Transport of oxygen
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
I have comprehensive content. Now let me compile the full answer.
Transport of Oxygen
Source: Guyton and Hall Textbook of Medical Physiology
Overview
Oxygen (O2) diffuses from the alveoli into pulmonary capillary blood and is then transported to the tissues almost entirely in chemical combination with hemoglobin. Hemoglobin allows blood to carry 30-100 times as much O2 as could be dissolved in plasma water alone. The remaining ~3% travels dissolved in plasma.
1. Diffusion From Alveoli to Pulmonary Blood
Transport relies on partial pressure gradients:
- Alveolar PO2 = ~104 mm Hg
- Venous blood entering pulmonary capillary PO2 = ~40 mm Hg
- Initial diffusion gradient = 64 mm Hg
Blood equilibrates to nearly 104 mm Hg by the time it has traveled only one-third of the length of the pulmonary capillary - this gives a large safety margin during exercise, when capillary transit time is cut by more than half yet the blood still becomes fully saturated.
2. Forms of Oxygen in Blood
| Form | Amount (normal arterial) | Notes |
|---|---|---|
| Bound to hemoglobin (HbO2) | ~19.4 mL/100 mL blood | 97% of total O2 |
| Dissolved in plasma | ~0.29 mL/100 mL blood | ~3% of total O2 |
Oxygen-carrying capacity of hemoglobin:
- Normal Hb = 15 g/100 mL blood
- Each gram of Hb binds max 1.34 mL O2
- Total capacity = 15 × 1.34 = ~20 mL O2 / 100 mL blood (= 20 volume %)
3. The Oxygen-Hemoglobin Dissociation Curve
The sigmoid shape is central to understanding O2 delivery:
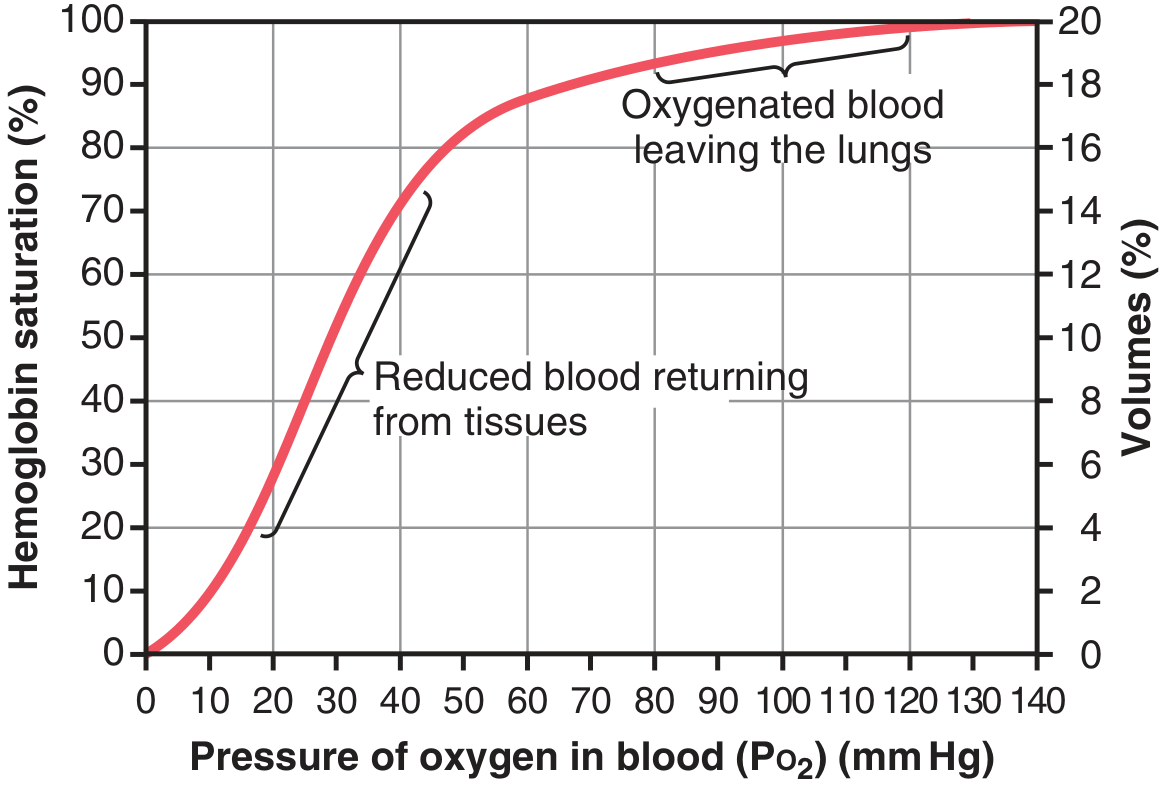
Figure 41.8 - Guyton & Hall: Oxygen-hemoglobin dissociation curve
Key reference points:
| Location | PO2 (mm Hg) | Hb Saturation | O2 content |
|---|---|---|---|
| Arterial (leaving lungs) | 95 | 97% | ~19.4 mL/100 mL |
| Venous (returning from tissues) | 40 | 75% | ~14.4 mL/100 mL |
| Heavy exercise (muscle) | 15 | ~22% | ~4.4 mL/100 mL |
Under normal resting conditions, ~5 mL of O2 is delivered per 100 mL blood. During heavy exercise, this rises to ~15 mL per 100 mL blood.
4. Factors Shifting the Dissociation Curve
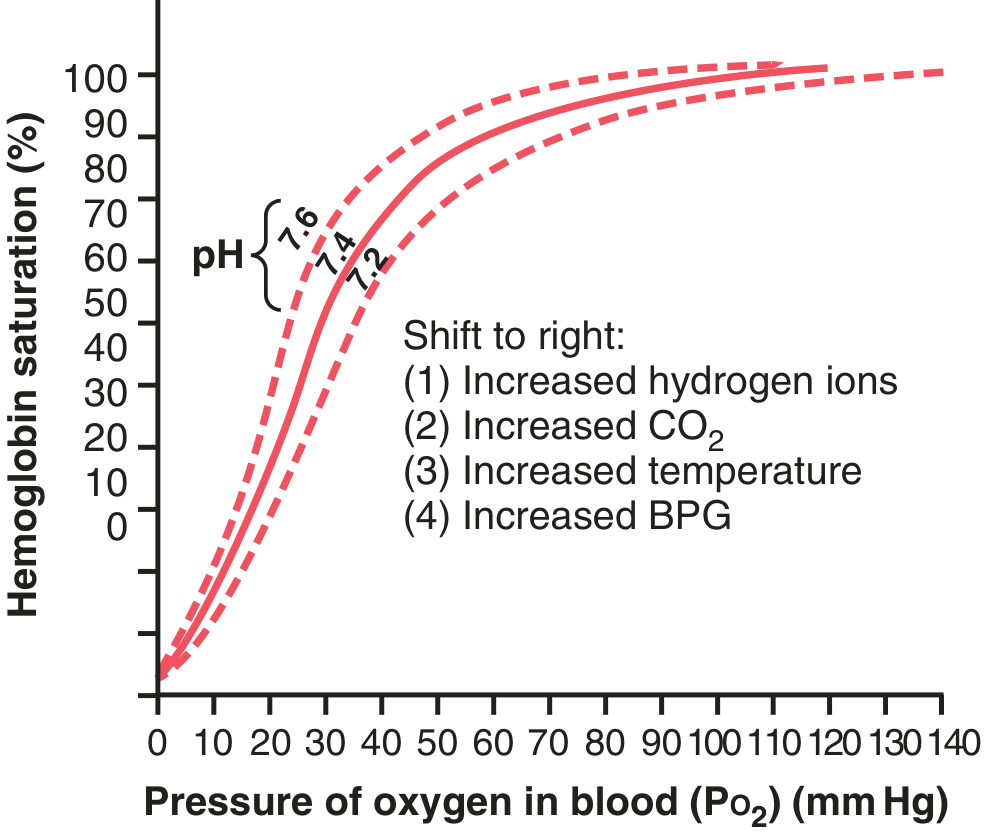
Figure 41.10 - Guyton & Hall: Shift caused by increased H+ (decreased pH), increased CO2, temperature, and 2,3-BPG
Rightward shift (Bohr Effect) - reduces O2 affinity, enhances tissue delivery:
- Increased H+ (lower pH / acidosis)
- Increased CO2
- Increased temperature
- Increased 2,3-bisphosphoglycerate (2,3-BPG)
Leftward shift - increases O2 affinity (better loading in lungs, less delivery to tissues):
- Decreased H+, CO2, temperature
- Decreased 2,3-BPG
- Fetal hemoglobin (HbF) - naturally left-shifted to pull O2 from maternal blood
During exercise, all four rightward-shift factors operate simultaneously in muscle capillaries (CO2 rises, pH falls, temperature rises, 2,3-BPG increases), forcing extra O2 delivery to active muscle even when 70% of O2 has already been extracted.
5. Hemoglobin as a Tissue PO2 Buffer
Hemoglobin has a remarkable buffering role that keeps tissue PO2 within a narrow range (~15-40 mm Hg), regardless of major changes in alveolar PO2:
- When alveolar PO2 falls to 60 mm Hg (high altitude), Hb is still 89% saturated - tissues receive nearly the same amount of O2
- When alveolar PO2 rises to 500 mm Hg (hyperbaric O2), Hb saturation can only reach 100% (3% above normal) - tissue PO2 barely changes
- This is because the flat upper portion of the dissociation curve absorbs large alveolar PO2 changes with minimal effect on saturation
6. Oxygen in the Dissolved State
Henry's Law governs dissolved O2:
- At normal alveolar PO2 of 104 mm Hg → 0.29 mL O2 / 100 mL blood dissolves
- Breathing 100% O2 at 1 atm → ~0.5 mL dissolved O2
- Breathing 100% O2 at 4 atm (hyperbaric) → ~6 mL - enough to sustain life without hemoglobin
This is the basis for hyperbaric oxygen therapy.
7. Cellular Oxygen Utilization
Once O2 diffuses into cells:
- Only 1 mm Hg intracellular PO2 is needed for normal oxidative metabolism - O2 availability is rarely rate-limiting
- The actual rate of O2 usage is controlled by the concentration of ADP (energy demand), not by O2 supply (as long as PO2 > 1 mm Hg)
- As ATP is used → ADP rises → drives oxidative phosphorylation → O2 consumption increases
Summary Flow
Alveoli (PO2 104 mmHg)
↓ diffusion
Pulmonary capillary blood → 97% Hb saturation
↓ carried by hemoglobin (97%) + dissolved (3%)
Systemic arteries (PO2 ~95 mmHg)
↓ diffusion gradient
Tissue capillaries → O2 released as PO2 falls to ~40 mmHg
↓
Cells → oxidative metabolism (needs only >1 mmHg intracellular PO2)
↓
Venous blood (PO2 ~40 mmHg, 75% Hb saturation)
↓ returns to lungs
- Guyton and Hall Textbook of Medical Physiology, Chapter 41 (O2 and CO2 Transport in Blood)
Cerebellum
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have all the content needed for a thorough answer. Let me compile it now.
The Cerebellum
Sources: Ganong's Review of Medical Physiology; Costanzo Physiology; Guyton and Hall; Bradley and Daroff's Neurology in Clinical Practice
Overview
The cerebellum ("little brain") sits in the posterior fossa below the occipital lobe, astride the main sensory and motor systems of the brainstem. Despite weighing only ~10% as much as the cerebral cortex, its surface area is ~75% of the cerebral cortex, due to dense folding into folia (leaf-like ridges) separated by fissures.
The cerebellum does not initiate movement. Instead it:
- Regulates rate, range, force, and direction of ongoing movements (synergy)
- Compares motor intention vs. performance and corrects errors
- Controls balance and eye movements
- Participates in motor learning
Gross Anatomy and Lobes
The cerebellum is divided by two transverse fissures:
| Fissure | Divides |
|---|---|
| Posterolateral fissure | Flocculonodular lobe from the rest |
| Primary fissure | Anterior lobe from posterior lobe |
- The vermis is the midline strip; it is divided into 10 lobules (I-X)
- Cerebellar hemispheres flank the vermis on each side
- Flocculus + nodulus = flocculonodular lobe
Functional Divisions
Three functional subdivisions exist, each with distinct inputs, outputs, and roles:
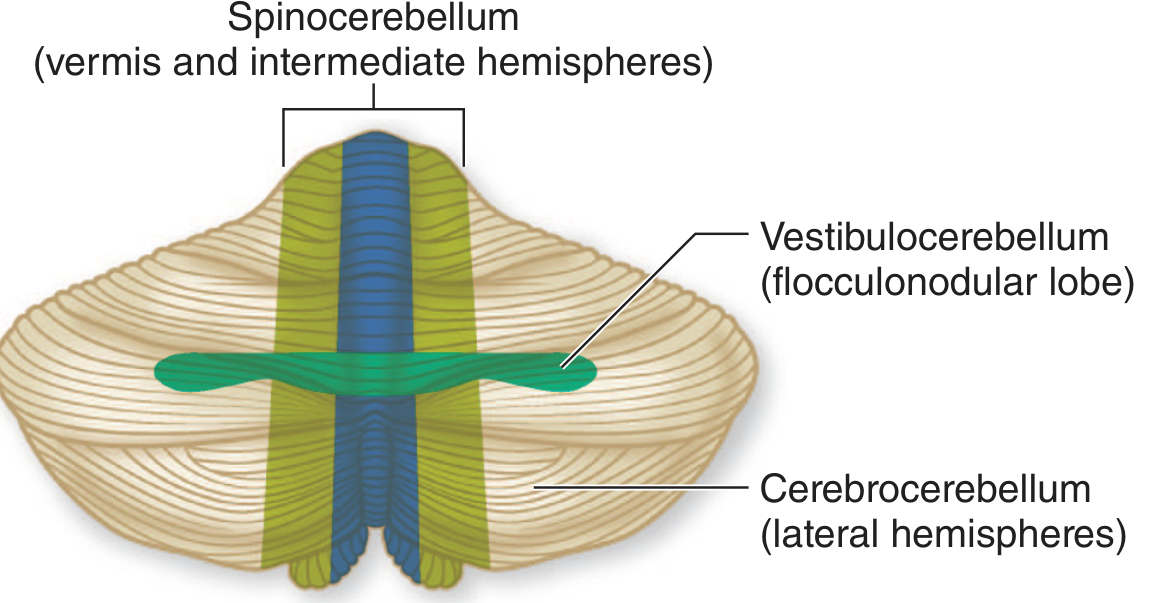
Functional divisions of the cerebellum (Adams and Victor's Principles of Neurology)
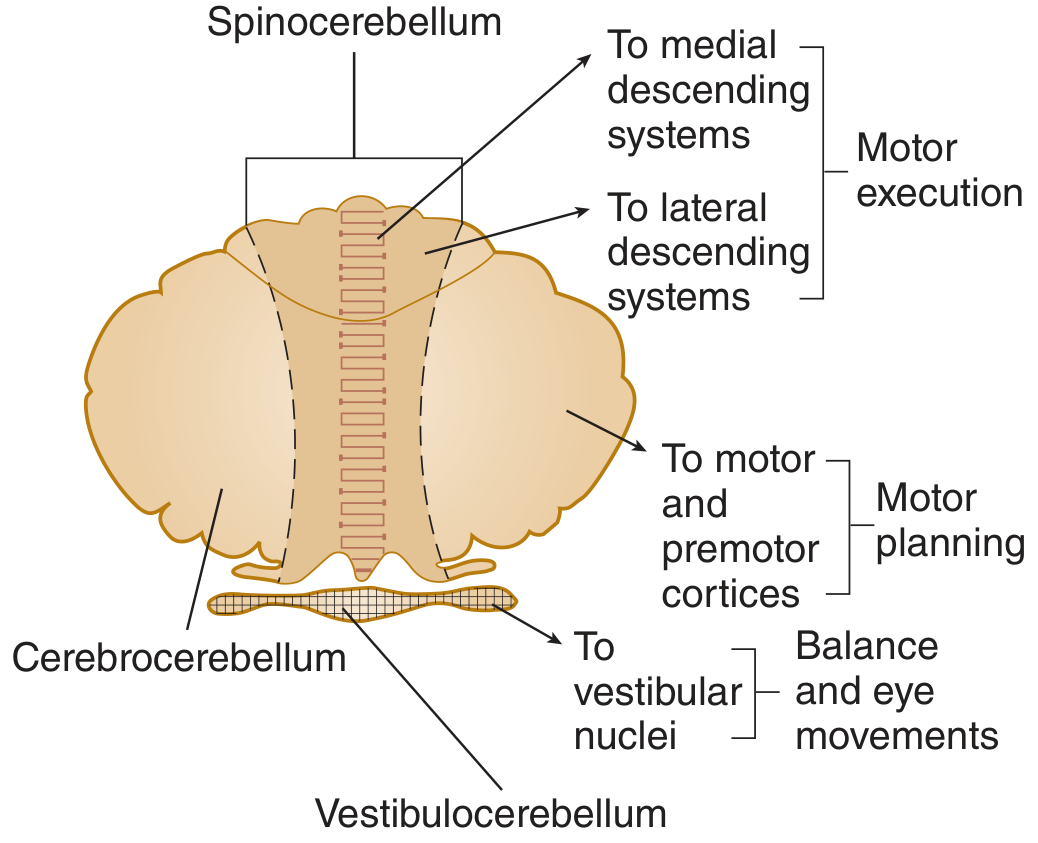
Figure 12-19 - Ganong's Review of Medical Physiology: Functional divisions and their projections
| Division | Structure | Input | Output | Function |
|---|---|---|---|---|
| Vestibulocerebellum | Flocculonodular lobe | Vestibular, visual | Directly to vestibular nuclei | Balance, eye movements |
| Spinocerebellum | Vermis + medial hemispheres | Proprioception from spinal cord + motor cortex copy | Via fastigial/interpositus nuclei → brainstem | Synergy of ongoing movement; axial + limb coordination |
| Cerebrocerebellum (Pontocerebellum) | Lateral hemispheres | Cerebral cortex via pons | Via dentate nucleus → thalamus (VL) → motor cortex | Motor planning and programming |
Cerebellar Peduncles
The cerebellum communicates through three pairs of peduncles:
| Peduncle | Fibers | Key Connections |
|---|---|---|
| Superior cerebellar peduncle | Mainly efferent | Deep nuclei → red nucleus + thalamus |
| Middle cerebellar peduncle | Only afferent | Contralateral pontine nuclei → cerebellum |
| Inferior cerebellar peduncle | Mixed afferent + efferent | Spinal cord + brainstem → cerebellum; cerebellum → vestibular nuclei |
Cerebellar Cortex: Layers and Cells
The cortex has 3 layers containing 5 neuron types:
Layers (outer to inner)
- Molecular layer - basket cells, stellate cells, Purkinje cell dendrites, granule cell axons (parallel fibers)
- Purkinje cell layer - single layer of Purkinje cells (the sole cortical output)
- Granular layer - granule cells, Golgi II cells, glomeruli (synaptic islands)
Key Neurons
| Cell | Role | Neurotransmitter |
|---|---|---|
| Purkinje cell | Sole output of cortex; enormous dendritic arbor spanning the molecular layer | GABA (inhibitory) |
| Granule cell | Receives mossy fiber input; sends axons up → bifurcate into parallel fibers | Glutamate (excitatory) |
| Basket cell | Inhibits Purkinje cells | GABA |
| Stellate cell | Inhibits Purkinje cells | GABA |
| Golgi II cell | Inhibits granule cells (feedback) | GABA |
Key rule: All cerebellar interneurons are inhibitory EXCEPT granule cells. All Purkinje cell output is inhibitory (GABA).
Input Systems: Mossy Fibers vs. Climbing Fibers
| Feature | Mossy Fibers | Climbing Fibers |
|---|---|---|
| Origin | Spinocerebellar, pontocerebellar, vestibulocerebellar tracts | Inferior olivary nucleus (contralateral) |
| First synapse in cortex | Granule cells (in glomeruli) | Directly on Purkinje cell dendrites |
| Ratio to Purkinje cells | Each Purkinje cell receives ~250,000 parallel fiber inputs | Each Purkinje cell receives input from only one climbing fiber |
| Effect on Purkinje cell | Simple spikes | Complex spikes (burst of action potentials) |
| Role in learning | General motor signaling | Motor learning and "error correction" |
Both systems also send collaterals directly to the deep cerebellar nuclei.
Output: Deep Cerebellar Nuclei
The deep nuclei (from medial to lateral):
- Fastigial nucleus - receives from vermis → projects to vestibular nuclei and brainstem (axial/trunk control)
- Globose + Emboliform nuclei (= Interpositus nucleus) - receives from intermediate hemisphere → red nucleus + brainstem (limb coordination)
- Dentate nucleus (largest) - receives from lateral hemisphere → thalamus (VL) → motor and premotor cortex (motor planning)
Purkinje cells inhibit the deep nuclei. Deep nuclei tonically fire and drive motor output; Purkinje cell inhibition shapes and modulates this tonic output.
Afferent Tracts Summary
| Tract | Carries |
|---|---|
| Vestibulocerebellar | Vestibular impulses (labyrinths + vestibular nuclei) |
| Dorsal spinocerebellar | Proprioception from lower limbs/trunk (ipsilateral) |
| Ventral spinocerebellar | Proprioception from upper + lower limbs (crossed) |
| Cuneocerebellar | Proprioception from upper limb + upper thorax |
| Pontocerebellar | Cortical motor commands (via pontine nuclei) |
| Olivocerebellar | Whole-body proprioception via inferior olive → climbing fibers |
Cerebellar Disease: Signs
Lesions produce ipsilateral signs (cerebellum does not decussate to the other side before projecting).
| Sign | Description |
|---|---|
| Ataxia | Incoordination of limbs or gait - errors in rate, range, force, direction |
| Intention tremor | Tremor that worsens as limb approaches target (perpendicular to movement direction) |
| Dysmetria | Overshoot (hypermetria) or undershoot (hypometria) of target |
| Dysdiadochokinesia | Inability to perform rapid alternating movements |
| Rebound phenomenon | Inability to stop a movement when resistance is suddenly removed |
| Hypotonia | Decreased muscle tone |
| Nystagmus | With flocculonodular lobe lesions |
Localization rule:
- Midline (vermis) lesion → truncal/gait ataxia
- Lateral hemisphere lesion → ipsilateral limb ataxia
- Flocculonodular lobe → nystagmus, balance problems, vertigo
The Cerebellum and Motor Learning
As a motor skill is practiced and learned, activity shifts from prefrontal areas toward the parietal and motor cortex and the cerebellum. The proposed mechanism:
- A climbing fiber (from inferior olive) fires strongly during a movement error - producing a complex spike in Purkinje cells
- This spike causes long-term depression (LTD) of the specific mossy fiber-granule-Purkinje cell synapse that was active at the same time
- Over many repetitions, this weakens the "wrong" Purkinje responses and smooths out the movement
Selective lesions of the inferior olive abolish this learning. This makes the olivocerebellar pathway the likely substrate for procedural/motor memory acquisition.
Summary Circuit
Motor cortex command
↓ (via pons → mossy fibers)
Granule cells → parallel fibers → Purkinje cells (+ basket, stellate)
↓ (GABA - inhibitory)
Deep cerebellar nuclei
(tonically excitatory)
↓
Thalamus (VL) → Motor cortex [cerebrocerebellum]
Red nucleus / brainstem [spinocerebellum]
Vestibular nuclei [vestibulocerebellum]
Inferior olive → climbing fibers → Purkinje cells (1:1 ratio, complex spikes)
[error correction and motor learning]
This is a shared conversation. Sign in to Orris to start your own chat.