; if present, suspect malignancy)
- Venous engorgement - superior vena cava syndrome from retrosternal extension
- Pemberton's sign - flushing + venous engorgement of face/neck when both arms raised above head (indicates thoracic inlet obstruction from retrosternal extension)
- Cardiovascular symptoms predominate: palpitations, ectopic beats, atrial fibrillation, cardiac failure
- Develops gradually in long-standing MNG
- No eye signs (absent in secondary thyrotoxicosis)
- In very long-standing MNG (age 60-70 years): most nodules become inactive → gradual thyroid failure → myxoedema
Signs
- Asymmetrically enlarged thyroid with palpable nodules
- Surface: Smooth and nodular (not smooth and uniform as in Graves')
- Consistency: Variable - soft (colloid-filled), firm (hyperplastic), or hard (tense haemorrhagic/calcified nodules)
- Moves upward on deglutition (confirms thyroid origin)
- No bruit or thrill (unlike primary toxic goitre)
- Tracheal deviation visible/palpable in large goitres
- Pemberton's sign positive if retrosternal extension
- Signs of secondary thyrotoxicosis if toxic MNG: irregular pulse (AF), signs of cardiac failure
- No eye signs (differentiates from primary thyrotoxicosis)
Investigations
| Investigation | Finding / Purpose |
|---|---|
| Serum TSH | Normal (euthyroid MNG); suppressed if toxic MNG |
| Free T3, Free T4 | Normal; elevated if toxic |
| Thyroid autoantibodies (anti-TPO) | To differentiate from Hashimoto's thyroiditis (may coexist) |
| Thyroid USG (gold standard) | Multiple nodules of varying size and echogenicity; cystic/solid; calcification; vascular pattern; identifies dominant nodule for FNAC |
| FNAC | Required only for dominant nodule with suspicious USG features; NOT for all nodules |
| Radioiodine scan (¹²³I/⁹⁹ᵐTc) | Patchy, irregular uptake; hot and cold areas; useful to identify toxic nodule in secondary thyrotoxicosis |
| CT/MRI neck and chest | For substernal extension assessment, tracheal compression, surgical planning; essential if goitre extends below clavicles |
| X-ray neck (soft tissue) | Tracheal deviation/compression; calcification in goitre |
| Barium swallow | Oesophageal displacement (if dysphagia prominent) |
| Spirometry/flow-volume loop | Fixed or variable airway obstruction from tracheal compression |
| ECG | Atrial fibrillation in toxic MNG |
Complications of Multinodular Goitre
| Complication | Details |
|---|---|
| Haemorrhage into nodule | Sudden pain + rapid enlargement; may cause acute airway obstruction (emergency tracheostomy) |
| Secondary thyrotoxicosis | In ~25% of cases; Jöd-Basedow phenomenon (after iodine load/contrast/amiodarone) |
| Tracheal compression | Progressive or acute (haemorrhage); retrosternal extension worsens this |
| Malignant transformation | Increased incidence of follicular carcinoma in endemic areas; carcinoma can reside within MNG; dominant/rapidly growing nodule must be investigated |
| Myxoedema (hypothyroidism) | Late stage; most nodules become inactive |
| Superior vena cava (SVC) obstruction | Retrosternal extension |
| Calcification | May simulate carcinoma on imaging |
Management
A. Expectant / Observation (Small, Asymptomatic MNG)
- Most patients with MNG are asymptomatic and do NOT require treatment
- More than 50% of benign nodules regress over 10 years
- Follow-up: Periodic TFTs + USG every 6-12 months
- FNAC only for suspicious nodules (not all nodules)
B. Medical Treatment
- Mechanism: Suppresses TSH → removes growth stimulus → may reduce goitre size
- Dose: 0.15-0.2 mg (150-200 µg) daily
- Effective only in early hyperplastic stage (nodular stage is largely irreversible)
- Trials show goitre size reduction in ~30% of patients
- Drawbacks: Need for lifelong suppression; subclinical hyperthyroidism effects on heart (AF) and bone (osteoporosis); NOT curative
- For endemic iodine-deficient hyperplastic goitre (early stage)
- Iodised salt is the primary public health intervention
- Caution: Excess iodine in long-standing MNG can precipitate hyperthyroidism (Jöd-Basedow phenomenon)
- For symptomatic control if secondary thyrotoxicosis develops
- Propranolol 40-80 mg TDS until euthyroid with antithyroid drugs
- Used if secondary thyrotoxicosis develops
- Only temporize - recurrence is certain on stopping (autonomous nodules not suppressible)
- Pre-operative preparation before thyroidectomy
C. Radioactive Iodine (¹³¹I) Therapy
- Can reduce goitre size by up to 50% over 1 year
- Increasingly used in many countries as alternative to surgery
- Indications: Elderly patients unfit for surgery; small-moderate toxic MNG; patient preference
- Limitations:
- Effect is gradual; not suitable for large goitres
- Acute transient thyroiditis may temporarily worsen symptoms
- Ineffective for very large goitres
- May precipitate hypothyroidism (often requires lifelong thyroxine)
- Contraindicated in pregnancy, breastfeeding, suspected malignancy, active ophthalmopathy
D. Surgical Treatment (Thyroidectomy) - Definitive Treatment
- Local compressive symptoms - dyspnoea, stridor, dysphagia not responding to other treatment
- Substernal/retrosternal extension (often presents with compressive symptoms)
- Suspected or confirmed malignancy - dominant nodule, rapidly growing nodule, suspicious FNAC
- Toxic MNG with compressive symptoms (surgery + RAI both effective)
- Cosmetic disfigurement - patient finds goitre unsightly
- Failure of medical management - continued growth despite thyroxine
- Sudden haemorrhage causing acute airway compromise
- Patient preference (assuming acceptable surgical candidate)
| Situation | Preferred Procedure |
|---|---|
| Bilateral MNG | Total thyroidectomy (now preferred) - eliminates regrowth and cancer risk |
| Bilateral MNG (historically) | Subtotal thyroidectomy - unacceptably high recurrence >50% |
| Asymmetric unilateral dominant MNG | Total lobectomy of dominant side; no intervention on less-affected side (avoids re-operation risk) |
| Bilateral with unequal involvement | Dunhill procedure - total lobectomy one side + subtotal of other; most surgeons now prefer total thyroidectomy |
| Substernal goitre | Standard cervical incision (most cases); sternotomy only for goitres below aortic arch or posterior extension |
| Younger patients | Total thyroidectomy preferred to avoid difficult re-operation for recurrence |
- Antithyroid drugs (carbimazole) → render euthyroid (6-8 weeks)
- Beta-blockers (propranolol) → pulse <80/min
- Lugol's iodine × 10-14 days → reduce vascularity
- If total thyroidectomy: Lifelong levothyroxine replacement
- Monitor for complications: tetany (Ca²⁺, PTH), hoarseness (RLN), haemorrhage
- Follow-up: TFTs at 6 weeks, then annually
| Complication | Time | Management |
|---|---|---|
| Reactionary haemorrhage | 0-24 hrs | Re-explore; may need urgent bedside wound opening to relieve airway compression |
| Tetany/hypocalcaemia | 24-72 hrs | IV calcium gluconate; check PTH and Ca²⁺ |
| RLN injury (hoarseness) | Immediate | Unilateral: usually recovers; bilateral: tracheostomy |
| Hypothyroidism | Weeks-months | Levothyroxine replacement |
| Thyroid storm | Intra/post-op | If inadequate pre-op preparation |
| Recurrence | Months-years | More likely with subtotal resection |
Summary of MNG Management Algorithm
Multinodular Goitre diagnosed
│
┌─────┴─────┐
Asymptomatic Symptomatic/Complicated
│ │
Observe Assess:
TFTs + USG ┌──────────┼──────────┐
annually Toxic Compressive Malignancy
│ suspected │
ATDs + Surgery/RAI Surgery
Beta-Bl (large goitre → Surgery preferred)
│
Euthyroid
│
RAI or Surgery (definitive)